Analysis of factors influencing innovative behaviors of intensive care unit nurses using a random forest model-a multicentre cross-sectional study
Wen-Jie Ge, Zhi-Min Cao, Xin-Yi Zhu, Shou-Jun Zhu

TL;DR
This study identifies key factors influencing innovative behaviors in ICU nurses using a random forest model to guide targeted interventions.
Contribution
The novel use of a random forest model to rank factors influencing innovation behaviors in ICU nurses.
Findings
Spiritual climate was the most important factor influencing innovative behavior among ICU nurses.
Information literacy, thriving at work, and education level significantly contributed to innovation behavior.
A combination of six factors explained 55.7% of the variation in innovative behavior.
Abstract
To identify and rank the key determinants-including sociodemographic factors, Spiritual Climate, Information Literacy, and Thriving at Work-of Innovative behaviours among intensive care nurses, and provide a theoretical basis for targeted interventions. Nurse innovation behavior is essential for the development of the nursing discipline; yet, significant progress in enhancing the innovation behavior of Intensive care nurses has been limited over the past few decades. Nurses must identify deficiencies and areas for improvement within the intensive medical care system while performing care practices. For nurses to identify solutions to these issues through an innovative approach, they must adopt innovative behaviors. A multicentre cross-sectional study was conducted. We gathered data from a convenient sample of 587 Intensive care nurses from twenty-three hospitals of grade 2 A and above…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
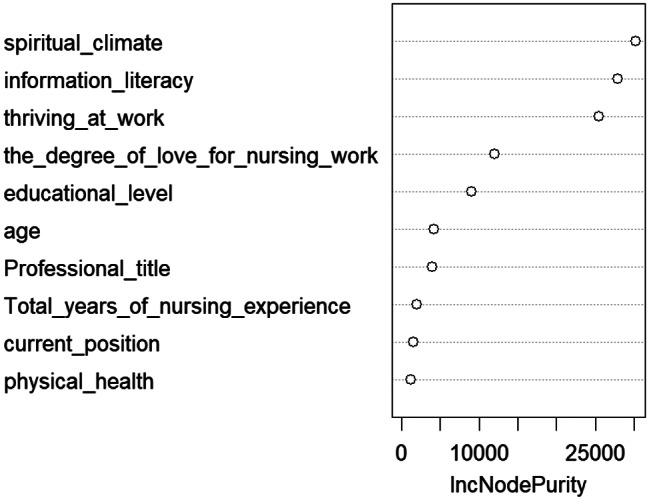 Figure 1
Figure 1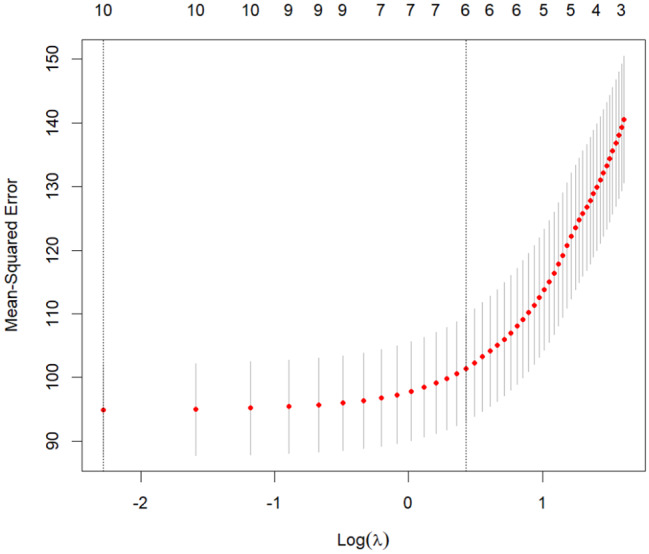 Figure 2
Figure 2- —This work was supported by Scientific Research Project of Anhui Provincial of China Department of Education
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNursing education and management · Health Sciences Research and Education · Family and Patient Care in Intensive Care Units
Introduction
Amid rapid advancements in health technology and rising healthcare demands, hospitals must enhance their efficiency, innovation capabilities, and value [1]. The sustainable development and innovation of healthcare organizations depend on building innovative healthcare teams [2]. As essential members of these teams, clinical nurses possess unique work characteristics—sustained patient contact and the delivery of comprehensive care—enabling them to identify opportunities for improvement in clinical practice and thus drive innovation to enhance healthcare service quality [3]. Nurses, who represent the largest segment of the global healthcare workforce, play a crucial role in advancing healthcare innovation [4]. Nurses’ innovative behavior refers to the process of nurses’ behavior based on the needs of health promotion and disease prevention and control, through exploring and developing innovative nursing technologies and practice models, introducing and applying them to their work under the mechanism of collaborative cooperation, which mainly consists of 3 stages: generating ideas, obtaining support, and realizing ideas [5, 6]. Asurakkody et al. [7] reported that the consequences of innovative behavior included increased job productivity, lower levels of job burnout, higher job satisfaction, improved ability to solve organizational problems, increased organizational commitment, and enhanced organizational efficiency and effectiveness. A recent study emphasised that the innovative behavior of nurses plays a significant role in shaping their productive performance [8]. The American Nursing Association’s “2024 ANA Enterprise Strategic Plan” lays out a goal to raise nursing’s professional standards globally, with an emphasis on developing nurses who can use creative nursing techniques in complex and dynamic settings to improve public health outcomes [9]. Meantime, China’s National Health Commission has issued the ‘National