Septic Shock Due to Brevundimonas diminuta Bacteremia in an Immunocompetent Patient: A Case Report With a Literature Review of Antimicrobial Resistance Patterns
Aleksandra Kaplina, Kanika Rathi, Chandra Hassan, Michael Samotowka, Riley G Jones

TL;DR
A rare case of septic shock caused by Brevundimonas diminuta in an otherwise healthy patient is reported, highlighting the challenges of diagnosing and treating this uncommon infection.
Contribution
This is the first reported case of B. diminuta septic shock in an immunocompetent individual.
Findings
Brevundimonas diminuta caused septic shock in an immunocompetent patient.
Only 12 cases of B. diminuta infections have been reported in North America.
B. diminuta presents diagnostic and therapeutic challenges due to its rare occurrence and variable antibiotic susceptibility.
Abstract
Brevundimonas species are a group of aerobic, non-fermenting, Gram-negative bacilli that are primarily environmental organisms commonly isolated from soil, water, and hospital surfaces. While historically regarded as non-pathogenic, they are increasingly recognized as opportunistic pathogens in immunocompromised or critically ill individuals. While most Brevundimonas species are not known to cause human disease, Brevundimonas diminuta and Brevundimonas vesicularis are the two species most commonly associated with human infections. Due to its uncommon occurrence and variable antibiotic susceptibility, B. diminuta is a diagnostic and therapeutic challenge. To our knowledge, only 12 cases of B. diminuta infections have been reported in North America to date. Here, we present a rare case of septic shock due to B. diminuta bacteremia in an immunocompetent patient.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
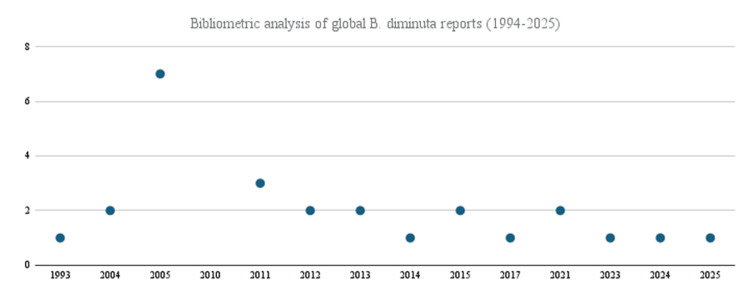 Figure 1
Figure 1| Laboratory tests | Patient's values | Reference range |
| Blood | ||
| Sodium | 122 mmol/L | 136-145 mmol/L |
| C-reactive protein (CRP) | 193.8 mg/L | 0.0-5.0 mg/L |
| Procalcitonin | 1.58 ng/mL | <0.1 ng/mL |
| White blood cells (WBC) | 11.7 × 10E3/uL | 4.0-10.0 × 10E3/uL |
| Lactic acid | 1.9 mmol/L | 0.3-1.5 mmol/L |
| Creatinine | 5.87 mg/dL | 0.51-1.18 mg/dL |
| Urine | ||
| Leukocyte esterase | Positive | Negative |
| White blood cells per high-power field | 21 | 0-5 |
| Antibiotic | MIC | Interpretation |
| Amikacin | ≤2 µg/mL | Susceptible |
| Cefepime | 8 µg/mL | Susceptible |
| Ceftazidime | 16 µg/mL | Intermediate |
| Ciprofloxacin | ≥4 µg/mL | Resistant |
| Gentamicin | ≤1 µg/mL | Susceptible |
| Levofloxacin | 4 µg/mL | Intermediate |
| Meropenem | 0.5 µg/mL | Susceptible |
| PiperacillintTazobactam | ≤4 µg/mL | Susceptible |
| Tobramycin | ≤1 µg/mL | Susceptible |
| Trimethoprim/sulfamethoxazole | ≥320 µg/mL | Resistant |
| Author (Ref.) | Year | Sex/age | Country | Comorbidity | Type of infection |
| Pasadakis et al. [ | 1993 | N/A | Greece | End-stage renal failure | Peritonitis |
| Seve et al. [ | 2004 | F/35 | France | Leukemia | Bacteremia (hospital-acquired) |
| Chi et al. [ | 2004 | M/62 | Taiwan | Liver cirrhosis (hepatitis B associated), esophageal varices, encephalopathy, spontaneous bacterial peritonitis, duodenal ulcer | Bloodstream infection (community-acquired) |
| Han et al. [ | 2005 | Multiple (7 cases) | USA | Cancer | Bacteremia, UTI, empyema (hospital-acquired) |
| Lee et al. [ | 2011 | 3 Cases | Taiwan | Cancer | Bacteremia |
| Almuzara et al. [ | 2012 | F/56 | Argentina | Lupus glomerulonephritis | Leg ulcer |
| Pandit et al. [ | 2012 | F/66 | USA | N/A | Keratitis (community-acquired) |
| Lu et al. [ | 2013 | M/38 | China | None | Pleuritis |
| Shobha et al. [ | 2013 | Infant | India | None | UTI |
| Mahapatra et al. [ | 2014 | M/35 | India | None | Post-traumatic abscess |
| Cao et al. [ | 2015 | M/62 | China | Myelodysplastic syndrome, DM type 2 | Bacteremia |
