Management of patients with lower urinary tract symptoms due to benign prostatic enlargement at risk of progression treated with 5-alpha-reductase inhibitors: examining real-world clinical practice in Spain and Brazil
Juan Manuel Palacios, Pratiksha Kapse, Vanessa Cortés, Marcio Augusto Averbeck, Alberto Budia Alba, Danilo Souza Lima da Costa Cruz, Suryakant Somvanshi, Fiona Pereira

TL;DR
This study examines how urologists in Spain and Brazil manage patients with prostate enlargement symptoms using a specific type of medication.
Contribution
The study reveals real-world clinical practices of urologists in Spain and Brazil regarding the use of 5ARIs for LUTS/BPE.
Findings
Most urologists in Spain and Brazil assess risk factors for disease progression before prescribing 5ARIs.
Urologists often use higher thresholds for risk factors than recommended by guidelines.
Sexual function concerns were a common barrier to initiating 5ARI treatment.
Abstract
For patients with lower urinary tract symptoms due to benign prostatic enlargement (LUTS/BPE), assessing patient risk of disease progression is important to determine if treatment with 5-alpha-reductase inhibitors (5ARIs) is warranted. Clinical trials and guidelines have identified risk factors for disease progression, which affects subsequent treatment decision making; however, real-world clinical practices may differ. This non-interventional, cross-sectional study examined the management of patients with LUTS/BPE at risk of disease progression receiving 5ARIs by urologists from Spain and Brazil. Urologists were randomly recruited and completed an online questionnaire comprising multiple-choice, open-ended ranking and rating questions on their clinical approach in patients with LUTS/BPE receiving 5ARIs. Urologists also provided patient record forms for two recent patients treated with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
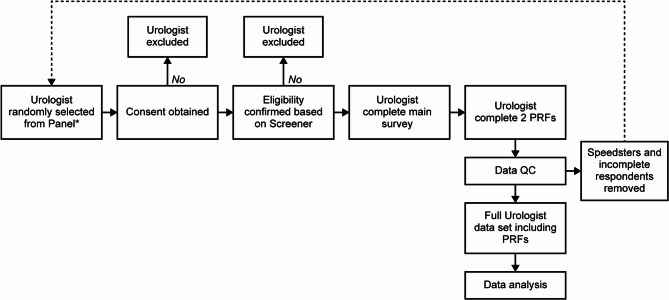 Figure 1
Figure 1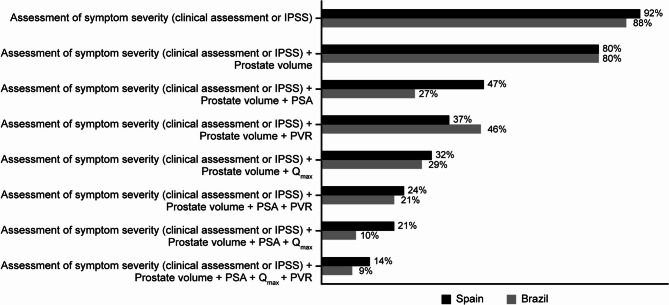 Figure 2
Figure 2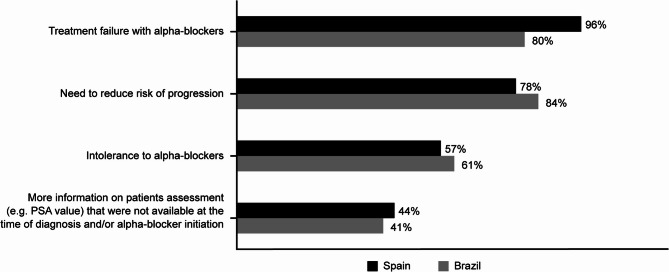 Figure 3
Figure 3- —GSK
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Bladder and Prostate Research · Prostate Cancer Diagnosis and Treatment · Bladder and Urothelial Cancer Treatments
Introduction
Benign prostatic enlargement (BPE) is a progressive condition characterized by reduced urine flow and lower urinary tract symptoms (LUTS) [1]. If left untreated or inappropriately treated, BPE can cause chronic high-pressure retention and long-term changes to bladder function [2–4]. Appropriate and timely treatment of BPE can reduce the risk of worsening LUTS, surgery and quality of life (QoL) deterioration [5, 6].
