Pulsed field ablation of atrial fibrillation via jugular transseptal puncture in a patient with dextrocardia and interrupted inferior vena cava: a case report
Marco Scaglione, Enrico Guido Spinoni, Francesco Geuna, Andrea Lamanna, Alberto Battaglia

TL;DR
A patient with rare heart anatomy successfully underwent a new ablation procedure for atrial fibrillation using a specialized technique.
Contribution
Demonstrates the use of one-shot pulsed field ablation via jugular transseptal puncture in a patient with dextrocardia and interrupted inferior vena cava.
Findings
Multimodal imaging and jugular TSP enabled safe left atrial access in a patient with complex anatomy.
One-shot PFA was effectively used for AF ablation in this challenging case.
The procedure highlights the adaptability of PFA in rare anatomical conditions.
Abstract
Situs viscerum inversus with dextrocardia and interrupted inferior vena cava (I-IVC) are rare congenital diseases that might challenge interventional procedures, such as transcatheter ablation for atrial fibrillation (AF), when transseptal puncture (TSP) is required for left atrial access. Recently, one-shot pulsed field ablation (PFA) has emerged as a safe and effective energy modality for AF ablation. We present a case report on jugular TSP guiding one-shot PFA in a patient presenting dextrocardia and an I-IVC, addressing the unique anatomical challenges. A 52-year-old male with situs viscerum inversus with dextrocardia and I-IVC presented to our institution with symptomatic paroxysmal AF. Pre-procedural evaluation included transthoracic echocardiography and cardiac magnetic resonance (CMR) imaging. The PFA procedure was successfully performed under general anaesthesia guided by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
