Inpatient versus outpatient management of community-acquired acute skin and soft tissue infections. Clinical outcomes and factors associated with eligibility for early discharge
Elena Sendra, Inmaculada López-Montesinos, Estela Membrilla-Fernández, Ana María Gonzalez-Castillo, Francisca Sánchez, Esperanza Cañas-Ruano, Silvia Castañeda, Judith Poblet-Florentin, Rosana Sabaté, Alicia Rodríguez-Alarcón, Sandra Esteban-Cucó, Amaya Suárez

TL;DR
This study compares inpatient and outpatient treatment for skin infections and finds similar outcomes, but social and economic factors affect early discharge eligibility.
Contribution
The study identifies factors influencing early discharge eligibility for SSTI patients and compares clinical outcomes between inpatient and outpatient care.
Findings
No differences in early clinical failure, recurrences, or readmissions between inpatient and outpatient groups.
Hospitalized patients were less likely to revisit the ED for SSTI-related issues.
Social barriers and infection severity were linked to lower eligibility for early discharge.
Abstract
Skin and soft tissue infections (SSTIs) cause an increasing demand for inpatient and outpatient medical care. In recent years, health systems have promoted strategies to treat selected patients on an outpatient basis, which may avoid hospital admissions and associated complications. A retrospective, cohort study of adults presenting to the emergency department (ED) with a SSTI between 2018 and 2020. Primary objective: to compare clinical outcomes in patients with SSTI treated as outpatients or inpatients. Primary outcome: Early clinical failure. Secondary outcomes: Recurrences, unplanned readmissions and ED visits related to the SSTI. Secondary objective: to investigate factors associated with eligibility for early discharge of inpatients. Logistic regression analysis was used to control for confounding factors. Three hundred twenty patients were included, 160 hospitalized. The median…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
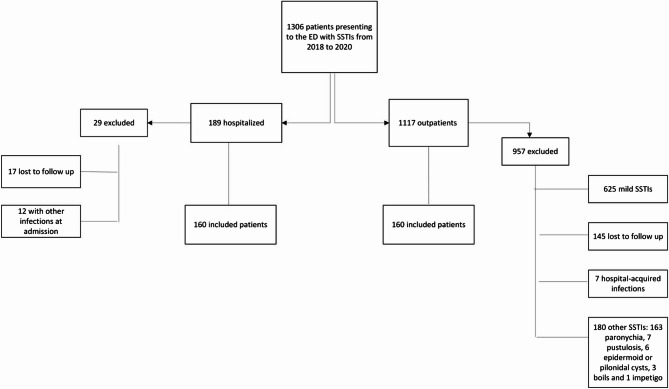 Figure 1
Figure 1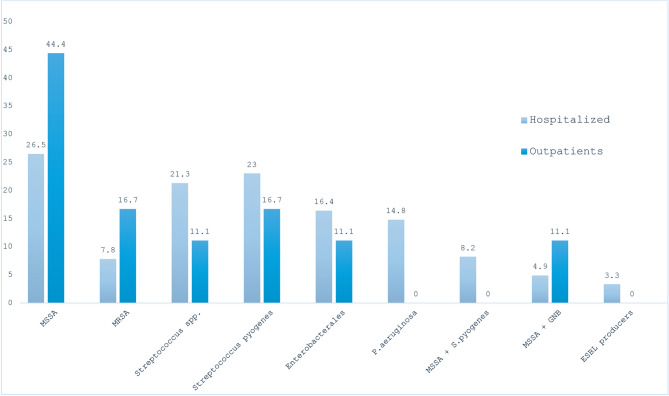 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Streptococcal Infections and Treatments · Antibiotic Use and Resistance
Introduction
Bacterial skin and soft tissue infections (SSTIs) are currently one of the most common reasons for emergency department (ED) visits and subsequent hospital admissions [1]. Studies have reported an increase in the incidence and economic burden of SSTIs in recent years [2, 3]. One of the reasons for this increase is the emergence of community-associated methicillin-resistant Staphylococcus aureus (MRSA) in recent decades [4].
SSTIs are often associated with susceptible populations, such as the elderly, patients with comorbidities, persons who inject drugs (PWID) or are experiencing homelessness [5, 6]. Ambulatory approaches based on outpatient parenteral antimicrobial therapy (OPAT) programs and oral antibiotic switch therapy represent effective alternatives to hospitalization in these patients [7, 8] The recent development of long-acting lipoglycopeptides may be useful in the outpatient management of SSTIs due to their broad activity against Gram- positive cocci (GPC) and long half-lives [9], and particularly useful in patients for whom antibiotic treatment adherence or follow-up is difficult, such as PWID [10].
In recent years, healthcare systems have encouraged ambulatory care practices to reduce the healthcare burden associated with hospitalization. However, few previous studies have set out to analyse the possible predictors that can help identify the subset of patients who may benefit from management in the outpatient setting, based on their risk of clinical failure and/or death [11–14].
We hypothesized that outpatient management is not-inferior to hospitalization in selected patients with community-acquired SSTIs. This study aims to compare differences in clinical outcomes between inpatient and outpatient management of community-acquired SSTIs. The secondary objective is to investigate factors associated with suitability for early discharge in hospitalized patients.
Methods
Setting, study design, and study population
A retrospective, cohort study was conducted from January 2018 to December 2020 at the Hospital del Mar, a 450-bed, tertiary care teaching hospital in Barcelona (Spain). Episodes of SSTIs were identified from the hospital’s documentation service and pertinent data were retrieved from hospital charts, using data from January 2018 to May 2021. All consecutive adult patients aged 18 years or older who presented to the ED with a diagnosis of community-acquired SSTI, including cellulitis/erysipelas, wound infections, necrotizing fasciitis and skin abscesses, were retrospectively reviewed. Patients were including consecutively, starting from the initial data of the study (January 2018) until the required sample size was achieved. Hospital-acquired infections, mild SSTIs, patients with other infections at the time of admission, patients lost to follow-up and patients with a diagnosis of paronychia, pustulosis, lymphangitis, lymphadenitis, boils, carbuncles, impetigo, epidermoid cyst or pilonidal cyst without abscess were excluded. Mild SSTIs were considered when patients did not present with systemic involvement (such as altered mental status, fever, hypotension, or tachycardia), or when no laboratory tests were available to assess systemic involvement through elevated parameters, such as leukocytosis or increased acute-phase reactants (e.g., C-reactive protein or procalcitonin). Outpatient evolution was evaluated during outpatient visits to the hospital and primary care centres by reviewing the patient’s medical records through the electronic health record system of the Catalonia healthcare region. The comprehensive nature of the electronic system allowed for consistent monitoring of outpatient visits and facilitated an in-depth retrospective evaluation of patient outcomes. Patients were followed for up to 30 days after the date of discharge from the hospital. In cases of more than one SSTI episode, the second episode was assessed only if it occurred at least 30 days after discharge from the previous episode and if the first episode had previously resolved.