Treatment with 5alpha reductase inhibitors (5ARIs), as a monotherapy or in combination with alpha blockers, has been shown to improve clinical outcomes in patients with LUTS/BPE at risk of disease progression [7–9]. The American Urological Association (AUA) [5] clinical guidelines recommend that 5ARIs are used to treat patients with moderate-to-severe LUTS, while the European Association of Urology (EAU) [6] clinical guideline recommends that 5ARIs are used to treat men with moderate-to-severe LUTS and an increased risk of disease progression. Risk factors for disease progression can include: prostatic enlargement > 30–40 mL, prostate-specific antigen (PSA) > 1.5 ng/mL, advanced age, larger prostate volume (PV), larger post-void residual volume (PVR), and lower maximal urinary flow rate (Q_max_). However, some patients with risk factors for disease progression do not receive treatment with 5ARIs [10, 11].
The aim of this study was to assess the real-world management of patients with LUTS/BPE treated with 5ARIs by urologists in Spain and Brazil. Urologists responded to a questionnaire and completed patient record forms (PRFs). This study investigated the gap between guideline recommendations and real-world clinical practice to help optimize care for patients with LUTS/BPE at risk of progression.
Methods
Study design
This non-interventional, cross-sectional study gathered data from urologists regarding the management of patients with LUTS/BPE from February–April 2023 (Fig. 1). Data were collected via an online survey comprising a questionnaire and PRFs. The questionnaire was designed to provide an overview of LUTS/BPE diagnosis, management, and monitoring. The PRFs were designed to collect information from each urologist about their two most recent patients with LUTS/BPE aged ≥ 50 who had initiated 5ARI therapy (alone or combination with an α-blocker) in the previous year.Fig. 1. Study design. *Panel size in Spain was approximately 700 urologists; panel size in Brazil was approximately 1920 urologists. Urologists were randomly chosen from each panel and asked to participate in the questionnaire. To achieve the required sample size, 133 urologists were invited to participate in Spain of whom 105 met the inclusion criteria, and 153 were invited in Brazil, of whom 112 met the inclusion criteria. Urologists who did not complete the survey (5 in Spain and 12 in Brazil) were excluded from the final analysis resulting in 100 urologists in Spain and 100 in Brazil included in the final analysis. QC quality check, PRF patient record form
Respondents
Urologists were randomly recruited from Spain and Brazil using country-specific panels internal and external to the IQVIA network. IQVIA, formally known as the Intercontinental Medical statistics [IMS] Health and Quintiles network, is a global provider of advanced analytics, technology solutions, and clinical research services. Urologists provided consent to be contacted via email or telephone for research studies. The panels comprised approximately 700 urologists in Spain and 1920 in Brazil, from which eligible urologists were screened to achieve the target sample size. The survey questions used for screening are detailed in the Supplementary Methods, Additional file 1. Eligible urologists were practicing, with 5‒35 years of experience, spent ≥ 60% of their time in direct patient care, personally provided specialized assistance to ≥ 10 patients with LUTS/BPE in the month prior to the study, and were able to complete PRFs for the two most recent patients with LUTS/BPE aged ≥ 50 years who had initiated 5ARI therapy (alone or combination with an α-blocker) in the previous 12 months. Urologists were excluded if they reported that they had not treated an average of ≥ 10 different patients diagnosed with LUTS/BPE per month in the 12 months prior. Respondents were also excluded from the final analysis if they completed the survey in less than half the average time taken to do so across all respondents.
Primary objective and endpoints
The primary objective of this study was to report real-world practice regarding the management of patients with LUTS/BPE at risk of progression receiving 5ARIs in Spain and Brazil. The key endpoints were to examine: (1) factors considered when assessing the risk of disease progression; (2) how the assessment of disease progression informs decisions about 5ARI treatment; (3) urologist adherence to guideline recommendations; (4) drivers of and barriers to 5ARI prescribing; and (5) patient involvement in treatment decisions. The survey questions used to assess all endpoints are detailed in the Supplementary Methods, Additional file 1.
Ethical approval
This study complied with all applicable laws in the relevant countries regarding participant privacy. Urologists completed consent forms before study participation. All patient data were de-identified so informed consent was not required. A central independent review board (Pearl IRB) considered that the research had no risk or minimal risk to participants and was exempt from most of the requirements of the Federal Policy for the Protection of Human Subjects.