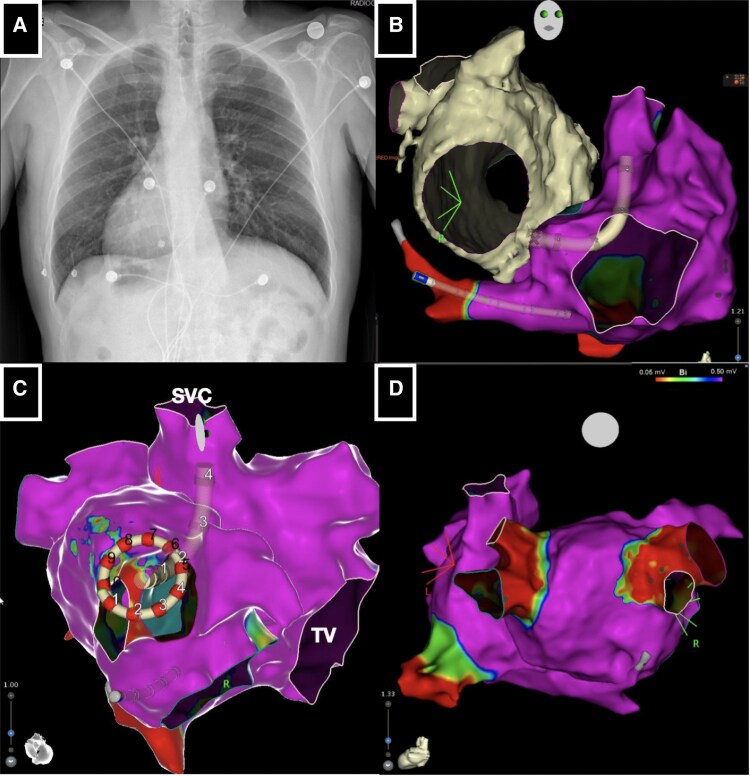 Figure 1
Figure 1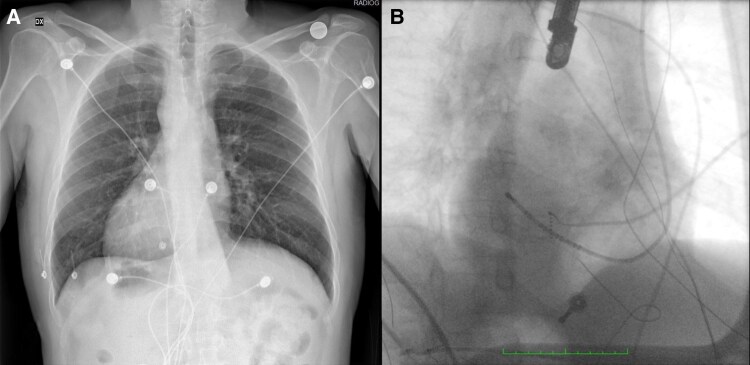 Figure 1
Figure 1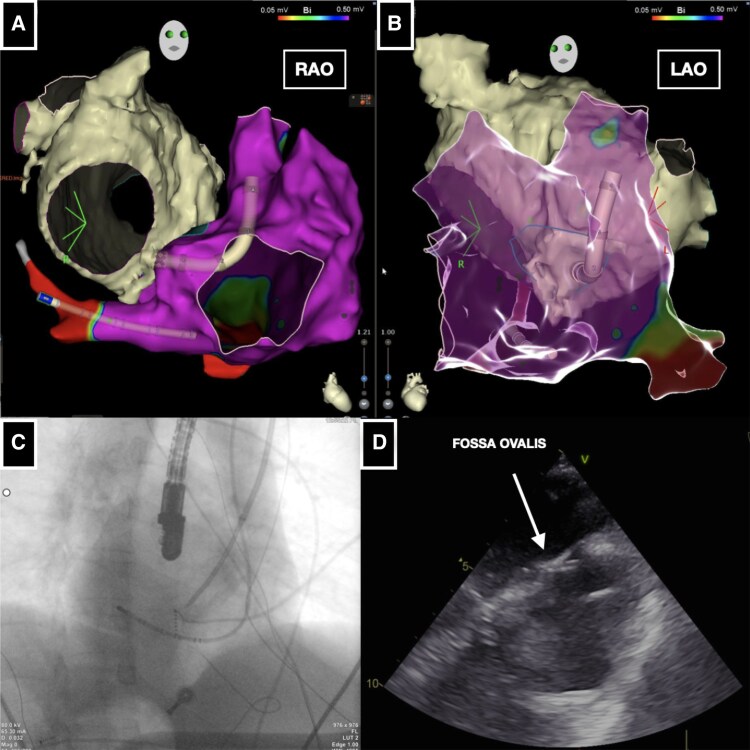 Figure 2
Figure 2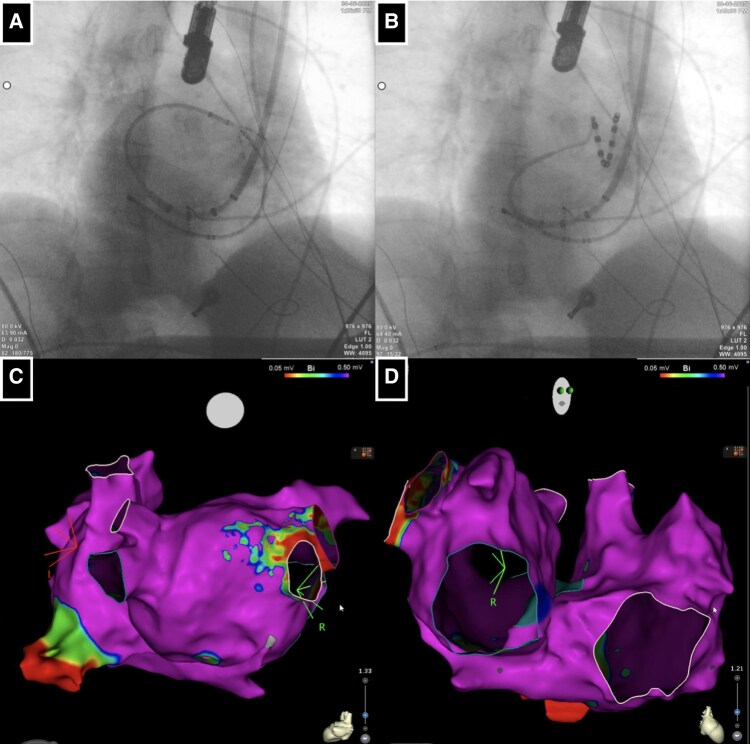 Figure 3
Figure 3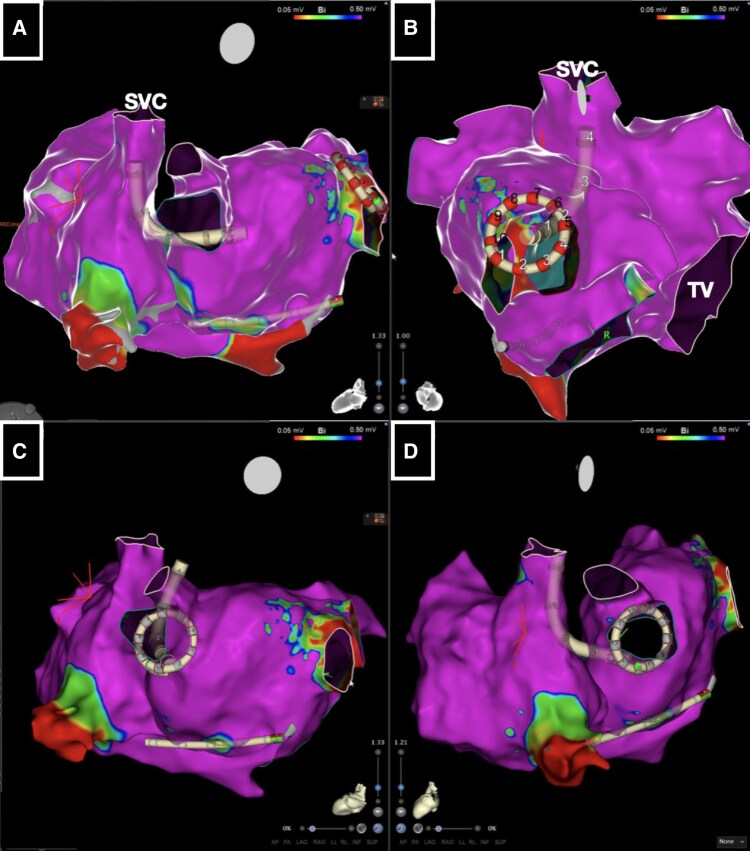 Figure 4
Figure 4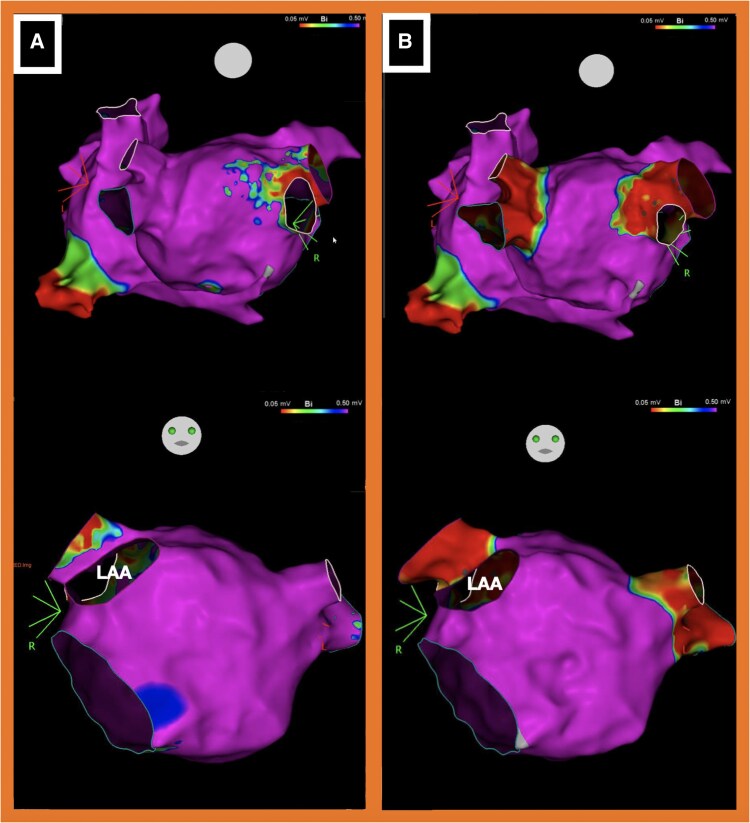 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Cardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes
Introduction
Situs viscerum inversus with dextrocardia and interrupted inferior vena cava (I-IVC) are exceptionally rare congenital malformations.^1,2^ The coexistence of these conditions presents a significant procedural challenge in transcatheter ablation of atrial fibrillation (AF), particularly when transseptal puncture (TSP) is required to access the functional left atrium (LA).