| Ghosh et al. [ | 2015 | N/A | India | Tuberculosis | N/A |
| Chandra et al. [ | 2017 | M/18 | India | Focal segmental glomerulosclerosis with nephrotic syndrome | Bacteremia |
| Lupande-Mwenebitu et al. [ | 2021 | Newborn | Democratic Republic of Congo | Low-weight, preterm | Omphalitis |
| Burch et al. [ | 2021 | M/67 | USA | DM type 1, stage 0 CLL | Hepatic abscess |
| Hassan et al. [ | 2023 | M/47 | USA | COPD, bipolar disorder, stable seizure disorder | Sepsis, lung abscess |
| Ferreira Caceres et al. [ | 2024 | M/69 | USA | Adrenal insufficiency secondary to panhypopituitarism, CHFpEF, atrial fibrillation, NASH, OSA, pulmonary hypertension, morbid obesity | Sepsis secondary to cellulitis of the abdominal wall and right lower extremity |
| Thareja et al. [ | 2025 | M/50 | USA | N/A | Keratitis |
| Country | Amikacin | Netilimycin | Fosfomycin | Gentamicin | Tobramycin | Doxycyline | Tetracycline | Minocycline | Tigecycline | Imipenem | Meropenem | Aztreonam | Mezlocillin | Carbenicillin | Piperacillin | Amoxicillin/ Clavulanate | Piperacillin/ Tazobactam | Ticarcillin | Ticarcillin/ Clavulanate | Trimethoprim/ Sulfamethoxazole | Cefoperazone/ Sulbactam | Nitrofurantoin | Cefalothin | Cefoxitin | Cefazolin | Ceftriaxone | Ceftazidime | Ceftazidime/ Clavulanate | Cefuroxime | Cefepime | Cefoperazone | Cefotaxime | Ampicillin | Ampicillin/ Sulbactam | Gatifloxacin | Levofloxacin | Ciprofloxacin | Moxifloxacin | Chloramphenicol | Flomoxef | Rifampicin | Colistin | |
| Case 1 (Pasadakis et al. [ | Greece | - | - | - | - | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Case 2 (Seve et al. [ | France | R | - | - | - | - | - | - | - | - | S | - | - | - | - | R | - | - | - | - | - | - | - | - | - | - | - | R | - | - | R | - | - | - | - | - | - | S | - | - | - | - | - |
| Case 3 (Chi et al. [ | Taiwan | S | - | - | S | S | S | - | - | - | S | - | S | - | - | - | - | S | - | - | S | - | - | - | - | R | R | R | - | S | S | R | S | R | - | - | - | S | - | S | - | - | - |
| Case 4 (Han et al. [ | USA | ||||||||||||||||||||||||||||||||||||||||||
| Case 4a | USA | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | S | - | - | - | - | - | S | R | - | - | R | - | - | I | - | R | R | R | - | - | - | - | - |
| Case 4b | USA | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | S | - | - | - | - | - | R | R | - | - | R | - | - | R | - | R | R | R | - | - | - | - | - |
| Case 4c | USA | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | R | - | - | - | - | - | - | R | - | - | - | - | - | R | - | - | - | R | - | - | - | - | - |
| Case 4d | USA | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | R | - | - | - | - | - | - | S | - | - | - | - | - | I | - | - | - | R | - | - | - | - | - |
| Case 4e | USA | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | R | - | - | - | - | - | I | R | - | - | R | - | - | R | - | R | R | R | - | - | - | - | - |
| Case 4f | USA | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | R | - | - | - | - | - | R | R | - | - | R | - | - | I | - | R | R | R | - | - | - | - | - |
| Case 4g | USA | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | R | - | - | - | - | - | R | R | - | - | R | - | - | R | - | R | R | R | - | - | - | - | - |
| Case 5 (Lee et al. [ | Taiwan | ||||||||||||||||||||||||||||||||||||||||||
| Case 5a | Taiwan | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | R | - | - | - | - | R |
| Case 5b | Taiwan | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | R | - | - | - | - | R |
| Case 5c | Taiwan | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | R | - | - | - | - | R |
| Case 6 (Almuzara et al. [ | Argentina | R | - | - | R | - | - | - | S | S | R | R | R | - | - | - | - | R | - | - | R | - | - | R | R | - | - | R | - | - | R | - | R | R | R | - | - | R | - | - | - | - | R |