Nursing Development Plan (2021–2025)‘ [10], focusing on the new expectations of the people in the field of nursing, grasping the characteristics of nursing work, innovating the nursing service model, and striving to promote the reform and development of the nursing service industry. The intensive care unit (ICU) is a specialized department that provides care and treatment for the most critically ill patients due to its advanced and unique facilities. With the rapid advancements in science and technology, the ICU has evolved into a highly specialized field, creating a complex and often stressful work environment [11]. The inherent complexity of care in these units makes them susceptible to errors and adverse events. Epidemiological data indicate that ICUs report the highest incidence rates of adverse events among hospital departments, with prevalence rates ranging from approximately 17% to 31% for incidents such as pressure ulcers, patient falls, and hospital-acquired infections [12]. Research has demonstrated that innovation in intensive care nursing plays a crucial role in improving access to healthcare services, enhancing care quality, and increasing treatment efficiency and productivity [13]. Consequently, for ICU nurses, innovative behavior is not an optional ‘add-on’ but a core professional competency essential to safeguard patient safety and enhance the quality of care in high-stakes situations.
“Innovation in intensive care nursing” can be defined as the application of novel ideas, techniques, or procedures to address the critical needs of individuals, reduce healthcare costs, and enhance efficiency [14]. The innovative behavior of ICU nurses is positively associated with higher-quality care, as shown in various studies, mitigating complications, improving patient outcomes, and shortening hospitalization duration, thereby contributing to a more comfortable recovery experience [15–17]. However, despite its critical importance, the level of innovative behavior among ICU nurses remains insufficient. A national survey conducted in China by Gao et al. (2016) revealed that only 12.00% of ICU nurses demonstrated strong innovative behaviors, with the majority adhering to fixed nursing procedures and engaging in limited technical innovation [18]. This underscores a notable gap between the demand for innovation in critical care environments and nurses’ current levels of innovation. Compounding this issue, while innovative behavior in the general nursing population has been studied extensively, there remains limited research focused specifically on the unique cohort of intensive care nurses [19, 20].
Therefore, given the critical role of innovation in ICU settings and the identified gaps in both practice and research, it is both valuable and necessary to conduct a focused investigation into the factors influencing innovative behavior among intensive care nurses, with the ultimate aim of developing targeted strategies to enhance it. Several sociodemographic factors [6], such as gender, age, position, marital status, health status, and level of education, have been suggested to influence nurses’ innovative behavior; however, the results of studies of the effects of demographic characteristics on nurses’ innovative behavior have been mixed. Li et al. (2025) found no significant effect of age or position on nurses’ innovative behavior [21], but another study reported that these factors were associated with innovative behavior [22]. These findings indicate that the factors affecting innovative behavior warrant further investigation and offer guidance for identifying potential variables.
Literature review
Antecedents to innovative behavior, comprising organizational, work environment, and individual characteristics, represent key factors affecting innovation [7]. Within these domains, nurses’ information literacy [23, 24], thriving at work [25], and spiritual climate [12, 26, 27] constitute critical variables, each representing a distinct level of influence on innovative behavior (individual, organizational, and work environment).
