Pachymeningitis With Dural Vessel Dilatation in MOG Antibody–Associated Disease: A Case Report
Yunchen Huang, Yafei Song, Ding Liu, Yin Liu

TL;DR
A case report describes a rare manifestation of MOG antibody-associated disease involving pachymeningitis and dural vessel dilation, which improved with hormone therapy.
Contribution
This case expands the known imaging features of MOGAD by highlighting pachymeningitis with dural vessel dilation.
Findings
Pachymeningitis with dural vessel dilation was observed in a patient with MOGAD.
The condition improved significantly after hormone therapy.
This case broadens the imaging spectrum of MOGAD.
Abstract
Myelin oligodendrocyte glycoprotein (MOG) antibody–associated disease (MOGAD) is a novel inflammatory demyelinating disorder marked by heterogenous clinical and radiological manifestations. Pachymeningitis is a rare manifestation. An 18-year-old male was hospitalized with fever, dizziness, altered consciousness, and seizure attacks. Serum testing was positive for MOG antibodies. Diffuse pachymeningitis with prominent dural vessel dilation was observed prior to treatment, which markedly improved after hormone therapy. MOGAD pachymeningitis with dural vessel dilatation broadens the imaging spectrum of MOGAD.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
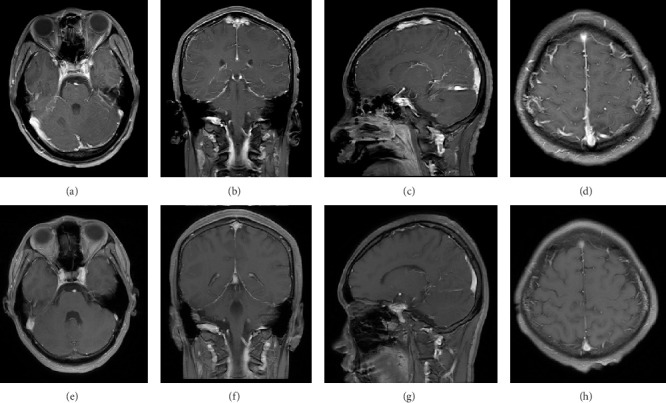 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIgG4-Related and Inflammatory Diseases · Vasculitis and related conditions · Otitis Media and Relapsing Polychondritis
1. Introduction
Myelin oligodendrocyte glycoprotein (MOG) antibody–associated disease (MOGAD) is a recently recognized inflammatory demyelinating disease mediated by antibodies against MOG [1]. Typical clinical manifestations include optic neuritis, myelitis, acute disseminated encephalomyelitis, brainstem encephalitis, cortical encephalitis, and aseptic meningitis [1–3]. Radiological features of MOGAD are similarly diverse, reflecting the clinical phenotype [1]. Pachymeningitis represents a rare imaging manifestation of MOGAD, and this report describes a case of MOGAD with pachymeningitis and prominent dural vessel dilatation.
2. Clinical Data
An 18-year-old male patient was admitted to the hospital with a 4-day history of fever and dizziness, followed by 2 days of altered consciousness and seizure attacks. The patient was sedated upon admission, with equal and round pupils that were reactive to light. His neck was supple. A lumbar puncture was performed on the day of admission. The cerebrospinal fluid (CSF) pressure was found to be 185 mmH_2_O, with CSF analysis revealing total protein of 1632 mg/L and glucose of 5.19 mmol/L. Oligoclonal bands were negative. CSF cytology indicated a total white blood cell count of 110 × 10^6^/L (67% lymphocytes and 11% neutrophils). Infection work-up revealed IgG positivity for Epstein–Barr virus, Mycoplasma pneumoniae, and Chlamydophila pneumoniae, while both blood and CSF bacterial cultures were negative. Serum autoantibodies, including ANCA, ANA, rheumatoid factor, anti-SSA, and anti-SSB, were negative. An MRI of the head performed on the second day of admission revealed diffuse linear dural thickening and enhancement with prominent dural vessel dilatation; however, no other parenchymal lesion was identified in the brain (Figures 1(a), 1(b), and 1(c)). The initial diagnosis was probable viral meningoencephalitis with secondary epilepsy. The patient was treated with acyclovir for antiviral therapy, along with valproic acid and levetiracetam for seizure control. However, live cell–based assays subsequently detected positive serum MOG antibodies at a titer of 1:100, while CSF MOG antibodies were negative. An additional serum IgG4 test was not found to be significant.
Following confirmation of the diagnosis of MOGAD, the patient was treated with high-dose intravenous methylprednisolone, 1,000 mg for the initial three days, followed by half the previous dose every 3 days, transitioning to oral prednisolone at 60 mg/day. On the fifth day of intravenous methylprednisolone therapy, the patient regained consciousness and remained seizure-free. A follow-up lumbar puncture performed after 1 week of hormone treatment revealed a CSF pressure of 150 mmH_2_O and a total protein of 351 mg/L. CSF cytology was negative, with a total white blood cell count of 1 × 10^6^/L (no neutrophils). A follow-up contrast-enhanced brain MRI on the 12^th^ day of hormone treatment demonstrated complete resolution of dural thickening, enhancement, and dural vessel dilatation (Figures 1(d), 1(e), and 1(f)). No spinal MRI was performed, as the patient exhibited no spinal or optic symptoms.