| Case 7 (Pandit et al. [ | USA | S | - | - | S | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | R | - | - | - | - | R | R | - | - | - | R | R | - | - | - | - |
| Case 8 (Lu et al. [ | China | S | - | - | S | - | - | S | - | - | S | S | R | - | - | - | - | S | - | - | R | S | - | - | - | - | - | R | - | - | R | - | - | - | - | - | R | R | - | S | - | - | - |
| Case 9 (Shobha et al. [ | India | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | S | - | - | S | S | - | - | - | - | - | - | - | - | - | S | - | S | - | - | - | - | R | - | - | - | - | - |
| Case 10 (Mahapatra et al. [ | India | S | - | - | - | - | - | - | - | - | S | - | - | - | - | - | R | S | - | - | - | S | - | - | - | - | - | - | - | - | - | - | S | - | - | - | R | R | - | - | - | - | - |
| Case 11 (Cao et al. [ | China | S | - | - | S | R | - | - | - | - | S | - | R | - | - | - | - | S | - | - | S | - | - | - | - | S | S | S | - | - | S | - | - | S | S | - | S | S | - | - | - | - | - |
| Case 12 (Ghosh et al. [ | India | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Case 13 (Chandra et al. [ | India | S | - | - | S | - | - | - | S | S | S | S | - | - | - | - | - | - | - | - | S | S | - | - | - | - | - | S | - | - | S | S | - | - | - | S | S | S | S | - | - | - | R |
| Case 16 (Lupande-Mwenebitu et al. [ | Democratic Republic of Congo | S | - | S | R | - | - | - | - | - | S | S | - | - | - | - | - | S | R | R | R | - | R | - | - | - | - | R | - | - | S | - | - | - | - | - | - | R | - | - | - | S | - |
| Case 17 (Burch et al. [ | USA | - | - | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | - | - | - | - | - | - | R | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Case 18 (Hassan et al. [ | USA | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - |
| Case 19 (Ferreira Caceres et al. [ | USA | S | - | - | S | S | - | S | - | - | - | - | S | - | - | - | - | S | - | - | S | - | - | - | - | - | S | - | - | - | S | - | - | - | - | - | S | S | - | - | - | - | - |
| Case 20 (Thareja et al. [ | USA | S | - | - | S | S | - | - | - | - | - | - | - | - | - | - | - | S | - | - | - | - | - | - | - | - | S | R | - | - | I | - | - | - | - | - | - | R | - | - | - | - | - |
| Case 21 (current) | USA | S | - | - | S | S | - | - | - | - | - | S | - | - | - | - | - | S | - | - | S | - | - | - | - | - | - | - | I | - | S | - | - | - | - | - | I | R | - | - | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfections and bacterial resistance · Antibiotic Resistance in Bacteria · Streptococcal Infections and Treatments
Introduction
Brevundimonas is a genus of bacteria comprised of 25 species of bacteria, which are rarely associated with human infections. Brevundimonas are aerobic, non-fermenting, Gram-negative rods with catalase- and oxidase-positive activity. Morphologically, they have a small, polar flagella [1]. Brevundimonas were first reported as human pathogens in 1993, although it was still classified at the time as a strain of *Pseudomonas *[2]; however, the incidences may be somewhat underreported since identification with real-time PCR was not widely available until 2010. Although rare, Brevundimonas has recently been identified as an emerging pathogen, primarily B. vesicularis and, to a lesser extent, B. diminuta. To our knowledge, only 12 cases of B. diminuta infection have been reported in the United States [3-8], with only three cases of bacteremia in adults or children [3,6,7], all of whom were reportedly immunocompromised. Importantly, Brevundimonas have a wide range of antimicrobial resistance, which, coupled with limited reports and data available, makes management difficult when clinically significant infections are encountered. Here, we present the full body of known resistance patterns of this rare disease by presenting this case of B. diminuta bacteremia causing septic shock in an immunocompetent patient who was successfully treated with cefepime and made a full recovery.