For individuals, information literacy is the foundation for lifelong learning and contributing to the knowledge society, encompassing the comprehensive performance of individuals in effectively acquiring and utilizing information in conjunction with their own needs [28]. Given the significance of innovative behavior among Intensive care nurses, information literacy—as an individual characteristic—is recognized as a key factor in generating innovative ideas to enhance such behavior. Information literacy refers to the ability of nursing professionals to accurately and comprehensively retrieve, objectively evaluate, and effectively apply information to resolve clinical dilemmas [29]. Information literacy serves as a critical mediating factor between workplace learning determinants and innovative outcomes, thereby enhancing both knowledge creation and the development of practical solutions [23]. Wang et al. (2025) demonstrated that Information Literacy positively influences the innovative behaviors of clinical nurses [24]. Fundamentally, enhanced information literacy among ICU nurses signifies their advanced capabilities in acquiring, managing, and effectively utilizing information. This proficiency serves as a catalyst for innovation and the development of valuable clinical resources, thereby fostering greater awareness of innovation and strengthening systemic innovation capacity within critical care settings. Advancing information literacy enables ICU nurses to translate evidence into practice more effectively, cultivating research capabilities foundational to innovation.
The rapid development of positive psychology in modern high-pressure, high-intensity work environments has drawn extensive scholarly attention to the concept of positive variables. Thriving at work is a key concept in positive organizational behavior, describing the continuous psychological states of vigor and learning that individuals experience at work, in which they feel energized and acquire new skills, thereby enhancing their development and performance. Vigor, the affective dimension of thriving at work, refers to an individual’s positive feeling of having available energy. Learning, the cognitive dimension, pertains to an individual’s sense of acquiring and effectively applying knowledge and skills [30, 31]. Numerous studies have shown the positive effects of thriving at work on nurses. Liu et al. [25] found that nurse leaders with a platform leadership style can facilitate the demonstration of innovative behaviors by enhancing subordinate nurses’ thriving at work, based on a survey of 428 nurses. Thriving at work enhances nurses’ job performance and reduces work withdrawal behaviors [32, 33]. With the increasing Thriving at Work of clinical nurses, they will, on the one hand, have great enthusiasm for their work and the goals of the department and the hospital, and become more devoted to them; on the other hand, they will feel their actual growth and thus have a stronger sense of self-efficacy for the development of innovative work. Although the correlation between thriving at work and innovative behaviors has been confirmed, few studies have examined this relationship among ICU nurses. Within the high-stress context of the ICU, thriving at work is likely a significant factor influencing ICU nurses’ innovative behavior.
A growing number of scholars are focusing on spiritual climate, and the inquiry into how to cultivate a favorable one in the workplace has emerged as a prominent research topic across multiple disciplines. Spiritual climate refers to an organization that respects and encourages employees to express their inner thoughts, fostering a spiritual culture that directly affects employee work engagement [34, 35]. By increasing employee engagement at work, employees can be motivated to perform their jobs more effectively, thereby promoting innovation [36]. In a 2024 study, Zhang et al. [26] found a significant positive correlation between spiritual climate and the innovative behaviors of ICU nurses. Moreover, studies by Hashemian et al. [20] and Lu et al. [27] have confirmed that work environment factors influence nurses’ innovative behavior, and that an excellent organizational climate enhances nurses’ level of innovative behavior. These results provide a theoretical framework for understanding how the spiritual climate influences innovative behavior.
Although the correlations among nurses’ information literacy, spiritual climate, thriving at work, and innovative behavior have been confirmed, few studies have integrated these factors specifically among ICU nurses. In the complex and high-acuity ICU environment, the interplay of these variables may manifest in distinct patterns that influence innovative behaviors differently than in general ward settings. In addition, few studies have systematically ranked the importance of factors identified as influencing ICU nurses’ innovative behavior. The random forest model is a commonly used machine learning method for variable screening. By constructing multiple decision trees into an integrated learning framework, it can effectively handle complex, nonlinear relationships. It can accurately rank the importance of influencing factors and is highly efficient when dealing with large datasets and high-dimensional features [37, 38]. LASSO regression can exclude unimportant variables, greatly simplify the relationship between dependent and independent variables, prevent overfitting, and provide a reliable technical approach for the multifactorial analysis of ICU nurses’ innovative behaviors. Based on this, this study employs a Lasso regression model to identify key factors associated with innovative behaviors among ICU nurses. It applies a random forest algorithm to rank the relative importance of these factors, thereby providing evidence-based insights for the development of targeted, individualized interventions to promote innovation in ICU nursing practice.
