Arrhythmogenic cardiomyopathy: double, double toil, and trouble
Joana Certo Pereira, Oana Moldovan, Pedro Lopes, Bruno ML Rocha

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
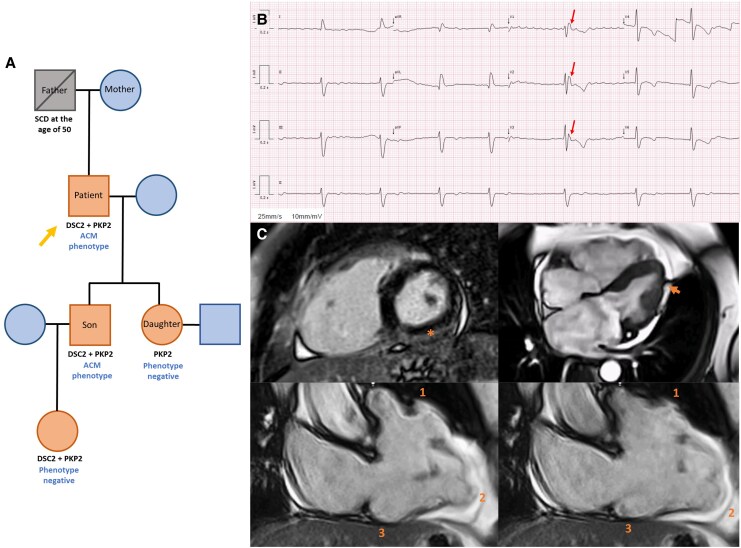 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Effects of Exercise · Trauma Management and Diagnosis · Cardiac Arrhythmias and Treatments
Summary
While single genetic variants associated with arrhythmogenic cardiomyopathy (ACM) have a highly variable penetrance and expression, compound heterozygosity increases the likelihood of displaying the ACM phenotype.^1^ We here describe the case of a patient with a positive screening with double mutation and a late-presenting ACM phenotype, emphasizing the importance of a structured systematic cascade screening.
Case description
A 70-year-old man patient with permanent atrial fibrillation, hypertension, and type 2 diabetes was referred to the Cardiomyopathy Clinic following genetic cascade screening for ACM. His son (index case) had symptomatic ACM with two pathogenic variants: PKP2 (c.1170 + 2T > A) and DSC2 [c.2112_2116del p.(Phe708fs14)]. The patient also had both the same mutations. His father had died suddenly at the age of 50 years, of unknown cause, and two other relatives were genotype-positive but phenotype-negative—see the genogram (Figure 1A*).
(A) Family tree depicting the members with pathogenic mutations, with and without an ACM phenotype. The patient’s son exhibits a positive ACM phenotype, including RV dilation and systolic dysfunction with biventricular extensive LGE, and has an implantable cardioverter-defibrillator for secondary prevention, following a syncope due to monomorphic ventricular tachycardia with left bundle branch block morphology. (B) ECG of the 70-year-old patient depicting atrial fibrillation (50–60 b.p.m.), complete right bundle branch block, epsilon waves in V1–V3 (arrow), and T-wave inversion in all precordial leads. (C) Cardiac magnetic resonance showing subepicardial LGE in the inferolateral and inferior walls of the left ventricle (asterisk), irregular myocardial contour of the LV lateral wall [‘rat-bite sign’ (arrow)], and dyskinetic movement of the right ventricular apex, and the inflow and outflow tracts [ACM ‘triangle of dysplasia’ (1, 2, 3)].
He complained of mild fatigue and orthostatic intolerance. The ECG (Figure 1B) showed atrial fibrillation, complete right bundle branch block, and epsilon waves in V_1_–V_3_. The transthoracic echocardiography revealed right ventricular (RV) dilation and moderate systolic dysfunction with free wall akinesia. The cardiac magnetic resonance imaging (Figure 1C; Supplementary Material Supplementary material online, Videos S1-S4) confirmed the reduced RV systolic function (ejection fraction 30%), apical, inflow, and outflow dyskinesia and subepicardial late gadolinium enhancement (LGE) in the so-called triangle of dysplasia. Late gadolinium enhancement was also seen in the left ventricular infero-lateral wall. Notably, both ventricles had myocardial contour irregularities (‘rat-bite sign’), suggestive of adipose infiltration. The 48 h Holter monitor (while on bisoprolol 5 mg) recorded 73 polymorphic premature ventricular contractions.
The diagnosis of biventricular ACM was established (according to the 2020 Padua criteria^2^). The estimated 5 year arrhythmic risk was 17.3% using the ACM risk calculator v3.0.^3^ Accordingly, we recommended an implantable cardioverter-defibrillator, which was placed for the primary prevention of sudden cardiac death. At 1.5 years of follow-up, the patient complains of mild fatigue and has had no cardiovascular events or ICD therapies.
Supplementary Material
ytaf563_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen L, Hu Y, Saguner AM, Bauce B, Liu Y, Shi A, et al Natural history and clinical outcomes of patients with DSG 2/DSC 2 variant-related arrhythmogenic right ventricular cardiomyopathy. Circulation 2025;151:1213–1230.40123482 10.1161/CIRCULATIONAHA.124.072226 · doi ↗ · pubmed ↗
- 2Corrado D, Perazzolo Marra M, Zorzi A, Beffagna G, Cipriani A, De Lazzari M, et al Diagnosis of arrhythmogenic cardiomyopathy: the Padua criteria. Int J Cardiol 2020;319:106–114.32561223 10.1016/j.ijcard.2020.06.005 · doi ↗ · pubmed ↗
- 3Cadrin-Tourigny J, Bosman LP, Nozza A, Wang W, Tadros R, Bhonsale A, et al A new prediction model for ventricular arrhythmias in arrhythmogenic right ventricular cardiomyopathy. Eur Heart J 2019;40:1850–1858.30915475 10.1093/eurheartj/ehz 103PMC 6568197 · doi ↗ · pubmed ↗