Case presentation
A 64-year-old male with a history of coronary artery disease, hypertension, major depressive disorder, and alcohol use disorder presented with severe fatigue and malaise. He reported hospitalization one month prior for an episode of severe alcohol withdrawal; he had no history of immunosuppression or immunocompromising condition. From the time of discharge, he reported ongoing alcohol abuse accompanied by progressive weakness to the point of being bed-bound for the week leading up to hospitalization; he denied a history of IV drug use or vascular access devices. He was found by a maintenance worker on a routine house call and taken to the emergency department.
On arrival, he was hypothermic to 35.4°C (95.8°F) and hypotensive to 80/41 mmHg with a pulse of 74 beats per minute and a respiratory rate of 18 breaths per minute. He was ill-appearing and found with a stage II sacral decubitus ulcer wound, which did not show any signs of infection; the remainder of his exam was normal. He did not meet the American Society for Parenteral and Enteral Nutrition (ASPEN) criteria for malnutrition. CT imaging of the head, chest, and abdomen was negative for acute findings. He was negative for HIV and hepatitis B and C. Laboratory results relevant to the case are presented in Table 1.
His hypotension was refractory to multiple fluid boluses; thus, vasopressors were started, two sets of blood cultures were obtained, and broad-spectrum antibiotic therapy was initiated with vancomycin and cefepime. The patient was diagnosed with septic shock and admitted to the intensive care unit (ICU) for further management. Urine cultures revealed polymicrobial bacterial overgrowth of greater than three microorganisms and were deemed contaminated due to possible faulty collection by a laboratory testing protocol, consistent with a benign physical exam of the abdomen. His blood cultures were ultimately positive for high-grade Brevundimonas diminuta in four of four blood culture samples. Cultures revealed sensitivity to cefepime; thus, antibiotics were narrowed (Table 2). Repeat blood cultures after 48 hours were negative, so a one-week course of cefepime was administered. Immunoglobulin and vitamin levels were obtained and were normal. The infectious disease service was consulted for further exploration of the source of infection; however, no source or point of entry could be identified. He remained in the ICU for three days and had a steady recovery with normalization of renal function and inflammatory markers. He was transferred to the medical floor on hospital day 4, where he continued cefepime for a total of seven days. He was discharged home, and at the one-month follow-up, he remained well, with no recurrence of illness or bacteremia. At that encounter, he provided written consent for the publication of his case.
Discussion
The genus Brevundimonas was first proposed by Segers et al. in 1994 by identifying Pseudomonas diminuta and Pseudomonas vesicularis as a distinct genus based on the results of DNA-rRNA hybridization studies [2]. Subsequent quantitative real-time polymerase chain reaction (qPCR) and fluorescence in situ hybridization (FISH) assays were developed in 2010, making the identification of B. diminuta more widely and rapidly available.
A number of severe infections in malnourished and immunocompromised individuals have been associated with* Brevundimonas,* such as Noma disease, alternatively known as cancrum oris, a rapidly progressive orofacial gangrene typically affecting severely malnourished children in low-resource settings. While our patient was physically debilitated, evaluation by a clinical nutritionist confirmed the absence of malnutrition, and serum analysis with normal levels of vitamins B1, B5, B6, B9, B12, D3, C, Zn, Se, and thyroid-stimulating hormone. In addition, he was not considered immunocompromised, as his immunology laboratory results were within normal limits, no history of using immunosuppressing agents, and his HIV status was negative. His low heart rate of 74 beats per minute was attributed to beta-blockade used for the patient’s coronary artery disease and hypertension management.
Infections caused by B. diminuta are rare and have been infrequently reported in the medical literature; its virulence is generally considered low [1]. As a result, there is limited understanding of the pathogen's full clinical significance, pathogenic mechanisms, and optimal treatment strategies, which poses a challenge to clinicians faced with a clinically significant infection. Using a PubMed, EMBASE, and CINAHL query with citation chain search of "brivundimonas", "brivundimon*", and "pseudomonas diminuta" were captured and filtered for human reports, wherein 26 cases of B. diminuta infections worldwide out of 27 with citations were able to be located. Sixteen cases were reported across 10 reports after 2010 (Figure 1), which might correlate with more easily accessible testing and increased recognition of the species. Most of the reports were complicated by significant comorbidities that rendered patients immunocompromised and susceptible to opportunistic infections; only five cases were observed in immunocompetent patients without significant comorbidities (Table 3). Our analysis revealed an important complication in the existing literature: a widely cited paper was found with significant discrepancies between the manuscript text and the supplemented chart [1]. Furthermore, a single report in grey medical literature was unable to be obtained for review despite exhausting attempts with the assistance of a research librarian.