Statistical analysis
A recruitment target of 100 urologists per country was selected based on feasibility assessments with advice from an expert on benign prostatic hyperplasia (BPH) with extensive experience on prevalence of LUTS/BPE and the patient population. To achieve the required sample size, 133 urologists were invited to participate in Spain, of whom 105 met the inclusion criteria, and 153 were invited in Brazil, of whom 112 met the inclusion criteria. Urologists who did not complete the survey (5 in Spain and 12 in Brazil) were excluded from the final analysis resulting in 100 urologists in Spain and 100 in Brazil included in the final analysis. Two PRFs were completed by each urologist, meaning that there were 200 patient cases per country and 400 patient cases reported-upon overall. The statistical analysis was primarily descriptive; frequencies and percentages of responses as well as mean and median thresholds are provided. The margin of error on the analysis performed was determined to be approximately 7% for the given sample size per country, with a 95% confidence interval. Therefore, sample size was considered adequate to support the quantitative analysis in this study. Pearson’s correlation test was used to evaluate the relationship between the proportion of patients at risk of progression and the proportion of patients taking 5ARIs. PASS software (NCSS, LLC, Version 22.0.2) was used for the analyses.
Results
Urologist characteristics and patient demographics
A total of 100 urologists were included from each country (Supplementary Table 1, Additional file 1). Urologists in Spain had an average of 16 years of clinical experience and those in Brazil had 14 years of clinical experience. Most urologists in Spain worked in public practice (87%) and most urologists in Brazil worked in private practice (65%). Across both countries, approximately half of the patients evaluated via PRFs were aged 55–64 years and diagnosed with LUTS/BPE > 1 year prior to study initiation. Most patients had multiple comorbidities, moderate LUTS, and were considered at risk of progression when they initiated 5ARI treatment (82% in Spain and 88% in Brazil; Supplementary Table 2, Additional file 1).
Factors considered when assessing the risk of disease progression
Most urologists reported assessing patients with LUTS/BPE for their risk of disease progression (66% Spain; 75% Brazil, Table 1). The most common reason for not assessing progression in both countries was a lack of time during outpatient visits (55% of urologists in Spain and 52% in Brazil; Supplementary Table 3, Additional file 1).
Table 1. The proportion of patients diagnosed as at risk of progression and/or prescribed 5ARIsSurvey questionSpainBrazilS8Patients with LUTS/BPE treated or managed in the last month, n14968S9Patients with LUTS/BPE currently being treated with 5ARIs, n8054Percentage of patients with LUTS/BPE treated or managed in the last month and currently being treated with 5ARIs, %5479Q1aPercentage of patients with LUTS/BPE assessed for risk of progression, %6675Q2aPercentage of patients with LUTS/BPE diagnosed as at risk of progression, %3942Q10Percentage of patients with LUTS/BPE prescribed 5ARIs, %5056Q11Percentage of patients with LUTS/BPE at risk of progression prescribed 5ARIs, %6581LUTS lower urinary tract symptoms, BPE benign prostatic enlargement, 5ARI 5-alpha-reductase inhibitor
In Spain, 39% of patients diagnosed with LUTS/BPE fulfilled progression criteria and were therefore identified as being at risk of progression (Table 1). From the questionnaires, the most common baseline parameters used to assess the risk of progression in Spain were symptom severity based on the International Prostate Symptom Score (IPSS; 79%), PVR (79%) and PV (78%) (Table 2). The mean thresholds used to decide if patients were at risk of progression for these factors were an IPSS of ≥ 17, PVR of ≥ 111 mL and PV of ≥ 60 mL. From the PRFs, these values were ≥ 20, ≥101 mL and ≥ 82 mL, respectively. PV assessments in Spain were conducted transabdominally (43%), via digital rectal examination (DRE; 32%) or transrectal ultrasound (22%). Baseline PSA levels were used to assess the risk of progression by 65% of urologists in Spain.