This article was written according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) (Supplementary material, Table S1).
Outcomes
Primary outcome was early clinical failure assessed 72 h after initiation of antibiotic therapy. Clinical failure was defined as the presence of one of the next criteria: the appearance of new symptoms or signs of infection, persistence or worsening of previous signs and symptoms, change in antibiotic treatment to rescue therapy and/or death.
Secondary outcomes were recurrences, unplanned readmissions and ED visits related to the SSTI in the follow-up period.
Clinical variables and definitions
Demographic and clinical data and the Charlson comorbidity severity index were collected [15]. Previous episodes of SSTIs and history of recurrent SSTIs were also recorded. Baseline disease severity in acute infection was estimated by the following scores: the Sequential Organ Failure Assessment (SOFA) [16]; Quick SOFA score (qSOFA) [16]; Simplified Acute Physiology Score (SAPS II) [17] and the Pitt index [17] in case of bacteremia.
For the classification of SSTIs, cellulitis or erysipelas were defined as diffuse skin infection characterized by spreading areas of erythema, edema and/or induration; surgical or trauma-related wound infection was defined as infection with purulent drainage or the presence of one or more fluid collections associated with a surgical or post-traumatic wound with surrounding erythema, edema and/or induration; skin abscess was defined as an infection characterized by a collection of pus within the dermis or deeper, accompanied by erythema, edema, and/or induration, and necrotizing fasciitis was defined as a rapidly spreading skin and soft tissue infection, with progressive destruction and necrosis of the fascia and fat, with significant associated systemic toxicity [18, 19].
Reasons for admission to the hospital via the ED were classified based on electronic medical records, and comprehensive firsthand data were collected for each patient by trained investigator. Reasons were classified as: complicated infection or suspected complicated infection (deep soft tissue involvement in a patient with underlying pathology requiring intravenous antibiotic therapy and/or surgery), sepsis [20], social conditions, chronic diseases decompensation, high Charlson score or advanced age, oral intake unavailable, colonization or risk factors for multidrug-resistant infection, nonadherent patient, immunosuppression and lack of improvement after 48–72 h of treatment.
Risk factors for multidrug-resistant infection were considered in patients with previously prolonged hospitalization and/or antimicrobial exposure, invasive procedures and prior colonization or infection [21]. Immunosuppression was defined by corticosteroid use, receipt of chemotherapy or radiation therapy, diagnosis of human immunodeficiency virus or acquired immunodeficiency syndrome, absolute neutrophil count of less than 1,500/mcL, or prior solid organ or bone marrow transplantation with receipt of chronic immunosuppression [22].
Empirical antibiotic treatment was defined as antibiotics administered in the first hours of infection if cultures were not available. Definitive antibiotic treatment was defined as antibiotics administered according to the results of the antimicrobial susceptibility testing if cultures were available. Appropriate treatment was defined as antibiotic therapy administered if cultures were available and at least one of the antibiotics administered had in vitro activity against the isolated strain, according to the breakpoints established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) [23]. Antibiotic rescue therapy was defined as escalation or new empirical rescue therapy, evaluated between 24 and 72 h after the antibiotic therapy was initiated. Antibiotic adverse effects (i.e., nephrotoxicity, Clostridioides difficile infection, allergic reaction) were also recorded. Adequate source control, if required, was defined as percutaneous drainage or surgical intervention, as appropriate.
Clinical cure was defined if the following criteria within 72 h of initiation of antibiotic therapy were met: the patient remained afebrile (temperature less than 37.3 °C) for at least 24 h, no increase in lesion size compared to the ED consultation, decrease in the extent and intensity of one or more signs of inflammation at the primary site of infection and white blood cell (WBC) count was between 4 × 10^9/L and 12 × 10^9/L. This last criterion was added to the clinical data based on previous references [24–28]. An indeterminate clinical response was established in patients lost to follow-up. Recurrence was defined as relapse of symptoms after initial improvement of the first episode during the follow-up period. Length of hospital stay and complications during the 30 days after the onset of infection were also recorded.
Finally, in hospitalized patients a subgroup analysis was made and eligibility for early discharge (at 72 h from admission) was evaluated. The patients were eligible for early discharge if the following criteria were met: clinical cure within 72 h, absence of sepsis, septic shock and/or multiple organ failure, absence of comorbidity decompensation, no changes in cognitive or mental status or any other situation that would compromise adherence to medication at home.
Microbiological studies
Bacterial identification was performed by conventional biochemical tests and matrix-assisted laser desorption and ionization time-of-flight mass spectrometry (MALDI-TOF MS), using the Bruker Microflex^®^ LT instrument and MALDI Biotyper^®^ software (Bruker Daltonics, MA, USA). Antibiotic susceptibility testing (AST) of isolates was performed by broth microdilution, using MicroScan panels [Beckman-Coulter] on the automated MicroScan WalkAway system [Beckman-Coulter]. Results were interpreted according to EUCAST guidelines [23].
Statistical analysis
The required sample size was estimated at 160 patients per group and a maximum difference of 10% was considered clinically relevant. An alpha error of 0.05 and a beta error of 0.20 were set. It was calculated using a non-superiority test based on the hypothesis that the percentage of readmissions in the outpatient group would not be higher than in the hospitalized group. The results of a previous study [29] found a readmission rate of 21% in the outpatient group and 24% in the inpatient group.