3. Discussion
According to the proposed diagnosis criteria of MOGAD, this patient exhibited a typical pattern of meningitis, as evidenced by infection-like symptoms, CSF findings, and a positive serum MOG antibody at the titer of 1:100. However, this case demonstrated pachymeningeal involvement, which was different from the leptomeningeal pattern primarily reported in previous studies on the aseptic meningitis type of MOGAD [2].
Based on anatomic location and embryological origin, meningitis of the central nervous system can be classified into two patterns, pachymeningitis (involving the dura and dura-arachnoid interface) and leptomeningitis (pia-subarachnoid) [4]. Leptomeningitis typically presents with signs of meningeal irritation, whereas pachymeningitis is generally associated with headache, cranial nerve symptoms, seizures, and ataxia. Notably, oligodendrocytes are not normally present in the dura mater, which may explain the rarity of pachymeningeal involvement in MOGAD. However, cases of heterotopic neuroglial tissues have been reported [5].
Similar to the cases reported by Ueno et al. [6] and Khaladkar et al. [7], pachymeningitis was the only radiological finding in this case. However, the diffuse pachymeningeal enhancement pattern and infectious features observed here were not described in those reports. Consistent with the findings in Ueno et al. [6], the pachymeningeal enhancement resolved completely following high-dose intravenous methylprednisolone. However, the MOGAD patient with bilateral Sturge–Weber syndrome reported by Michishita et al. [8] showed bilateral diffuse pachymeningeal enhancement after treatment, while the concurrent right leptomeningeal enhancement and a focal lesion of the right cerebellar hemisphere resolved completely. The possibility that the bilateral dural enhancement in that case was influenced by the Sturge–Weber syndrome cannot be excluded. Moreover, prominent dural vessel dilatation was observed in the present case, which was not previously reported in MOGAD.
The mechanism underlying pachymeningeal enhancement, particularly the diffuse type, remains poorly understood. Intracranial volume compensatory changes seen in intracranial hypotension, as well as increased vascularity or angiogenesis secondary to meningeal pathology or irritation, may contribute to this phenomenon [9]. It has also been suggested that the diffuse pachymeningeal enhancement may be related to periosteal pathology [9]. Recent studies indicate that the vessels between the cranial bone and dura may be important passages for neuroimmune surveillance [10]. In this case, heterotopic neuroglial tissues within dura mater may be responsible for the pachymeningeal enhancement, while the dilated dural vessels as well as the pachymeningeal enhancement may reflect communication between the cranial bone marrow and meninges, suggesting a periosteal involvement in MOGAD meningitis.
Furthermore, the patient underwent MRI examination following the lumbar puncture procedure, which has been associated with diffuse leptomeningeal enhancement due to cerebral hypotension after lumbar puncture [11]. However, the patient did not report any symptoms suggestive of cerebral hypotension.
In summary, MOGAD pachymeningitis, with or without dural vessel dilatation, broadens the imaging spectrum of MOGAD. The dural enhancement pattern and its pathophysiological mechanism in MOGAD warrant further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Banwell B. Bennett J. L. Marignier R. Diagnosis of Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease: International MOGAD Panel Proposed Criteria The Lancet Neurology 2023 March 22326828210.1016/S 1474-4422(22)00431-836706773 · doi ↗ · pubmed ↗
- 2Gu M. Mo X. Fang Z. Characteristics of Aseptic Meningitis-Like Attack-An Underestimated Phenotype of Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease Multiple Sclerosis and Related Disorders 2023 October 78p. 10493910.1016/j.msard.2023.10493937611382 · doi ↗ · pubmed ↗
- 3Ren B. Li S. Liu B. Zhang J. Feng Y. Anti-MOG Antibody-Associated Unilateral Cortical Encephalitis With Bilateral Meningeal Involvement: A Case Report Brain Sciences 2023 February 132p. 28310.3390/brainsci 13020283 PMC 995413736831826 · doi ↗ · pubmed ↗
- 4Kurokawa R. Kurokawa M. Isshiki S. Dural and Leptomeningeal Diseases: Anatomy, Causes, and Neuroimaging Findings Radio Graphics 2023 August 439p. e 23003910.1148/rg.23003937535461 · doi ↗ · pubmed ↗
- 5Ho K. L. Heterotopic Neuroglial Tissue in the Cerebral Dura Mater Clinical Neuropathology 198762462493427852 · pubmed ↗
- 6Ueno T. Kon T. Kaneko K. Takahashi T. Tomiyama M. Contrast Enhancement of Hypertrophic Dura Mater in MOG Antibody-Associated Disease Neurology 2019 August 93627127210.1212/WNL.00000000000079092-s 2.0-8507115002931383801 · doi ↗ · pubmed ↗
- 7Khaladkar S. M. Kirdat Patil P. P. Dhande A. Jhala N. A. Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease Complicated by Pachymeningitis: A Case Report Cureus 2024 July 167p. e 6486810.7759/cureus.64868 PMC 1133037339156322 · doi ↗ · pubmed ↗
- 8Michishita Y. Saito T. Uchiyama T. Myelin-Oligodendrocyte Glycoprotein Antibody-Positive Encephalitis in a Patient With Sturge-Weber Syndrome Radiology Case Reports 2024 January 1941276127910.1016/j.radcr.2024.01.00638292807 PMC 10825592 · doi ↗ · pubmed ↗