Table 2. Factors considered when assessing the risk of disease progression and the thresholds employed in SpainQuestionnairesPRFsQ5a Parameters used to assess risk of progression (%) (n = 100)Q5b Proportion of patients reported assessed with each parameter (%)Mean threshold (SD)Median threshold (Max–Min)Mean threshold (SD)Median threshold (Max–Min)Baseline symptom severity based on IPSS795917 (5.3)18 (30–6)20 (6.2)20 (33–5)Baseline PVR, mL7957111 (37.3)105 (200–25)101 (42.0)100 (200–1)Baseline PV, mL786460 (31.7)50 (153–17)82 (28.6)79 (165–17)Baseline Q_max_, mL/sec75578 (2.7)9 (12–3)7 (2.2)8 (13–2)Baseline PSA, ng/mL65644 (1.8)3 (8–2)4 (1.8)3 (9–1)Symptom deterioration by clinical assessment5168---5 (8–1)Baseline symptom severity based on clinical assessment4767----Age, years476567 (9.7)67 (90–50)--Symptom deterioration while on alpha blocker monotherapy41575 (2.0)5 (9–1)5 (1.5)5 (8–2)Intravesical prostatic protrusion, mm34565 (1.9)5 (10–2)5 (1.8)5 (8–1)Renal function assessment (eGFR)306548 (12.6)50 (77–22)55 (15.9)55 (90–29)Bladder wall thickness measurement, mm10515 (1.7)5 (8–2)5 (2.3)4 (10–1)Frailty phenotype/status944----Presence of metabolic syndrome8613 (0.8)3 (4–2)3 (0.8)3 (4–2)Evidence of chronic intraprostatic inflammation772----PRF patient record form, SD standard deviation, Max-Min* maximum, minimum, IPSS International Prostate Symptom Score, PVR post-void residual volume, PV prostate volume, Qmax maximal urinary flow rate, PSA prostate-specific antigen, eGFR estimated glomerular filtration rate*Mean of reported percentage of patients from responses to the question “What percentage of your BPH patients do you use parameters listed below to assess risk of progression” (Q5A)
Table 3. Factors considered when assessing the risk of disease progression and the thresholds employed in BrazilQuestionnairesPRFsQ5a Parameters used to assess risk of progression (%) (n = 100)Q5b Proportion of patients reported assessed with each parameter (%)Mean (SD)Median (Max–Min)Mean (SD)Median (Max–Min)Baseline PVR, mL836892 (33.7)100 (180–30)93 (37.8)93 (200–13)Baseline PV, mL826556 (18.5)59 (116–29)74 (25.2)67 (180–33)Baseline symptom severity based on IPSS796417 (5.2)19 (30–4)18 (5.3)20 (31–7)Age, years746661 (8.1)60 (82–50)--Baseline symptom severity based on clinical assessment6474----Baseline Q_max_, mL/sec56468 (2.4)9 (15–4)8 (2.2)8 (12–3)Symptom deterioration while on alpha blocker monotherapy51655 (1.7)5 (10–1)5 (2.1)5 (10–1)Baseline PSA, ng/mL49653 (1.4)3 (7–1)4 (1.8)3 (10–1)Symptom deterioration by clinical assessment4871 - - - -Intravesical prostatic protrusion, mm46545 (2.6)5 (10–1)5 (2.7)5 (10–1)Bladder wall thickness measurement, mm45535 (2.2)5 (10–1)5 (1.8)5 (10–1)Renal function assessment (eGFR)306549 (13.2)50 (80–21)49 (15.5)48 (90–15)Presence of metabolic syndrome19403 (0.7)3 (4–2)3 (1.0)3 (4–1)Frailty phenotype/status964----Evidence of chronic intraprostatic inflammation744----PRF patient record form, SD standard deviation, Max-Min maximum/minimum, PVR post-void residual volume, PV prostate volume, IPSS International Prostate Symptom Score, Qmax maximal urinary flow rate, PSA prostate-specific antigen, eGFR estimated glomerular filtration rate*Mean of reported percentage of patients from responses to the question “What percentage of your BPH patients do you use parameters listed below to assess risk of progression” (Q5A)
In Brazil, 42% of patients diagnosed with LUTS/BPE fulfilled progression criteria and were identified as being at risk of progression (Table 1). From the questionnaires, the most common baseline parameters used to assess the risk of progression in Brazil were PVR (83%), PV (82%) and symptom severity based on IPSS (79%; Table 3). The average thresholds used to decide if patients were at risk of progression for these factors were a PVR of ≥ 92 mL, a PV of ≥ 56 mL and an IPSS of ≥ 17. From the PRFs, these values were ≥ 93 mL, ≥ 74 mL and ≥ 18, respectively. PV assessments in Brazil were conducted transabdominally (44%), via DRE (32%) or transrectal ultrasound (10%).
Urologists from both countries most frequently reported that the long-term concerns of managing patients at risk of disease progression were acute and chronic urinary retention and QoL deterioration (Spain: 77%, 76% and 68% respectively; Brazil: 92%, 77% and 76%, respectively; Supplementary Fig. 1A–C, Additional file 1). Fewer noted bladder damage and remodeling as important long-term concerns, with 35% of respondents in Spain and 69% in Brazil rating bladder damage and remodeling as the most important long-term outcome. In the mid-term, urologists were most concerned about symptom deterioration (Spain: 87%, Brazil: 84%; Supplementary Fig. 1D, Additional file 1). When managing patients receiving α-blocker monotherapy, urologists were most often concerned about symptom progression (Spain: 92%, Brazil: 83%) and the risk of disease complications (Spain: 72%, Brazil: 90%; Supplementary Fig. 1E, Additional file 1).