Categorical variables were presented as numbers and percentages and were compared using the X^2^ test or Fisher’s exact test. Continuous variables were expressed as median and interquartile range (IQR) and compared using Student’s t-test or the Mann–Whitney U test, as appropriate.
Univariate and multivariate logistic regression analyses were used to assess associations between covariates and primary and secondary outcomes. Variables associated significantly or nearly significantly in the univariate analysis, and those that were clinically relevant but not statistically significant were included in the model. No missing imputation was applied. To avoid collinearity between related variables (homelessness and social/economic barriers), only one was included in the multivariate analysis. Results were expressed as odds ratios (OR) and their 95% confidence intervals (95% CI). Statistical analyses were performed using SPSS Statistics 26.0 software, R 4.0.0, and STATA 15.1.
Ethics
This study was conducted in accordance with national and international guidelines of the Deontological Codel, the Declaration of Helsinki (Fortaleza, Brazil, October 2013), the Code of Good Research Practices, and Royal Decree 957/2020 of November 3rd. The study was approved by the Clinical Research Ethics Committee of the Parc de Salut Mar, Barcelona (register no. 2021/10132). Due to the observational nature of the study and retrospective analysis, the need for written informed consent was waived.
Results
Demographics and clinical characteristics
One thousand three hundred six patients attending the ED with SSTIs during the study period were screened. However, the vast majority of the patients did not met inclusion criteria for our study and were not included. The main reason for exclusion was the presence of mild infections that did not meet the study’s inclusion criteria. Finally, of the 1.306 patients, 320 fulfilled the inclusion and exclusion criteria and were included, of whom 50% (160 patients) were admitted in the hospital (Fig. 1). Nineteen patients (11.9%) were admitted to OPAT. Table 1 shows the differences between the groups.Fig. 1. Flowchart of patients included in the study. Abbreviation: SSTIs: Skin and soft tissue infectionsTable 1Baseline characteristics of patients included in the study and comparative analysis according to management Overall cohort (n=320)Hospitalization (n=160)Outpatients (n=160)p-valueDemographics and social conditions Age (years), m (IQR)62 (46–76)55 (40.25–71.25)0.035 Male sex95 (59.4)105 (65.6)0.248 Drug injection history19 (11.9)13 (8.1)0.264 Homelessness26 (16.3)13 (8.1)0.026 Social and economic barriers to care31 (19.4)12 (7.5)0.002Underlying condition Charlson Comorbidity Index, m (IQR)3 (1–5)2 (0–4)0.110 Diabetes mellitus41 (25.6)32 (20)0.231 COPD7 (4.4)10 (6.3)0.455 Congestive heart failure11 (6.9)12 (7.5)0.829 Cirrhosis10 (6.3)4 (2.5)0.101 Neurological disorder14 (8.8)11 (6.9)0.532 Chronic kidney disease23 (14.4)11 (6.9)0.029 Dialysis3 (1.9)4 (2.5)1.000 Hematologic malignancy1 (0.6)4 (2.5)0.371 Solid tumor malignancy6 (3.8)13 (8.1)0.098 Mental illness11 (6.9)6 (3.8)0.213Immunosuppression27 (16.9)24 (15)0.647 Neutropenia0 (0)1 (0.6)1.000 HIV/AIDS10 (6.3)12 (7.5)0.659 Kidney transplant6 (3.8)1 (0.6)0.121SSTI classification Cellulitis/Erysipelas126 (78.8)132 (82.5)0.479 Surgical or traumatic wound infection0 (0)6 (3.7)0.030 Skin abscess18 (11.2)16 (10)0.856 Necrotizing fasciitis2 (1.3)0 (0.0)0.498 Cellulitis + abscess14 (8.8)6 (3.8)0.106Localization Upper extremities12 (7.5)20 (12.5)0.192 Lower extremities133 (83.1)116 (72.5)0.031 Other10 (6.25)23 (14.4)0.027 Various localizations5 (3.12)1 (0.62)0.214Portal of entry Surgical or traumatic wound43 (26.9) 45 (28.1)0.900 Ulcer 36 (22.5)12 (7.5)<0.001 Fungal infection20 (12.5)3 (1.9)0.001 Skin lesion8 (5)11 (6.9)0.636 Other10 (6.2)16 (10)0.306 Unknown43 (26.9)73 (45.6)0.001Predisposing factors Lymphedema6 (3.8)4 (2.5)0.748 Venous insufficiency13 (8.1)15 (9.4)0.843 Obesity3 (1.9)6 (3.8)0.502 Trauma6 (3.8)10 (6.3)0.623 Skin disease7 (4.4)5 (3.1)0.556 Fungal infection16 (10)3 (1.9)0.002 Diabetic foot4 (2.5)1 (0.6)0.371 Stasis dermatitis1 (0.6)2 (1.3)1.000 Drug injection-related wound12 (7.5)9 (5.6)0.498 Others22 (13.8)13 (8.1)0.152 None46 (28.7)84 (52.5)<0.001 Various factors28 (17.5)3 (1.9)<0.001HCA Risk Factors Hospitalization in last 3 months23 (14.4)16 (10)0.232 Surgery in last 3 months3 (1.9)10 (6.3)0.047 Residence in a long-term care facility6 (3.8)0 (0)0.030 Antibiotic exposure in last 3 months59 (36.9)47 (29.4)0.154 Admission to long-term care facility3 (1.9)0 (0)0.248Previous episodes of SSTIs53 (33.1)22 (13.8)<0.001Recurrent SSTIs44 (27.5)13 (8.1)<0.001Laboratory parameters on ED admission CRP,m (IQR) (mg/dL)11.5 (5.3–22.36)5.1 (2.4–10.6)<0.001 WBC,m (IQR) (x10E3/µL)14.3 (9.3–18.9)10.7 (7.7–13.1)<0.001 Positive culture64 (40)18 (11.3)<0.001 Blood culture11 (16.9)2 (11.1)0.724 Drainage culture21 (32.3)11 (61.1)0.051 Wound smear culture30 (46.2)5 (27.8)0.260 Various cultures3 (4.6)0 (0)1.000Baseline Disease Severity SOFA score, m (IQR)0 (0–1)0 (0-0)0.018 qSOFA score, m (IQR)0 (0-0)0 (0-0)0.002 SAPS II, m (IQR)26 (19–31.75.75)19 (19–28)<0.001 Sepsis or septic shock11 (6.9)0 (0)0.002 ICU admission5 (3.1)0 (0)0.061 Bacteraemia12 (7.5)2 (1.3)0.006 Pitt score, m (IQR)0 (0-0)0 (0-0)0.220Management Appropriate treatment58 (90.6)12 (66.6)<0.001 Inappropriate treatment3 (4.6)7 (38.8)0.218 72 h delay in initiating appropriate antibiotic therapy5 (7.8)0 (0)0.576Source control Surgery26 (16.5)1 (0.6)<0.001 Percutaneous drainage7 (4.4)16 (10)0.055 Not required125 (79.1)143 (89.4)0.012 Inadequate3 (1.9)0 (0)0.248Discharge against medical advice16 (10)7 (4.4)0.051Outpatient treatment Oral antibiotic76 (47.5)157 (98.1)<0.001 Day-care hospital1 (0.6)0 (0)1.000 “Hospital at home” program3 (1.9)0 (0)0.248 Not completed2 (2.5)7 (4.5)0.722 Completed57 (71.3)134 (85.4)0.009 Unknown21 (26.3)16 (10.2)0.001Antibiotic Rescue Therapy Yes12 (7.5)21 (13.1)0.098 No144 (90)139 (86.9)0.382 Unknown4 (2.5)0 (0)0.123Antibiotic-related side effects16 (10)8 (5)0.093 Acute kidney injury2 (12.5)0 (0)0.520* Clostridioides difficile3 (18.8)0 (0)0.280 Diarrhea negative for Clostridioides difficile4 (25)3 (33.3)0.673 Allergic reaction4 (25)5 (55.6)0.200 Other3 (18.8)1 (11.1)1.000Data are presented as nos. (%) unless otherwise specifiedAbbreviations*: AIDS acquired immunodeficiency syndrome, COPD chronic obstructive pulmonary disease, CRP C-reactive protein, ED emergency department, HCA healthcare-acquired, HIV human immunodeficiency virus, ICU intensive care unit, IQR interquartile range, m median, SAPS II Simplified Acute Physiology Score, SOFA Sequential Organ Failure Assessment, SSTI(s) skin and soft tissue infection(s), WBC white blood cell count
In the hospitalized group, the most common reasons for admission to hospital were (patients could have more than one reason for admission): complicated infection or suspected complicated infection (31/160, 19.3%), colonization or risk of infection with multidrug-resistant microorganisms (27/160, 16.8%), consultation to the ED due to lack of improvement after 48–72 h of treatment (27/160, 16.8%), chronic diseases decompensation (23/160 14.3%), risk of non-adherence to treatment (15/160, 9.3%), social and economic barriers to regular care (15/160, 9.3%), sepsis or septic shock (11/160, 6.8%), immunosuppression (7/160, 4.3%) and advanced age/high Charlson score (12/160, 7.5%).
In hospitalized patients, 31 had complications related with the admission. The most frequent complications were phlebitis (9/160, 5.6%), delirium (8/160, 5%) and nosocomial infections (7/160, 4.3%). In the OPAT cohort only one patient with phlebitis had a health-care related complication during admission.
The median length of hospital stay was 9 days (IQR 5–15), and 20/160 patients (12.5%) were discharged within the first 72 h. Ninety seven out of 160 (60.6%) hospitalized patients were not eligible for early discharge. The most common reasons for ineligibility for early discharge were (patients could have more than one reason): clinical cure criteria not met (25/97, 25.7%), need for parenteral antibiotic therapy or wound care (21/97, 21.6%), social and economic barriers to regular care (13/97, 13.4%), sepsis/septic shock (11/97 11.3%), chronic diseases decompensation (10/97, 10.3%), cognitive or mental disorders (7/97, 7.2%) and alcohol or substance use disorder (3/97, 3%). Parenteral antibiotic therapy was required for one or more of the following reasons: suspicion of infection with a multidrug-resistant organism (based on colonization, positive culture results, known risk factors or prior treatment failure), for which effective treatment options were limited to the parenteral route; and the patient’s inability to tolerate oral intake. Twenty-three patients (7%) left against medical advice; 16/23 (69.5%) of this group were PWID and/or homeless.
Baseline illness severity, microbiological information and therapeutic management
At the time of first assessment, hospitalized patients were more seriously ill, as indicated by worse laboratory parameters (CRP and WBC, p < 0.001 in both cases), higher severity scores (SOFA (p = 0.018), qSOFA (p = 0.002) and SAPS II (p < 0.001)) and a higher proportion of sepsis or septic shock (p < 0.001). Among inpatients, 11 patients (6.9%) had sepsis or septic shock but only 5 patients (3.1%) required admission to the ICU.
Among patients with microbiological results (82/320, 25.6%), Staphylococcus aureus was the most common pathogen isolated in both groups. Figure 2 shows the microbiological data by study group.Fig. 2. Microbiological data by study group (hospitalized vs. outpatients). Abbreviations: GNB (gram negative bacilli), ESBL (extended- spectrum beta-lactamases), MRSA (methicillin-resistant Staphylococcus aureus), MSSA (methicillin-susceptible Staphylococcus aureus), P. aeruginosa (Pseudomonas aeruginosa). All MRSA isolates were susceptible to clindamycin and trimethoprim/sulfamethoxazole, and 3/8 isolates (37.5%) were susceptible to levofloxacin. For vancomycin, half the strains (4/8) had a minimum inhibitory concentration (MIC) = 1 µg/ml and the other half had a MIC = 2 µg/ml. Among Enterobacterales, 10/15 (66%) were resistant to amoxicillin/clavulànic acid, 5/15 (33.3%) were resistant to ciprofloxacin. In Pseudomonas aeruginosa infections, 4/9 (44.4%) were resistant to ciprofloxacin
The most common empiric antimicrobial therapies used in hospitalized patients were amoxicillin/clavulanic acid (75/160, 46.9%), ciprofloxacin plus clindamycin (23/160, 14.4%), piperacillin/tazobactam (21/160, 13.1%), piperacillin/tazobactam plus vancomycin (17/160, 10.6%) and ceftriaxone plus clindamycin (10/160, 6.3%). Among admitted patients with microbiological isolation (n = 64), 90.6% received appropriate antibiotic treatment. In the outpatient setting, the most common antibiotics used were oral amoxicillin/clavulanic acid (116/160, 73.9%) and oral ciprofloxacin plus clindamycin (28/160, 17.8%). Two patients were managed with long-acting lipoglycopeptides (both dalbavancin as outpatients).