Bibliometric analysis of global Brevundimonas diminuta reports (1994-2025)
Given the rarity of* B. diminuta *as a clinical pathogen, initial consideration was given to the possibility of specimen contamination; however, this was determined less likely when the second set was positive with concordant antibiotic resistance patterns. Alternatively, a laboratory pseudo-outbreak during the evaluation was considered. Pseudo-outbreaks are defined as an increase in identified organisms without evidence of true infection, usually reflecting laboratory supply contamination. They have been linked to factors such as contaminated culture media, syringes, blood culture vials, inadequate disinfection of analyzers, and improperly sterilized equipment. The literature review only shows two episodes of pseudo-outbreaks, one in the United States in 2017 and in South Korea in 2011 [1]. In our case, consultation with hospital infection control staff confirmed no pseudo-outbreak in our facility, further highlighting B. diminuta as the cause of septic shock in our patient.
Antimicrobial resistance is an emerging concern worldwide. In our analysis, B. diminuta showed varied and extensive resistance patterns. Concerningly, B. diminuta appeared widely resistant against antibiotics commonly used as empiric treatments for various infections, such as sepsis and abscesses, namely, fluoroquinolones, sulfonamides, colistin, and several beta-lactams. Antibiotic sensitivity is conserved with carbapenems, aminoglycosides, and ticarcillin/clavulanate. As such, the sensitivity analysis should be performed on a case-by-case basis to tailor antibiotic regimens when B. diminuta infections are encountered (Table 4).
Conclusions
B. diminuta is a rare cause of clinically significant infection, typically associated with malnourished or immunocompromised states. Antimicrobial resistance is a significant challenge to practitioners treating B. diminuta infections. Analysis reveals extensive resistance to fluoroquinolones, sulfonamides, and colistin. Sensitivity is preserved to carbapenems, aminoglycosides, and ticarcillin/clavulanate. Varied sensitivity to beta-lactams is observed, highlighting the need for antibiotic sensitivity assays when a clinically significant infection is encountered.
Here, we add to the existing literature a case of B. diminuta bacteremia with septic shock in an immunocompetent patient successfully treated with cefepime and build on previously reported cases with a compilation of antimicrobial resistance patterns emerged from a detailed analysis of available literature. Further research is warranted to explore the immunologic mechanisms behind B. diminuta infections in immunocompetent patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brevundimonas spp: emerging global opportunistic pathogens Virulence Ryan MP Pembroke JT 480493920182948491710.1080/21505594.2017.1419116 PMC 5955483 · doi ↗ · pubmed ↗
- 2Classification of Pseudomonas diminuta Leifson and Hugh 1954 and Pseudomonas vesicularis Büsing, Döll, and Freytag 1953 in Brevundimonas gen. nov. as Brevundimonas diminuta comb. nov. and Brevundimonas vesicularis comb. nov., respectively Int J Syst Bacteriol Segers P Vancanneyt M Pot B 499510441994806854310.1099/00207713-44-3-499 · doi ↗ · pubmed ↗
- 3Brevundimonas diminuta infections and its resistance to fluoroquinolones J Antimicrob Chemother Han XY Andrade RA 8538595520051588318010.1093/jac/dki 139 · doi ↗ · pubmed ↗
- 4Brevundimonas diminuta keratitis Eye Contact Lens Pandit RT 63653820122161753510.1097/ICL.0b 013e 31821 c 04f 7 · doi ↗ · pubmed ↗
- 5Brevundimonas diminuta coinfection as source of pyogenic liver abscess BMJ Case Rep Burch J Tatineni S Enofe I Laird-Fick H 14202110.1136/bcr-2020-236235 PMC 811798933975829 · doi ↗ · pubmed ↗
- 6Brevundimonas diminuta-induced lung abscess in an immunocompetent adult: a rare case report Cureus Hassan MA Syed F Singh GP Pakala R Gasmelseed H 015202310.7759/cureus.42371 PMC 1044550437621835 · doi ↗ · pubmed ↗
- 7Brevundimonas diminuta bacteremia in a case of adrenal insufficiency: a case report and literature review Cureus Ferreira Caceres MM Veliz Caceres E Alvarez Silva MA Rosas LA 016202410.7759/cureus.75943 PMC 1174063639830549 · doi ↗ · pubmed ↗
- 8A sneaky culprit: secondary infectious keratitis due to Brevundimonas diminuta Eye Contact Lens Thareja SK Luo S Carballo S 2442465120253987449310.1097/ICL.0000000000001170 · doi ↗ · pubmed ↗