Assessment of diseas progression to infom decisions about 5ARI treatment
In our sample, the total proportion of patients with LUTS/BPE treated with 5ARIs (either alone or combination with an alpha-blocker) each month was 54% in Spain and 79% in Brazil (Table 1). Urologists reported prescribing 5ARIs to approximately half of all patients with LUTS/BPE (50% in Spain, 56% in Brazil) and to a higher proportion of patients diagnosed as being at risk of progression (65% in Spain and 81% in Brazil) via questionnaires.
From the questionnaires, the most common baseline parameters used to guide 5ARI treatment initiation were aligned with those used to assess the risk of progression (Tables 4 and 5) In Spain, the factors most frequently used to guide 5ARI treatment initiation were PV (87%), symptom severity per IPSS (66%) and PVR (60%). The mean thresholds for these factors used to drive 5ARI initiation were a PV of ≥ 59 mL, an IPSS of ≥ 17, and a PVR of ≥ 111 mL. From the PRFs, these values were ≥ 62 mL, ≥ 14 and ≥ 46 mL, respectively (Table 4).
Table 4. Factors considered when making decisions about 5ARI treatment and the thresholds employed in Spain QuestionnairesPRFsQ9a Parameters used to decide risk on 5ARI treatment (%) (n = 100)Mean (SD)Median (Max-Min)Mean (SD)Median (Max-Min)Baseline PV, mL8759 (26.4)51 (147–22)62 (24.4)59 (137–28)Baseline symptom severity based on IPSS6617 (5.6)16 (27–4)14 (6.1)14 (25–2)Baseline PVR, mL60111 (35.2)103 (200–23)46 (41.6)32 (150–8)Baseline PSA, ng/mL593 (1.7)2 (8–1)3 (1.8)2 (7–1)Baseline symptom severity based on clinical assessment58----Baseline Q_max_, mL/sec568 (2.5)9 (12–1)10 (3.3)10 (15–3)Age, years5065 (9.6)65 (86–50)Symptom deterioration while on alpha blocker monotherapy505 (1.5)5 (8–1)4 (2.6)4 (7–1)Symptom deterioration by clinical assessment43---Intravesical prostatic protrusion, mm205 (1.9)5 (10–2)4 (4.1)3 (10–1)Renal function assessment (eGFR)1547 (13.5)50 (62–18)58 (21.1)65 (90–20)Bladder wall thickness measurement, mm84 (1.9)4 (6–1)7 (4.2)7 (10–4)Evidence of chronic intraprostatic inflammation8----Frailty phenotype/status8----Presence of metabolic syndrome52 (0.6)2 (3–2)4 (0.0)4 (4–4)Other2---PRF patient record form, 5ARI 5-alpha-reductase inhibitor, SD standard deviation, Max-Min maximum-minimum, IPSS International Prostate Symptom Score, PV prostate volume, PVR post-void residual volume, PSA prostate-specific antigen, Qmax maximal urinary flow rate, eGFR estimated glomerular filtration rate
Table 5. Factors considered when making decisions about 5ARI treatment and the thresholds employed in Brazil QuestionnairesPRFsQ9a Parameters used to assess risk of progression (%) (n = 100)Mean (SD)Median (Max–Min)Mean (SD)Median (Max–Min)Baseline PV, mL8956 (19.5)50 (124–30)56 (18.3)53 (105–38)Baseline PVR, mL7887 (32.4)100 (153–30)64 (33.2)60 (120–10)Baseline symptom severity based on clinical assessment75----Baseline symptom severity based on IPSS6116 (4.8)17 (24–7)14 (4.6)15 (20–7)Age, years5662 (8.9)60 (85–50) - -Symptom deterioration while on alpha blocker monotherapy595 (2.2)5 (10–1)4 (0.6)4 (5–4)Symptom deterioration by clinical assessment50----Baseline Q_max_, mL/sec498 (2.4)8 (12–3)8 (3.0)9 (13–3)Baseline PSA, ng/mL353 (1.2)4 (7–2)3 (1.1)3 (4–1)Intravesical prostatic protrusion, mm335 (2.4)5 (10–1)4 (1.2)4 (5–3)Bladder wall thickness measurement, mm294 (1.9)4 (10–2)3 (1.2)3 (6–2)Renal function assessment (eGFR)1845 (17.1)50 (70–15)57 (21.9)61 (90–23)Evidence of chronic intraprostatic inflammation8----Presence of metabolic syndrome82 (0.5)2 (3–2)0 (0.0)0 (0–0)Frailty phenotype/status5----Other1----PRF patient record form; SD standard deviation; Max*-Min* maximum, minimum; PV prostate volume; PVR post-void residual volume; IPSS International Prostate Symptom Score; Qmax maximal urinary flow rate, PSA prostate-specific antigen; eGFR estimated glomerular filtration rate
In Brazil, these factors were PV (89%), symptom severity per IPSS (61%) and PVR (78%). The mean thresholds for these factors used to drive 5ARI initiation from the questionnaires were a PV of ≥ 56 mL, an IPSS of ≥ 16; and a PVR of ≥ 87 mL. From the PRFs, these values were ≥ 56 mL, ≥ 14 and ≥ 64 mL, respectively (Table 5).