Primary objective: clinical outcomes
Early clinical failure
Clinical failure assessed 72 h after initiation of antibiotic therapy was 20.7% (31/150) and 17.3% (26/150) in the outpatient and inpatient groups, respectively (p = 0.467). Among patients admitted to OPAT, 2/19 (10.5%) had early clinical failure.
The unadjusted and adjusted analysis of variables associated with clinical failure are shown in Table 2. After adjusting for confounders in multivariate analysis, there were no differences according to management in early clinical failure. Clinical failure was independently associated with diabetes mellitus (OR 2.75, 95% CI 1.29–5.87; p = 0.009).Table 2. Univariate and multivariate analysis of parameters predicting early clinical failure Early clinical failure cohort sample (n= 300)Clinical Failure (n =57)Non-Clinical Failure (n =243) Unadjusted OR (95% CI) p-valueAdjusted OR (95% CI)p-valueManagement Outpatient31 (20.7)119 (79.3) - -1.00 Hospitalization26 (17.3)124 (82.7)0.80 (0.45–1.44.45.44) 0.4670.68 (0.37–1.26)0.223Demographics and social conditions Age (years), m (IQR)59 (44–76)59 (44–74)1.00 (0.98–1.02) 0.9700.99 (0.97–1.02)0.606 Male sex39 (21.4)143 (78.6) --1.00 Female sex18 (15.3)100 (84.7)0.66 (0.36–1.22) 0.1860.71 (0.37–1.37)0.311 History of drug injection 9 (32.1)19 (67.9)2.21 (0.94–5.18)0.0821.70 (0.59–4.91)0.324 Homelessness11 (34.4)21 (65.6)2.53 (1.14–5.60)0.030 2.66 (0.99-7.10)0.052 Social and economic barriers to care10 (27.8)26 (72.2)1.78 (0.80–3.93)0.170Underlying conditions Charlson Comorbidity Index, m(IQR)2.00 (0–6)2 (0–4)1.06 (0.96–1.16) 0.2661.07 (0.91–1.26)0.433 Diabetes mellitus 21 (30)49 (70) 2.31 (1.24–4.31) 0.0112.75 (1.29–5.87)0.009 COPD 6 (37.5)10 (62.5)2.74 (0.95–7.88)0.078 Congestive heart failure 1 (4.55)21 (95.5)0.19 (0.02–1.43) 0.061 Cirrhosis 1 (7.69)12 (92.3)0.34 (0.04–2.70) 0.316 Neurological disorder 5 (20.8)19 (79.2)1.13 (0.40–3.18)0.787 Chronic kidney disease 9 (27.3)24 (72.7)1.71 (0.75–3.91)0.216 Hematologic malignancy 2 (40) 3 (60)2.91 (0.47–17.8) 0.291 Solid tumor malignancy 3 (15.8)16 (84.2)0.79 (0.22–2.80)0.759 Mental illness 5 (35.7)9 (64.3)2.50 (0.80–7.77)0.136Immunosuppression11 (25)33 (75)1.52 (0.72–3.23.72.23)0.283 HIV/AIDS1 (6.67)14 (93.3)0.29 (0.04–2.27)0.223 Neutropenia0 (0)1 (100)0.00 (0.00;.)0.810 Kidney transplant1 (14.3)6 (85.7)0.71 (0.08–5.98)0.829SSTI classification Cellulitis/Erysipelas44 (18.2)198 (81.8)-- Surgical or traumatic wound infection2 (33.3) 4 (66.7) 2.25 (0.40–12.7.40.7) 0.388 Skin abscess11 (22)39 (78) 1.27 (0.60 −2.67)0.527 Necrotizing fasciitis0 (0)2 (100) 0.00 (0.00;.)0.671Localization Lower extremities44 (18.9)189 (81.1)-- Upper extremities4 (13.8)25 (86.2)0.69 (0.23–2.08)0.533 Other7 (21.9)25 (78.1)1.20 (0.49–2.96)0.675 Various localizations2 (33.3)4 (66.7)2.15 (0.38–12.1)0.413Portal of entry Surgical or traumatic wound20 (25)60 (75)-- Ulcer11 (22.9)37 (77.1)0.89 (0.38–2.07)0.801 Fungal infection1 (4.35)22 (95.7) 0.14 (0.02–1.08)0.025 Skin lesion3 (15.8)16 (84.2) 0.56 (0.15-2.13)0.420 Others6 (23.1)20 (76.9)0.90 (0.32–2.55)0.865 Unknown16 (15.4)88 (84.6)0.55 (0.26–1.14)0.110Predisposing factors None21 (17.2)101 (82.8) -- One or more factors36 (20.2)142 (79.8)1.22 (0.67–2.21)0.521Previous episodes of SSTIs13 (18.3)58 (81.7)0.94 (0.47- 1.87)0.881Recurrent SSTIs10 (19.2)42 (80.8)1.02 (0.48–2.18) 0.944Hospital-at-home2 (10.5)17 (89.5)0.48 (0.11–2.15)0.355Voluntary discharge7 (53.8)6 (46.2)5.53 (1.78–17.2)0.005 Baseline illness severity SOFA score, m (IQR)0 (0–1)0 (0–1)1.00 (0.80–1.26) 0.979 SAPS II24 (19–30)24 (19–30) 1.01 (0.98–1.04)0.670 Sepsis1 (25)3 (75)1.42 (0.14–13.9)0.740 Septic shock1 (14.3)6 (85.7)0.71 (0.08–6.01.0)0.833 ICU admission1 (20)4 (80)1.07 (0.12–9.73)0.896 Bacteremia 5 (35.7)9 (64.3)2.50 (0.80–7.77)0.136Therapeutic management Appropriate treatment15 (22.1)53 (77.9)1.31 (0.67–2.55)0.426 72 h delay in initiating appropriate antibiotic therapy2 (40)3 (60)2.56 (0.39–17)0.371Source control Not required47 (18.7)205 (81.3)-- Surgery8 (32)17 (68)2.05 (0.84–5.04)0.1320.132 Percutaneous drainage1 (4.55)21 (95.5)0.21 (0.03.1.58)0.0850.085Data are presented as nos. (%) unless otherwise specifiedAbbreviations: AIDS acquired immunodeficiency syndrome, COPD chronic obstructive pulmonary disease, ED emergency department, HIV human immunodeficiency virus, ICU intensive care unit, IQR interquartile range, m median, SAPS II Simplified Acute Physiology Score, SOFA Sequential Organ Failure Assessment, SSTI(s) skin and soft tissue infection(s)
Secondary outcomes: recurrences, unplanned readmissions and ED visits related to the SSTI
Recurrence was 7.5% (12/160) and 12.3% (19/155) in the outpatient and inpatient groups, respectively (p = 0.163). Among patients admitted to OPAT, recurrence was 5.26% (1/19). Unplanned readmissions related to the SSTI were 16.2% (26/160) and 17% (27/159) in the outpatient and inpatient groups, respectively (p = 0.862). Among patients admitted to OPAT, 15.8% were readmited (3/19). ED visits related to the SSTI were 25.6% (41/160) and 17.5% (28/160) in the outpatient and inpatient groups, respectively (p = 0.079). Among patients admitted to OPAT, 15.8% (3/19) visited the ED in the follow-up period (3/49).