Recently, one-shot pulsed field ablation (PFA) has emerged as a safe and effective energy modality for AF ablation.^3,4^
In this report, we describe a transjugular approach for guiding one-shot PFA in a patient with both dextrocardia and an I-IVC.
Summary figure
Pulsed field ablation of atrial fibrillation in a patient with situs viscerum inversus, dextrocardia, and interrupted inferior vena. (A) Standard chest radiography highlighting dextrocardia. (B) Electroanatomical mapping (RAO projection mimicking LAO) with cardiac magnetic resonance integration guiding the positioning of the VIZIGO sheath at the fossa ovalis. (C) Electroanatomical mapping guiding Varipulse catheter positioning within anatomical right pulmonary veins. (D) Electroanatomical mapping post-ablation confirming complete pulmonary vein isolation with PFA.
Case presentation
A 52-year-old man presented to our institution with episodes of symptomatic paroxysmal AF. He had a pre-existing diagnosis of situs viscerum inversus with dextrocardia (Figure 1A). Transthoracic echocardiography during his initial cardiological evaluation showed a preserved ejection fraction (EF; 65%), mild mitral regurgitation, and confirmed dextrocardia. Anti-arrhythmic drug therapy with flecainide 100 mg twice daily (b.i.d.) was initiated. Due to symptomatic relapse of arrhythmia, an AF ablation procedure was planned. Upon in-hospital admission, the patient was in stable sinus rhythm (SR).
(A) Standard chest radiography highlighting dextrocardia. (B) Fluoroscopy right anterior oblique (RAO) projection with decapolar catheter inserted in the coronary sinus mimicking left anterior oblique (LAO) projection.
The pre-procedural workflow included cardiac magnetic resonance (CMR) imaging for the reconstruction of the heart chambers and major vessels. The CMR scan revealed the absence of IVC connection to the functional right atrium, consistent with suspected I-IVC and the presence of azygos vein continuation. Ablation was performed the following day under general anaesthesia, guided by transoesophageal echocardiography (TOE), fluoroscopy, electroanatomical (EAM) mapping, and merging of CMR imaging.
Right femoral vein access was obtained under echocardiographic guidance. Contrast medium was then injected through the sheath, confirming the suspected I-IVC and the presence of azygos vein continuation. Subsequently, ultrasound-guided accesses were obtained via the left internal jugular vein and the left subclavian vein. A decapolar deflectable catheter was advanced into the coronary sinus via the left subclavian vein access (Figure 1B). At this time, a bi-directional guiding sheath (CARTO VIZIGO™, Biosense Webster, Irvine, CA, USA) with integrated visualization on the EAM mapping system (CARTO3, Biosense Webster) was introduced via the jugular vein access. Reconstruction of the functional right atrium was then performed using a multipolar mapping catheter (Pentaray, Biosense Webster). The obtained EAM was subsequently merged with the previously acquired CMR imaging (Figure 2A and B) to guide and identify the optimal site for TSP.
(A and B) Electroanatomical mapping [RAO projection mimicking LAO projection (A) and LAO projection mimicking RAO projection (B)] with cardiac magnetic resonance integration guiding the positioning of the VIZIGO sheath at the fossa ovalis. (C and D) Fluoroscopy RAO projection (C) and transoesophageal echocardiography (D) guiding the positioning of Fast-Cath long sheath at the fossa ovalis.
A manually curved Brockenbrough needle (BRK, St. Jude Medical) was advanced into the right atrium via the VIZIGO™ sheath, which was inserted through the right jugular vein, under fluoroscopic, EAM, and TOE guidance. However, it was not possible to adequately deflect the VIZIGO™ sheath to engage the fossa ovalis for the TSP. Consequently, it was replaced with an 8.5 Fr transseptal long sheath (Fast-Cath 60 cm, Mullins Curve, St. Jude Medical, Minneapolis, MN, USA). The Brockenbrough needle (BRK, St. Jude Medical) was then advanced via the left jugular vein into the right atrium through this new sheath (Figure 2C). The key point was to manually bend the needle to create a very large curve being able to engage and support the TSP puncture, as confirmed by TOE (Figure 2D).