Objectives and methods
Study design
We conducted a cross-sectional study on China ICU nurses. A STROBE checklist was used as the guideline in this study.
Participants
This study involved 587 ICU nurses from twenty-three grade 2 A and above hospitals in Anhui Province, China, who were selected using a convenience sampling method. The inclusion criteria were as follows: (1) Obtained a professional qualification certificate for nurses; (2) Worked in an ICU for at least 6 months; (3) Given informed consent and voluntarily participated in this study. Exclusion criteria: Non-working nursing staff during the survey period. According to the sample size estimation requirements for multiple linear regression analysis studies, the sample size for the study was calculated using an estimation method that requires the sample size to be ten to twenty times the number of questionnaire items [39]. This study included a total of 23 independent variables. Taking into account a 20% loss in the visit rate, the required sample size was calculated to be between 276 and 552 cases. The actual survey was conducted with 587 ICU nurses, which met the sample size requirement.
Data collection and survey instruments
The questionnaires used in this study included sociodemographic information, the Spiritual Climate Scale, the Information Literacy Scale, the Thriving at Work Scale, and the Innovative Behaviour Inventory.
Participant demographic information questionnaire
The questionnaire was drafted following discussions among research team members and primarily comprises 11 questions: gender, age, hospital rank, job nature, current position, education level, professional title, total years of nursing experience, whether or not you are an ICU nurses specialist, the degree of love for nursing work, and physical health.
Thriving at work scale
The Thriving at Work Scale was developed by Porath et al. (2012) [31] and translated and revised by Han et al. (2020) [40] to measure the level of Thriving at Work of employees, including two dimensions, the learning dimension (5 items) and the vitality dimension (5 items), with a total of 10 entries, each of which is scored on a 7-point Likert scale ranging from “strongly disagree” to “strongly agree” on a scale of 1 to 7, with entries 4 and 8 being reverse-scored entries. The total score ranges from 10 to 70, with higher scores indicating a higher level of Thriving at Work. The Cronbach’s alpha value for this scale is 0.771. The Cronbach’s alpha coefficient of this scale in this study was 0.902 for the overall scale, and the Cronbach’s alpha coefficients of the learning and vitality dimensions were 0.776 and 0.873, respectively.
Information literacy scale
The Information Literacy Scale, created by Shu (2009) [29] comprises four dimensions: information consciousness (4 items), information ability (6 items), information knowledge (6 items), and information morals (4 items), totaling 20 items. A 5-point Likert scale was employed, with “totally disagree” assigned 1 point and “totally agree” assigned 5 points. The total score ranged from 20 to 100, with higher scores indicating greater information literacy among nurses. The reliability (cronbach alpha) coefficient of the original form of the scale was found to be 0.911 [41]. The overall Cronbach’s alpha coefficient for the scale in this study was 0.967, while the coefficients for the dimensions of information consciousness, information ability, information knowledge, and information morals were 0.846, 0.952, 0.915, and 0.879, respectively.
Spiritual climate scale
The “Spiritual Climate Scale ” developed by Doram et al. (2017) [42] and adapted into China by Wu (2019) [43] was used to measure spiritual climate among healthcare workers. The scale consists of four items and one dimension, which are: I am encouraged to express spirituality in this clinical area; My spiritual views are respected in this clinical area; My spirituality has a comfortable home in this clinical area; and A diverse set of spiritual views are accepted in this clinical area. The Likert 5-point scale was used, with all items being positive questions, ranging from “strongly disagree” to “strongly agree,” scored from 1 to 5 points respectively. The average score of the four questions was subtracted by 1 and multiplied by 25 to obtain the final score, with a total score ranging from 0 to 100 points, where higher scores indicate better mental climate status among nurses. The Cronbach’s α value of the scale is 0.833. The overall Cronbach’s α coefficient of the scale in the present study was 0.964.