The unadjusted and adjusted analysis of variables associated with recurrences, unplanned readmissions and ED visits related to the SSTI are shown in Suplementary Tables S2, S3 and S4, respectively. After adjusting for confounders in multivariate analysis, there were no differences according to management in recurrence and unplanned readmissions.
Recurrence was independently associated with history of recurrent SSTIs (OR 5.86, 95% CI 2.51–13.67; p < 0.001). Unplanned readmissions were indepently associated with diabetes mellitus (OR 2.04, 95% CI 1.01–4.10; p = 0.046) and SOFA score (OR 1.25, 95% CI1.01–1.53; p = 0.039).
Hospitalization was independently associated with ED visits related to the SSTI with inpatients showing significantly lower odds of ED revisits (OR 0.32, 95% CI 0.16–0.62; p = 0.001). Moreover, ED visits related to the SSTI were indepently asociated with homelesness (OR 3.35, 95% CI 1.32–8.46; p = 0.011) and history of recurrent SSTIs (OR 6.47, 95% CI 3.05–13.71; p < 0.001).
Secondary objective: independent factors associated with eligibility for early discharge in hospitalized patients
Sixty-three out of 160 (39.3%) hospitalized patients were eligible for early discharge. Crude and adjusted analyses of variables associated with meeting the eligibility criteria for early discharge are shown in Table 3. In the multivariate analysis, immunosuppression was independently associated with fulfilling the criteria for eligibility for early discharge (OR 3.02 95% CI 1.13–8.10; p = 0.028). SAPS II score (OR 0.92 95% CI 0.88–0.96; p < 0.001) and social and economic barriers to regular care (OR 0.19 95% CI 0.07–0.54; p = 0.002) were associated with not fulfilling the criteria for eligibility for early discharge.Table 3. Univariate and multivariate analysis of parameters predicting fulfillment of eligibility criteria for early discharge in hospitalized patientsTotal cohort (n = 160), met eligibility criteria for early discharge =83)Criteria met (n =83)Criteria not met (n =77) Unadjusted (95% CI)OR p-valueAdjusted OR (95% CI)p-valueDemographics and social conditions Age (years), m (IQR)63 (48–71)64 (46–79.50) 1.02(1.00–1.04)0.033 Female sex34 (41)31 (40.2)0.97(0.52–1.83)0.9290.92 (0.45–1.90)0.827 History of drug injection 6 (7.2)13 (16.9) 2.61(0.94–7.25)0.066 Homelessness8 (9.6)18 (23.4)2.86(1.16–7.03)0.021 Social and economic barriers to care9 (10.8)22 (28.6)3.29(1.41–7.70)0.0050.19 (0.07-0.54)0.002Underlying conditions Charlson Comorbidity Index, m(IQR)3 (1–4)3 (1–6)1.15 (1.02–1.29)0.024 Diabetes mellitus17 (20.5)24 (31.1)1.76(0.86–3.61)0.128 COPD2 (2.4)5 (6.5)2.81 (0.53–14.9)0.239 Congestive heart failure5 (6)6 (7.8)1.32 (0.39–4.51)0.673 Cirrhosis3 (3.6)7 (9)2.67 (0.66–10.7)0.173 Neurological disorder7 (8.4)7 (9)1.09(0.36–3.25)0.886 Chronic kidney disease10 (12)13 (16.9)1.48(0.61–3.61)0.396 Dialysis2 (2.4)1 (1.3)0.53(0.05–6.00)0.665 Hematologic malignancy0 (0)1 (1.3) -0.481 Solid tumor malignancy2 (2.4)4 (5.2)2.22(0.39–12.5)0.394 Mental illness4 (4.8)7 (9)1.98(0.55–7.03)0.309Immunosuppression19 (22.9)8 (10.3)0.39(0.160-0.95)0.0373.02 (1.13–8.10)0.028 HIV/AIDS6 (7.2)4 (5.2)0.70(0.19–2.59)0.618 Kidney transplant3 (3.6)3 (3.9)1.08(0.21–5.52)0.929HCA Risk Factors Hospitalization in last 3 months14 (16.8)9 (11.7)0.65(0.26–1.61)0.363 Surgery in last 3 months 1 (1.2)2 (2.6)2.19(0.19–24.6)0.581 Antibiotic exposure in last 3 months38 (45.7)21 (27.3)0.44(0.23–0.86)0.0161.69 (0.80–3.58)0.169Previous episodes of SSTIs30 (36.1)23 (29.9)0.75(0.39–1.46)0.406Recurrent SSTIs24 (29)20 (26)0.86(0.43–1.73)0.683Laboratory parameters on ED admission CRP, m (IQR) (mg/dL)11.8 (3.5–23.1)14.9 (6.3–27.8)1.00(0.99–1.01)0.874 Leukocytes, m (IQR) (x10E3/µL)13.6 (10.5–18.4) 14.9 (9.2–19.7)1.03(0.98–1.08.9)0.249Positive culture28 (33.7)36 (46.7)1.72(0.91–3.27)0.097 Blood culture3 (10.3)8 (22.2)2.42(0.50–11.8)0.299Baseline illness severity SOFA score, m (IQR)0 (0-0)1 (0–2)1.72(1.24–2.39)0.001 SAPS II24 (19–30)29 (19–36)1.07(1.03–1.11)0.0010.92 (0.88–0.96.)**<0.001 **Management Appropriate treatment25 (43.1)33 (56.9) 0.66(0.06–7.69)0.794Source control16 (48.5)17 (51.5)1.15(0.53–2.48)0.724 Surgery12 (46.2)14 (53.8)1.26(0.54–2.95)0.596 Percutaneous drainage4 (57.1)3 (42.9)0.81(0.17–3.78)0.810Antibiotic Rescue Therapy2 (16.7)10 (83.3)5.75(1.22–27.2)0.016Antibiotic-related side effects4 (25)12 (75)3.65(1.12–11.8)0.027Data are presented as nos. (%), unless otherwise specifiedAbbreviations: AIDS acquired immunodeficiency syndrome, COPD chronic obstructive pulmonary disease, CRP C-reactive protein, ED emergency department, HCA healthcare-acquired, HIV human immunodeficiency virus, IQR interquartile range, ICU intensive care unit, m median, SAPS II Simplified Acute Physiology Score, SOFA Sequential Organ Failure Assessment, SSTIs skin and soft tissue infections
Discussion
