When Gas Replaces the Liver: A Rare Case of Successfully Treated Emphysematous Hepatitis
Dirin Ukwade, Hasan S. Raza, Omar T. Ahmed, James S. Love, Maria El Gemayel, Jamie L. Berkes

TL;DR
A rare case of emphysematous hepatitis was successfully treated with antibiotics and drainage, offering hope for better outcomes.
Contribution
This is the second reported survival case using percutaneous drainage for emphysematous hepatitis.
Findings
The patient had uncontrolled diabetes and was diagnosed with emphysematous hepatitis.
Treatment with antibiotics and percutaneous drainage led to successful recovery.
The case highlights the potential of minimally invasive treatment for this rare condition.
Abstract
Emphysematous hepatitis is a rare condition characterized by the presence of gas within the hepatic parenchyma. Only a limited number of cases have been reported, with most patients experiencing poor outcomes and median survival time ranging from hours to days after diagnosis. We present a case of a patient with uncontrolled diabetes, abdominal pain, and fatigue who was found to have emphysematous hepatitis. The patient was successfully treated with antibiotics and percutaneous drainage without the need for surgical intervention. This case represents the second reported instance of survival following percutaneous drainage, highlighting the potential efficacy of this minimally invasive approach.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
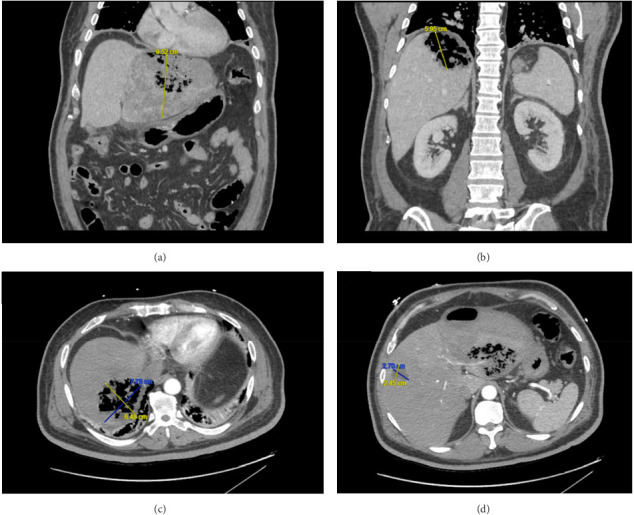 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Disease Case Reports and Treatments · Amoebic Infections and Treatments · Abdominal vascular conditions and treatments
1. Introduction
Emphysematous hepatitis (EH) was first described by Blachar et al. in 2002 as a condition characterized by hepatic parenchymal destruction with the presence of gas on imaging [1]. The clinical presentation of EH is variable, with common symptoms including fever and abdominal pain. In severe cases, patients may present with confusion and hypotension. Laboratory findings often reveal elevated liver enzymes and leukocytosis, indicative of an underlying infection. Due to its rarity and nonspecific presentation, EH requires a high index of suspicion for timely diagnosis. Early identification is critical, as the disease is associated with high mortality, with most reported cases resulting in fatality within hours to days of diagnosis [1–14]. Here, we present the second known case of EH successfully treated with antibiotics and percutaneous drainage.
2. Case Report
A 59-year-old male with a medical history significant for uncontrolled Type 2 diabetes mellitus, hyperlipidemia, and hypertension presented to an outside hospital with a 4-day history of abdominal pain and fatigue. Initial laboratory studies revealed leukocytosis (12.3 × 10^3^/L), elevated liver enzymes (aspartate aminotransferase [AST] 399 U/L, alanine aminotransferase [ALT] 339 U/L, and alkaline phosphatase [ALP] 268 U/L), total bilirubin of 1.4 mg/dL, lipase of 54 U/L, and an international normalized ratio (INR) of 1.2. During his hospital course, his white blood cell count peaked at 18.9 × 10^3^/L, and his AST and ALT levels rose to 1650 and 1321 U/L, respectively.
The patient was transferred to our institution for evaluation for liver transplantation. Further hepatology workup included viral hepatitis serologies, acetaminophen level, and antinuclear antibodies (ANA), which were all negative. Broad-spectrum antibiotics were initiated empirically. Blood cultures subsequently grew Klebsiella pneumoniae. A contrast-enhanced computed tomography (CT) scan of the abdomen revealed extensive gas-forming collections in both the left and right hepatic lobes, consistent with EH. A focal hypodensity in the mid-right hepatic lobe was also noted, likely representing an additional site of infection (Figure 1).