Once left atrial (LA) access was achieved, the long sheath was replaced with the VIZIGO™ sheath to allow its deflection into the LA to manoeuvre better both the mapping and the ablation catheter (Figure 3A and B). Once the EAM of the LA was reconstructed with the mapping catheter, it was merged with the CMR imaging rendering by CARTO-Merge software (Biosense Webster) (Figure 3C and D). Considering that a point-by-point ablation strategy might be challenging due to the complexity of LA access and anatomical relationships, a single-shot variable-loop PFA catheter was selected (Varipulse™, Biosense Webster), delivering four PFA pulses per vein, as per the current protocol^5^ (Figure 4).
(A) Fluoroscopy RAO projection guiding mapping catheter manoeuvres in the left atrium. (B) Fluoroscopy RAO projection guiding variable loop pulsed field ablation catheter manoeuvres in the left atrium. (C and D) Electroanatomical reconstruction of the left and right atrium in postero-anterior (PA) and RAO projection.
(A–D) Electroanatomical map projections guiding variable loop pulsed field ablation catheter positioning in the pulmonary veins for transcatheter ablation. SVC, superior vena cava; TV, tricuspid valve.
Following the ablation phase, a new EAM was performed, confirming complete isolation of all four pulmonary veins (Figure 5B). The skin-to-skin procedure time was 150 min. Post-procedure, transthoracic echocardiography was conducted, which excluded the presence of a significant pericardial effusion. The patient was monitored for 24 h post-procedure. Thoracic radiography performed the following day revealed no evidence of pneumothorax. The patient was discharged home the day after the ablation procedure.
(A) Electroanatomical map before atrial fibrillation ablation (upper figure PA projection, lower figure AP projection). (B) Electroanatomical map after atrial fibrillation ablation (upper figure PA projection, lower figure AP projection) confirming pulmonary vein isolation. LAA, left atrial appendage.
Discussion
In patients with IVC interruption, which precludes the use of standard femoral vein access for electrophysiology procedures, several strategies have been described, including the superior approach (jugular or subclavian vein), transhepatic access, and transaortic access.^6–10^ We opted for the superior transjugular approach due to its favourable risk–benefit profile, supported by a low reported rate of major complications and our centre’s extensive expertise in echo-guided jugular vein puncture
Use of right internal jugular vein for TSP was first described by Lim et al. for AF ablation in three patients with I-IVC, and the results were subsequently reproduced by small case series from different groups employing various approaches.^6–10^ In most of these cases, fluoroscopy and intracardiac echocardiography (ICE) guidance were used to detect the right puncture site. Transoesophageal echocardiography is reported as a safe alternative. In these cases, the TSP has been performed with a Brockenbrough needle manually curved or using a radiofrequency (RF) needle or RF wire.^6–10^
A single case report by Xu et al.^11^ described TSP by ICE guidance in a patient with I-IVC and dextrocardia.
In our case report, the patient exhibited a highly complex anatomy, characterized by an I-IVC and situs viscerum inversus with dextrocardia. Our procedural workflow involved the integration of multiple imaging modalities (CMR, TOE, and fluoroscopy combined with EAM). By combining these techniques, we were able to effectively guide the procedure, identify the optimal site, and perform the TSP safely. Our workflow for jugular TSP included:
Ultrasound-guided left jugular and subclavian vein accessDecapolar catheter advancement by the left subclavian vein in coronary sinus with an initial EAM reconstruction of the right atriumPositioning of mapping catheter through the jugular vein and complete reconstruction of the right atrium allowing merging and alignment with corresponding CMR renderingPositioning of VIZIGO™ sheath visualized by EAM in the right atrium on the fossa ovalis, confirmed by fluoroscopy and TOE imagingSubstitution of VIZIGO™ sheath with Fast-Cath long sheath, which provided substantial support for needle advancement for TSP
Numerous studies have recently been published on the safety and efficacy of variable-loop one-shot PFA catheters.^12–14^ Given these results, and considering the patient’s exceptionally complex anatomy, which could potentially influence the manoeuvrability of the ablation catheter and impact ablation outcomes in terms of safety and efficacy, ablation was performed using a single-shot variable-loop PFA catheter. Furthermore, the curvature of the catheter, supported by the bi-directional long sheath, enabled the effective ablation even in LA regions that would have otherwise been extremely challenging to target, such as the anatomically ‘left pulmonary veins’ (Figure 3B). The critical steps of this procedure were the following: (i) the integration of imaging (fluoroscopy, CMR, EAM, and TOE) which allowed effective and safe access to the target chamber; and (ii) the availability of the one-shot ablation tool, which offered good manoeuvrability and a favourable safe profile, enabling a procedure in such complex anatomy.