In the present study comparing the management of community-acquired SSTIs, we found no differences in early clinical failure, recurrence and unplanned readmissions between inpatients and outpatients. Numerous studies have set out to analyse the clinical characteristics and various outcomes in SSTIs, but to our knowledge, few have compared the differences between inpatient and outpatient approaches. After reviewing the literature, we found only one previous study, by Bookstaver et al., that compared the two groups [29]. They found that hospitalized patients were older and had more comorbidities than outpatients. No differences in unplanned ED visits or readmissions were observed between the groups. Consistent with these results, no differences were observed in the present study in either early clinical cure, recurrences, and readmissions related to the SSTI. Alternatively, in the current study patients who were hospitalized had significantly reduced odds of returning to the ED for SSTI-related concerns, suggesting a protective effect of hospitalization. This finding may be related with the higher rate of appropriate treatment in inpatients. On the contrary, some outpatients may return to the ED early after starting oral antibiotics, before sufficient time has passed for clinical improvement, as defervescence can be slower. This early reconsultation may reflect caution rather than true treatment failure.
In the present cohort, hospitalized patients had higher severity scores at the onset of infection, as assessed by SOFA, qSOFA and SAPS II scores. In addition, infection severity evaluated by SAPS II score was associated with not meeting the eligibility criteria for early discharge and severity evaluated by SOFA score was associated with unplanned readmissions related to the SSTIs. Despite the high frequency of SSTIs in the community, there is no validated score to assess the severity of infection and guide decisions about where patients should receive care. Several severity scoring systems have been developed but none has been validated in prospective multicentre cohort studies or clinical trials [30]. Furthermore, although 39% of hospitalized patients fulfilled predefined criteria for early discharge, only 12.5% were actually discharged within the first 72 h. This discrepancy reflects the gap between clinical eligibility and real-world practice. Several contributing factors have been described, including institutional and structural barriers, as well as logistical and social challenges [31].
In the present and other series, homeless patients and patients with economic/social barriers to regular care, such as those with a history of injecting drug use, represent a vulnerable population with a dramatic increase in the incidence of SSTIs and hospitalization in recent years [32]. Many of these patients use strategies to delay or avoid seeking medical attention due to fear of stigma and discrimination from healthcare professionals, as well as structural barriers to accessing medical care [33]. As a result, these patients have increased disease severity, longer courses of antibiotics and hospitalizations, high readmission rates and lack of appropriate follow-up [34]. In this study, patients with social and economic barriers to regular care were associated with a lower likelihood of being eligible for early discharge and homeless patients were associated with a higher probabilty of returning to the ED attributable to the SSTIs. In addition, 11/32 (34%) of those classified as PWID were discharged against medical advice, which is slightly higher than the rates of up to 30% reported in previous studies [34, 35].
Retrospective reports of newer long-acting antibiotics have shown the effectiveness and safety of these agents in the general population [36] and similar or even better results in terms of efficacy, safety and reduction in length of hospital stay compared to standard-of-care in patients with social and economic barriers to care and PWID [37]. Therefore, long-acting glycopeptides could be a useful treatment option in patients with low adherence, but further multicentre prospective studies are needed to confirm the results.
SSTIs are among the most common infections treated in OPAT units [38]. In a recent systematic review and meta-analysis of clinical trials comparing the efficacy and safety of OPAT versus inpatient parenteral antimicrobial therapy, no differences were found for mortality, treatment failure or adverse reactions related to antimicrobials, or the device used to administer them [8]. In the present cohort, 19 patients were enrolled in the OPAT program. Early clinical cure in this group was 89.5%, which is similar to previously published studies [39, 40]. Secondary to the SSTI 15.8% visited the ED and 15.8% of the patients were readmitted in the 30-day follow-up period. In another series, the readmission rates for patients with SSTIs ranged from 0% to 21% [39, 41–43]. In the OPAT cohort, none of the patients was PWID. Regarding the management of PWID in the outpatient setting, there is evidence that OPAT may be safe in these patients [44]. However, other studies have reported that PWID patients may not adhere to treatment and so experience readmissions and catheter-related complications such as drug relapse [45].