Urologist adherence to guideline recommendations
Most urologists in both Spain and Brazil (97% and 79%, respectively) reported following AUA and/or EAU guidelines in everyday practice (Supplementary Fig. 2, Additional file 1) and over half of urologists reported that guideline recommendations drove their decisions more than clinical knowledge (62% and 58%, respectively).
From the questionnaires, fewer than half of urologists (47% in Spain and 27% in Brazil) reported using the guideline-recommended combination of IPSS, PSA and PV when making the decision to initiate 5ARIs (Fig. 2). In Spain and Brazil, respectively, the proportion of urologists who additionally included PVR in their assessment was 24% and 21%, and the proportion who additionally included Q_max_ was 21% and 10%. Only 14% and 9% of urologists in Spain and Brazil, respectively, used a combination of all 5 factors: IPSS, PV, PSA, PVR and Q_max_ (Fig. 2).Fig. 2. The individual and combined clinical parameters used by urologists to make 5ARI treatment decisions. 5ARI 5-alpha-reductase inhibitor, IPSS International Prostate Symptom Score, PSA prostate-specific antigen, PVR post-void residual volume, Q_max_ maximal urinary flow rate
Drivers of 5ARI intiation
When selecting treatment, over 40% of urologists from both countries (44% in Spain and 46% in Brazil) reported in the questionnaires that reducing the risk of LUTS/BPE progression and reducing the risk of long-term complications were equally important considerations (Supplementary Fig. 3 A, Additional file 1). This was mirrored in the PRFs: the main reasons for initiating 5ARIs from the PRFs were aiming for sustained symptom relief (70% of urologists in Spain and 71% in Brazil) and a need to reduce the risk of progression (63% of urologists in Spain and 69% in Brazil; Table 6). From the questionnaires, the most common factor considered when switching to 5ARI therapy was treatment failure with α-blockers in Spain (reported by 96% of urologists) and a need to reduce the risk of progression in Brazil (84%; Fig. 3. The main urologist-reported benefit of 5ARI therapy was a reduced risk of LUTS/BPE-related surgery (84% of urologists in Spain and 59% in Brazil; Supplementary Fig. 3B, Additional file 1) and the main patient-perceived benefits reported by urologists were a better QoL (97% of urologists in Spain and 94% in Brazil) and sustained symptom relief (96% in Spain and 95% in Brazil; Supplementary Fig. 3 C, Additional file 1).Table 6. Summary of concerns for progression, drivers for 5ARI initiation and barriers for 5ARI initiation. See supplement for full dataSpainBrazilConcerns for progression most frequently rated ‘highly important’ Acute urinary retention77%92% Chronic urinary retention76%77% Deterioration of quality of life68%76% Chronic kidney failure62%73%Most frequently reported drivers for 5ARI initiation Aiming for sustained symptom relief70%71% Need to reduce risk of progression63%66% Need to reduce risk of complications33%40% High surgical risk/no surgical candidate12%10% Patient expressed preference for a treatment that reduces disease complications12%9% Intolerance to alpha blockers12%5%Barriers to 5ARI initiation most frequently rated ‘highly important’ When the patient is not keen to accept/trade any impact on sexual function46%67% Preference to initiate alpha blockers as a first line32%45% Delay 5ARIs to avoid any impact on sexual function42%43% Patient is not suitable for long-term pharmacologic treatment32%32% Concerns about patient affordability4%34%5ARI 5-alpha-reductase inhibitorFig. 3Factors considered when switching to 5ARI treatment per questionnaires. 5ARI 5-alpha-reductase inhibitor; PSA prostate-specific antigen
Barriers to 5ARI intiation
Almost half of the urologists in Spain (46%) and two thirds in Brazil (67%) reported patient’s unwillingness to accept any impact on sexual function as important to consider when thinking about 5ARI initiation in questionnaire responses (Supplementary Fig. 4A–B, Additional file 1). In Brazil, this view was reflected among 42% of urologists who wanted to delay 5ARI use to avoid an impact on sexual function, as reported in PRFs (Supplementary Fig. 4 C, Additional file 1). A preference to initiate α-blockers as first-line monotherapy was also reported as a key reason for not prescribing 5ARIs, as reported in PRFs (54% of urologists in Spain and 48% in Brazil).