Innovative behavior inventory
Innovative Behavior Inventory (IBI) is a 20-item scale compiled by Martin Lukes and Ute Stephan (2017) [44]. The Chinese version scale was revised by Huang et al. (2021) [45], including five dimensions: idea generation and search(6 items), plan communication and implementation(5 items), involving others (3 items), overcoming obstacles(3 items) and clinical application (3 items), with a total of 20 entries. Each item was rated on a 5-point Likert scale from “not at all” to “strongly agree,” with a total score of 15 to 75, with higher scores indicating higher levels of innovative behavior. The Cronbach’s α coefficient for the Chinese version of the scale was 0.95 [46]. The overall Cronbach’s alpha coefficient for the scale in this study was 0.988. Finally, the reliability (cronbach’s alpha) coefficient for each dimension of the scale were determined as 0.970, 0.958, 0.955, 0.944, and 0.948, respectively.
Random forest algorithm
The core idea of the Random Forest model is to calculate the model accuracy by building multiple decision trees, each based on modeling a different random subset of the training data, with the unextracted data serving as the test set. By integrating the predictions from multiple decision trees, the final prediction is typically selected through a voting process. The study ranks the importance of influencing factors based on mean decrease accuracy [37].
Participants and data collection
Data was collected via the Chinese internet platform ‘Wenjuanxing’ (https://www.wjx.cn), which facilitates the creation of electronic questionnaires and the generation of matching QR codes. The cross-sectional survey method was used for data collection in this study. The survey was implemented by members of the team (including the first author and two uniformly trained investigators) through an electronic questionnaire platform. The researchers contacted the nursing management personnel of the hospital to provide a detailed explanation of the study’s purpose and significance, as well as obtain their consent. A head of the ICU nursing unit was designated as the survey leader in each of the twenty-three hospitals, with clear communication regarding the study’s objectives, voluntary participation principle, respondent inclusion/ exclusion criteria, anonymity principle, guidelines for answering questions and data collection specifications. The study protocol was communicated to the nursing staff of the undergraduate unit by the head nurse, focusing on the principles of anonymity, single-device IP-limited answers, and the breakpoint renewal function. The research team monitored the dynamics of questionnaire submission in real-time through the back-end management system and set 72 consecutive hours without new data as the survey termination point. The data quality control link utilizes a two-person blind checking mechanism to exclude four questionnaires that were not completed or exhibited irregular responses. A total of 591 electronic questionnaires were distributed, and 587 valid questionnaires were ultimately included, resulting in an effective response rate of 99.33%.
Ethics approval and consent to participate
This study was conducted following the ethical principles required in the Declaration of Helsinki and approved by the ethical committee of the First Affiliated Hospital of the University of Science and Technology of China (ethical approval number: 2025-ky222). All participants were informed of the research objective, volunteered to participate in this survey, and had the right to refuse participation at any time. Informed consent was obtained from all participants. The study data are strictly confidential and are for research use only.
Statistical analysis
The results were exported directly from Wenjuanxing and analysed using SPSS 22.0. There were no missing values for all available data, as required fields were set at the time of data collection. Measurement data conforming to a normal distribution were expressed as mean ± standard deviation. Independent sample t-tests and one-way ANOVAs were used for comparison between groups, and the Pearson method was chosen for correlation tests. Taking the total number of innovative behaviors as the dependent variable, the statistically significant indicators (P < 0.05) from the one-way analysis of variance and correlation test were used as the set of predictor variables. Firstly, the randomForest program package in R Studio 4.3.2 software was used to construct a random forest model comprising 500 decision trees to obtain variable importance scores. At the same time, the glmnet package was used to implement LASSO regression for feature dimensionality reduction. Finally, the common predictors identified by the two algorithms were incorporated into the multiple linear regression model, and the prediction equations were established using the stepwise regression method. Differences were deemed statistically significant at p < 0.05.
Results
Comparison of nursing innovation behaviour inventory among ICU nurses with different characteristics
Consequently, 587 valid questionnaires were obtained, resulting in an effective response rate of 99.33%. The age range of the participants was 20–56 years, with a mean age of 31.63 years (SD 5.352). There were 105 males and 482 females. This study categorized ICU nurses and compared their innovative behavior ratings based on demographic parameters, occupational characteristics, and physical health. Only statistically significant items are listed in this study. For more information, see Table 1.