Given the previously identified collections on CT, the decision was made to pursue a CT-guided percutaneous aspiration and drainage of the hepatic collections to also assess for possible concomitant pyogenic liver abscess (PLA). Cultures of drained fluid also grew K. pneumoniae. The drains remained in place for approximately 2 months, with interval imaging demonstrating gradual resolution of the collections.
3. Discussion
Since the initial description by Blachar et al. in 2002, EH has remained an exceedingly rare condition, with only a handful of cases reported in the literature [1, 6, 15]. The majority of patients with EH have a history of uncontrolled diabetes mellitus, as seen in our case.
The pathophysiology of EH remains poorly understood. Current evidence suggests that EH represents a necrotizing infection of the liver parenchyma, with the most commonly implicated organisms being K. pneumoniae, Clostridium perfringens, Escherichia coli, and Enterococcus faecalis. The pathogenesis has been proposed to possibly be similar to that of other emphysematous infections, where the high glucose tissue concentration that is seen in diabetic patients attracts organisms that then ferment the sugar into carbon dioxide and leads to the production of gas within the hepatic tissue [13]. However, this hypothesis does not fully explain cases occurring in nondiabetic individuals, suggesting that additional factors, such as impaired hepatic perfusion or immunodeficiency, may play a role.
The diagnosis of EH relies on imaging, particularly contrast-enhanced CT, which demonstrates gas within the liver parenchyma. The condition is often associated with compromised arterial and portal venous blood supply, resulting in infarcted liver segments that appear as nonenhancing, hypodense areas on imaging [16]. It is also important to differentiate EH from gas-forming PLA, which also presents with hepatic gas. However, PLA is characterized by pus-filled fluid collections rather than parenchymal destruction [1].
Timely diagnosis and intervention are critical in EH, as the condition is associated with high mortality. Most reported cases have resulted in death within hours to days despite prompt antibiotic therapy (Table 1) [1–14]. To date, only seven cases of survival have been documented, including the present case [15–20]. In all surviving cases, antibiotic therapy was combined with either surgical or percutaneous drainage (Table 1). Notably, only two cases (including ours) have reported survival following antibiotic therapy and percutaneous drainage alone [18]. While some authors advocate for surgical drainage as the definitive treatment for EH [16, 19], others have noted that the available data are too sparse to establish the superiority of surgical over percutaneous drainage [17]. Our case underscores the potential efficacy of percutaneous drainage as a minimally invasive treatment option and highlights the importance of early intervention in this rare and life-threatening condition. In addition to identifying a rare case of EH that was successfully treated, our case also shows that further research is needed to establish standardized treatment guidelines for EH.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blachar A. Federle M. P. Brancatelli G. Acute Fulminant Hepatic Infection Causing Fatal “Emphysematous Hepatitis”: Case Report Abdominal Imaging 200227218819010.1007/s 00261-001-0067-y 2-s 2.0-003648943511847579 · doi ↗ · pubmed ↗
- 2Bofill A. Marco F. Emphysematous Hepatitis New England Journal of Medicine 202138517 p. e 5810.1056/NEJ Micm 210877934670046 · doi ↗ · pubmed ↗
- 3Lin Y. S. Wang W. S. Chen M. J. Emphysematous Changes of the Liver Gastroenterology 2012142221341410.1053/j.gastro.2011.04.0642-s 2.0-8486294480322192434 · doi ↗ · pubmed ↗
- 4Calderon H. Serfin J. 13-Hour Progression of Emphysematous Hepatitis as Depicted on Repeat Computerized Tomography Journal of Surgical Case Reports 202020204 p. rjaa 08910.1093/jscr/rjaa 089PMC 719188332373313 · doi ↗ · pubmed ↗
- 5Al Khatib A. Duboc H. Soliman H. Emphysematous Hepatitis due to Clostridiumsepticum Clinical Gastroenterology and Hepatology 2025234 p. A 3210.1016/j.cgh.2024.08.01339186966 · doi ↗ · pubmed ↗
- 6Ayoub C. Oula A. Nabila E. Asmae O. A. Siham A. R. Emphysematous Hepatitis: A Case Report and Review of Literature Radiology Case Reports 202419126629663210.1016/j.radcr.2024.09.05939403077 PMC 11472012 · doi ↗ · pubmed ↗
- 7Miranda G. Dionísio A. C. Azevedo C. Fulminant Emphysematous Hepatitis–A Rare Cause of Septic Shock European Journal of Case Reports in Internal Medicine 202075 p. 00153910.12890/2020_001539 PMC 721383632399443 · doi ↗ · pubmed ↗
- 8Tekinhatun M. YavaşH. G. Emphysematous Hepatitis: A Rare Fatal Case Journal of Clinical Ultrasound 20245281235123910.1002/jcu.2376539007204 · doi ↗ · pubmed ↗