Patient involvement in treatment decision-making
Most urologists in Spain and Brazil (81% and 69%, respectively; Supplementary Fig. 5 A, Additional file 1) reported in questionnaire responses that they usually discuss therapy options with their patients; however, the final treatment decision is generally made by the urologist (54% of urologists in Spain and 66% in Brazil). Urologists in Spain reported in the questionnaire that 25% of discussions with patients ‘always’ led to a change in treatment, and 20% ‘often’ led to a change; these numbers were 20% and 22%, respectively, in Brazil (Supplementary Fig. 5B, Additional file 1). According to PRFs, most urologists discussed treatments with patients (88% in Spain and 93% in Brazil) and some of these discussions led to treatment changes (22% in Spain and 35% in Brazil; Supplementary Fig. 5 C, Additional file 1).
Discussion
This study examined how urologists assess the risk of disease progression in patients with LUTS/BPE, and how that is used to inform 5ARI initiation in real-world clinical practice in Spain and Brazil. Urologists in both countries were generally aware of the need to monitor patients with LUTS/BPE for progression and recognized the benefits of 5ARI treatment. Although most urologists reported following AUA and/or EAU guidelines in everyday practice, we identified specific areas where assessment of the risk of disease progression could be improved, which could optimize access to 5ARI treatment by the right patient at the right time.
In this study, more than two thirds of urologists in both Spain and Brazil reported assessing the risk of disease progression in their patients with LUTS/BPE, with their main concerns being symptom deterioration and manifestations of bladder dysfunction (such as acute or chronic urinary retention). Fewer urologists reported bladder damage and remodeling as an important long-term consideration, which highlights the potential benefit of improved awareness of the consequences of chronic urinary obstruction [12].
Among urologists, the most common parameters used to assess the risk of disease progression were symptom severity (IPSS), PVR and PV, and urologists also widely used their subjective clinical assessment of symptoms. However, less than half of urologists reported using the combination of the three key parameters, IPSS, PSA and PV, recommended by AUA and EAU guidelines to assess the risk of disease progression and inform 5ARI initiation. Most urologists also did not combine these tests with additional factors like Q_max_ and PVR, to better inform the risk of progression. It is likely that this suboptimal approach to assessment of risk of disease progression in patients with LUTS/BPE is a direct consequence of the practical limitations of lack of time and availability of resources (e.g., flowmetry) experienced by healthcare systems.
Data from this study also shows that compared with treatment guidelines, urologists used higher thresholds for key parameters (e.g., PV, PVR) to identify patients at risk of disease progression and initiate treatment with 5ARIs. For example, the average baseline value of PV used to identify patients at risk of progression was 60 mL in Spain and 56 mL in Brazil, compared with the recommended thresholds of 30 mL per the AUA and 40 mL per the EAU guidelines [5, 6]. This difference in threshold between clinical practice and the guidelines was seen in both self-reported questionnaires and analysis of PRFs. It may be that urologists prescribe 5ARIs to patients with PV and PSA levels far above the thresholds recommended by the guidelines because the perceived benefit of treatment in these patients is greater. Potentially, this may mean that patients with relatively smaller prostates and lower PSA levels, who are nevertheless above the thresholds recommended by the guidelines and hence considered to be at risk of disease progression, do not receive 5ARI treatment from which they are likely to benefit. This is consistent with previous observations that patients with progression criteria were not receiving treatment with a 5ARI, either in monotherapy or in combination with an α-blocker, as is recommended by the clinical guidelines [10, 11]. Interestingly, the higher thresholds reported by the urologists in this study to initiate 5ARI treatment closely match the average profile of patients enrolled in landmark studies of 5ARI treatments, including the PLESS trial [7], the phase III trial of dutasteride monotherapy [13], the CombAT trial [8], and the CONDUCT trial [14]. In contrast, the thresholds recommended by the AUA and EAU guidelines reflect the entry criteria for these trials.