To the best of our knowledge, there have been no previously published cases of AF ablation using PFA performed via jugular TSP in patients with dextrocardia and an I-IVC.
Conclusions
In patients with complex anatomy, as dextrocardia with I-IVC, imaging integrations and the use of variable loop single-shot PFA catheter were effective in carrying out AF ablation by jugular TSP.
Lead author biography
Professor Marco Scaglione is an interventional arrhythmologist and director of the electrophysiology laboratory in Asti. The centre he leads is a national reference for interventional electrophysiology procedures in adult patients, paediatric populations, and adults with congenital heart disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bohun CM, Potts JE, Casey BM, Sandor GGS. A population-based study of cardiac malformations and outcomes associated with dextrocardia. Am J Cardiol 2007;100:305–309.17631088 10.1016/j.amjcard.2007.02.095 · doi ↗ · pubmed ↗
- 2Timmers GJ, Falke TH, Rauwerda JA, Huijgens PC. Deep vein thrombosis as a presenting symptom of congenital interruption of the inferior vena cava. Int J Clin Pract 1999;53:75–76.10344071 · pubmed ↗
- 3Reddy VY, Gerstenfeld EP, Natale A, Whang W, Cuoco FA, Patel C, et al ADVENT investigators. Pulsed field or conventional thermal ablation for paroxysmal atrial fibrillation. N Engl J Med 2023;389:1660–1671.37634148 10.1056/NEJ Moa 2307291 · doi ↗ · pubmed ↗
- 4Reddy VY, Calkins H, Mansour M, Wazni O, Di Biase L, Bahu M, et al Pulsed field ablation to treat paroxysmal atrial fibrillation: safety and effectiveness in the Adm IRE pivotal trial. Circulation 2024;150:1174–1186.39258362 10.1161/CIRCULATIONAHA.124.070333 PMC 11458102 · doi ↗ · pubmed ↗
- 5Nair DG, Gomez T, De Potter T. VARIPULSE: a step-by-step guide to pulmonary vein isolation. J Cardiovasc Electrophysiol 2024;35:1817–1827.Erratum in: J Cardiovasc Electrophysiol. 2025 Jan;36(1):303. doi: 10.1111/jce.16522.39004800 10.1111/jce.16366 · doi ↗ · pubmed ↗
- 6Lim HE, Pak HN, Tse HF, Lau CP, Hwang C, Kim YH. Catheter ablation of atrial fibrillation via superior approach in patients with interruption of the inferior vena cava. Heart Rhythm 2009;6:174–179.19187906 10.1016/j.hrthm.2008.10.026 · doi ↗ · pubmed ↗
- 7Kato H, Kubota S, Goto T, Inoue K, Oku N, Haba T, et al Transseptal puncture and catheter ablation via the superior vena cava approach for persistent atrial fibrillation in a patient with polysplenia syndrome and interruption of the inferior vena cava: contact force-guided pulmonary vein isolation. Europace 2017;19:1227–1232.27174901 10.1093/europace/euw 095 · doi ↗ · pubmed ↗
- 8Liang JJ, Lin A, Mohanty S, Muser D, Briceno DF, Burkhardt JD, et al Radiofrequency-assisted transseptal access for atrial fibrillation ablation via a superior approach. JACC Clin Electrophysiol 2020;6:272–281.32192677 10.1016/j.jacep.2019.10.019 · doi ↗ · pubmed ↗