Finally, regarding the aetiology of SSTIs in this population, S. aureus and Streptococcus were the most common isolates among patients with microbiological data, with a rate of 40.2% (34.3% in hospitalized patients and 61% in outpatients) of S.aureus isolates and 39% (84.3% in hospitalized patients and 15.6% in outpatients) of Streptoccus isolates. Among S. aureus isolates, methicillin-susceptible Staphylococcus aureus was more prevalent than MRSA (25/33, 75.7%, vs. 8/33, 24.2%). The rates of S.aureus in hospitalized patients were similar to those reported in other European studies [46] and significantly lower than those reported in North America, with values ranging from 35.9% to 81% of specimens isolated by culture [46, 47]. Among outpatients, the rate of S. aureus in the present study was significantly higher than that reported in previous studies, with values around 39% [48]. Previous reports of MRSA in SSTIs in Spain have found rates from 13 to 24.6% of the S. aueus isolates [49], while in Europe the rates rise to 29% with large variations among countries (higher prevalences in the Southern countries) [46]. In Latin and North America, the rates are more worrisome, with reports of rates up to 59% in North America [46] and up to 88% in Latin America with significant regional difference [50]. For gram-negative bacteria, Enterobacterales were isolated in 17% of cultures and Pseudomonas aeruginosa in 14.8% of hospitalized patients, rates consistent with previous studies in Europe and North America [46].
This study has some limitations that should be acknowledged. First, those related to the retrospective design with possible reporting bias. Outpatient evolution was assessed through visits to the hospital and primary care centers by reviewing patients’ medical records through the electronic health record system of the Catalonia healthcare region. However, in some cases, early clinical response may not have been assessed precisely at the 72-hour mark. Second, the higher rate of appropriate antibiotic treatment observed in the hospitalized group may reflect the use of broader-spectrum empirical therapy in these patients, who generally present with greater severity of illness and higher comorbidity. As a result, the improved appropriateness of initial treatment in this group could have contributed to better outcomes introducing potential performance bias. Third, we highlight possible selection biases; as this was a single-centre study including an idiosyncratic population attributable to an area of influence of Barcelona with a high prevalence of patients with social and economic barriers to care and PWID. In addition, necrotizing fasciitis is an infection that always requires hospital admission, although it may initially be managed in the outpatient setting until a definitive diagnosis is established. Therefore, these results may not be generalizable to other hospitals with different populations. Fourth, the sample size calculation was not based on the primary outcome, clinical failure, but rather on the secondary outcome of readmission. This was due to the lack of published studies specifically evaluating clinical failure, which limited our ability to estimate an expected effect size. Although this approach ensured sufficient statistical power, it may reduce the precision of our findings related to the primary outcome and affect the robutness of our study. Finally, the present study was conducted between 2018 and 2020. In 2020, the SARS-CoV-2 outbreak became a global pandemic [51] and the number of SSTI visits to the ED and hospitalizations may have decreased due to the prioritization of outpatient management. In addition, the use of long-acting glycopeptides was still infrequent in our hospital during the study period. Therefore, the outpatient management performed in the present study may not accurately reflect the management performed today, with more common use of long-acting antibiotics. However, several strengths of this study can be highlighted. Although previous reports have analysed the characteristics of SSTIs in inpatients and outpatients, to our knowledge, this is one of the first studies to compare differences between groups. Finally, we analysed factors associated with suitability for potential early discharge, a strategy that can be used by health care systems to reduce the burden associated with hospital admissions.
Conclusions
The present study found no differences in early clinical failure, recurrences and unplanned readmissions related to the SSTI between inpatients and outpatients in community-acquired SSTIs. Social and economic barriers to regular care and infection severity were identified as factors associated with unsuitability for early discharge in hospitalized patients.
These results warrant further investigation to establish standard criteria for hospital admission in SSTIs. Expanding outpatient management by using resources such as early discharge and switching to oral therapy, long-acting glycopeptides, and OPAT may represent an opportunity to reduce the healthcare burden, while improving patient adherence to care and clinical outcomes.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
Supplementary Material 4.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peterson RA, Polgreen LA, Cavanaugh JE, Polgreen PM. Increasing Incidence, Cost, and seasonality in patients hospitalized for cellulitis. Open Forum Infect Dis. 2017 Feb 8;4(1)ofx 008.10.1093/ofid/ofx 008PMC 541402428480281 · doi ↗ · pubmed ↗
- 2Tran TT, Gomez Villegas S, Aitken SL, Butler-Wu SM, Soriano A, Werth BJ et al. New perspectives on antimicrobial agents: Long-Acting lipoglycopeptides. Antimicrob Agents Chemother. 2022 Jun 21;66(6)(6):e 0261420.10.1128/aac.02614-20PMC 921141735475634 · doi ↗ · pubmed ↗
- 3Guidance for industry acute bacterial skin and skin structure infections: Developing drugs for treatment. 2013. Available from: https://www.fda.gov/drugs/guidance-compliance-regulatory-information/guidances-drugs. Cited 2 Aug 2024.
- 4The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MI Cs and zone diameters. Version 13.0. 2023. http://www.eucast.org.
- 5Stevens DL et al. Clin Infect Dis (2014; 59:147–59). Clinical Infectious Diseases. 2015;60(9):1448–1448.10.1093/cid/civ 11425725056 · doi ↗ · pubmed ↗
- 6Bookstaver PB, Jenkins TC, Stenehjem E, Doron S, Brown J, Goldwater SH et al. Impact of outpatient vs inpatient ABSSSI treatment on outcomes: A retrospective observational analysis of medical charts across US emergency departments. Open Forum Infect Dis. 2018 May 15;5(7)ofy 109.10.1093/ofid/ofy 109PMC 629946030581883 · doi ↗ · pubmed ↗
- 7Gonçalves-Bradley DC, Lannin NA, Clemson L, Cameron ID, Shepperd S. Discharge planning from hospital. Cochrane Database Syst Reviews. 2022 Feb 24;2(2):CD 000313. 10.1002/14651858.CD 000313.pub 6PMC 886772335199849 · doi ↗ · pubmed ↗
- 8Vazquez Deida AA, Shihadeh KC, Preslaski CR, Young HL, Wyles DL, Jenkins TC. Use of a standardized Dalbavancin approach to facilitate earlier hospital discharge for vulnerable patients receiving prolonged inpatient antibiotic therapy. Open Forum Infect Dis. 2020 Jul 13;7(8):ofaa 293.10.1093/ofid/ofaa 293PMC 741530432793767 · doi ↗ · pubmed ↗