This observation reinforces the need for treatment guidelines to be supported by evidence of treatment outcomes at a more individualized patient level rather than by average risk profiles. This would help guide urologists on the relative importance of specific factors when considering 5ARIs and their combination with other therapies. A predictive modeling study in patients receiving either placebo, tamsulosin, dutasteride of a combination of tamsulosin and dutasteride for BPH, the severity of symptoms at baseline was found to be the most important predictor of treatment effect on IPSS change over time while PV, Q_max_ and PVR were most important when predicting the effect of treatment on the risk of acute urinary retention or BPE-related surgery [15]. A follow-up study noted that PVR, age and Q_max_ were predictors of changes in storage and voiding subscores [16].
This study provides useful insights into the factors that inform 5ARI therapy in patients with LUTS/BPE. Urologists in Spain and Brazil reported that the main barriers to starting 5ARI therapy were a reliance on α-blockers as first-line treatment, and the possible impact of 5ARIs on sexual function. These factors may be linked; previous studies have highlighted an impact of 5ARIs but not α-blockers on sexual function [17, 18]. Urologists main reason to switch to 5ARIs was failure to improve symptoms with α-blockers, reflecting evidence that 5ARIs IPSS, improve Q_max_ while decreasing PV and the risk of acute urinary retention and LUTS/BPE-related surgery [19].
In real-world practice, it is likely that urologists and primary care physicians will make treatment decisions holistically, considering both the benefit and the tolerability of the treatment rather than relying on IPSS, PVR and/or PV measurements as risk factors for disease progression. Further studies evaluating the impact of 5ARIs on patients with different levels of risk of progression would help physicians make informed treatment decisions by allowing them to consider the risks versus the benefits of 5ARIs. Additional patient factors (e.g., frailty and aging) and systemic factors (e.g., metabolic syndrome components and indicators of chronic inflammation) may also have an impact on disease progression and treatment decisions for people with LUTS/BPE [20–22]. Further research into these factors is required to fully understand how to optimize disease management.
The care of patients with LUTS/BPE could also be improved by optimizing shared decision-making practices; current guidelines emphasize the importance of patient preference regarding their treatments [23]. However, while most urologists in this study reported providing their patients with details on the therapy options available, few said that these conversations led to changes in treatment [23].
A strength of this study is the use of real-world, clinical practice data from Spain and Brazil, which supports the external validity in those countries. A limitation is that data were self-reported by urologists and may be prone to recall bias; however, analysis of PRFs helps mitigate this with objective data on the treatment decisions made in everyday clinical practice. Additionally, urologists were requested to complete PRFs for only the two most recent eligible patients. This approach may limit the representativeness of the sample, increase the risk of case-mix variability and may not fully capture the diversity of patients managed in routine practice. This study was also subject to selection bias and the sample included is likely not fully representative of urologists practicing in Spain and Brazil. However, these results provide insight into the real-world practice of urologists in two countries with high 5ARI use, which may help guide 5ARI prescribing, and PSA monitoring practices in countries where 5ARI use is less common.
Conclusions
This study assessed the real-world management of patients with LUTS/BPE treated with 5ARIs from the perspective of urologists in Spain and Brazil. Most urologists in both countries were aware of the need to monitor patients with LUTS/BPE for disease progression and recognized the benefits of 5ARI treatment, especially in patients considered at risk of progression. Many urologists reported assessing fewer key risk factors and using higher thresholds than recommended by the guidelines, which may potentially limit the availability of 5ARI treatment for patients at risk of progression who may benefit from treatment. These results highlight the need for ongoing education and optimization of decision making for urologists treating patients with LUTS/BPE.
Supplementary Information
Additional file 1: Management of patients with lower urinary tract symptoms due to benign prostatic enlargement at risk of progression treated with 5-alpha-reductase inhibitors: examining real-world clinical practice in Spain and Brazil
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ng M, Krishna MB, Baradhi KM. Benign Prostatic Hyperplasia. Stat Pearls. https://www.ncbi.nlm.nih.gov/books/NBK 558920/. Stat Pearls. 2022. Accessed 23 Jul 2025.32644346 · pubmed ↗
- 2European Association of Urology EAU Guidelines on non-neurogenic male lower urinary tract symptoms (LUTS). Arnhem. 2024; https://d 56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Non-Neurogenic-Male-LUTS-2024.pdf. Accessed 11 Sept 2025.