Table 1. Demographic characteristics and innovation behaviour of ICU nursesDemographic characteristicsN(%)Score (M ± SD)F/t P Age (years old)7.684<0.001≤ 255667.21 ± 17.98926∼3022976.09 ± 15.09331∼3519378.02 ± 14.10236∼407377.92 ± 10.686≥ 413681.42 ± 10.149Education level24.203<0.001Junior college or below10167.60 ± 17.180Bachelor’s47678.34 ± 13.341Master’s or above1074.50 ± 16.188Professional title12.219<0.001Nurse6868.15 ± 17.638Senior nurse24575.87 ± 14.610Nurse-in-charge24978.41 ± 13.238Deputy chief nurse or above2584.76 ± 9.628Current positionClinical nurse53275.47 ± 14.862-8.087<0.001Head Nurse5585.73 ± 8.102Total years of nursing experience (years)8.221<0.001<614572.88 ± 16.6346∼1021175.11 ± 15.21311∼1516379.28 ± 12.674≥ 166881.28 ± 9.840Physical health6.5540.002Good40677.55 ± 14.813Fair16974.59 ± 13.353Worse1264.58 ± 20.170The degree of love for nursing work82.429<0.001Like21983.45 ± 14.500More like24976.86 ± 9.789Not sure7966.78 ± 8.804Don’t like4054.43 ± 18.174
Descriptive statistics of thriving at work, information literacy, spiritual climate and innovation behaviour
In this study, the total scores for Thriving at Work Scale were (54.33 ± 10.15), for Information Literacy Scale were (76.39 ± 12.94), for Spiritual Climate Scale were (71.53 ± 19.82), and for Innovation Behaviour were (76.43 ± 14.67) (Table 2).
Table 2. Scores of thriving at work, information literacy, spiritual climate, and innovation behaviour (n = 587)VariablesItemsScoring rangeScore X ± SAverage score X ± SThriving at work1012–7054.33 ± 10.155.43 ± 1.01Information literacy2022–10076.39 ± 12.943.82 ± 0.65Spiritual climate40-10071.53 ± 19.8217.88 ± 4.96Innovation behaviour2020–10076.43 ± 14.673.82 ± 0.73Idea generation and search61–523.05 ± 4.543.84 ± 0.76Plan communication and implementation51–519.07 ± 3.783.81 ± 0.76Overcoming obstacles31–511.55 ± 2.293.85 ± 0.76Clinical application31–511.45 ± 2.273.82 ± 0.76Involving others31–511.31 ± 2.383.77 ± 0.79
Correlation analysis of thriving at work, information literacy, spiritual climate and innovation behaviour
The correlation analysis results indicate significant positive correlations among Thriving at Work, Information Literacy, Spiritual Climate, and Innovation Behaviour. Thriving at work is positively correlated with Innovation Behaviour (r = 0.618, p < 0.001); thriving at work is positively correlated with information literacy (r = 0.723, p < 0.001); thriving at work is positively correlated with Spiritual Climate (r = 0.780, p < 0.001); information literacy is positively correlated with Innovation Behaviour (r = 0.627, p < 0.001); information literacy is positively correlated with Spiritual Climate (r = 0.706, p < 0.001); Spiritual Climate is positively correlated with Innovation Behaviour (r = 0.652, p < 0.001) (Table 3).
Table 3. Correlation coefficients among thriving at work, information literacy, spiritual climate, and innovation behaviour (n = 587)Variables1234Thriving at work1.000Information literacy0.723^^1.000Spiritual climate0.780^^0.706^^1.000Innovation behaviour0.618^^0.627^^0.652^^1.000**p < 0.001, indicating significance in correlation
Screening of factors influencing innovative behavior of ICU nurses
Ranking of variable importance
In this study, the dependent variable was the ICU nurses’ innovative behaviour scores, and ten statistically significant variables identified in univariate and correlation analyses were selected for inclusion in the random forest model. The results were output using the Random Forest package in RStudio. Increase in Node Purity (IncNodePurity) measures the extent to which a feature (variable) contributes to reducing node ‘impurity’ when splitting nodes in a decision tree. The larger the value of IncNodePurity, the more important the feature is in increasing node purity (i.e., the degree of aggregation of samples of the same category) when splitting the data. The larger the IncNodePurity value, the more critical the feature [47]. The assignment situations of each variable in the random forest model are detailed in Table 4. The results showed that the spiritual climate variable had the highest importance, while the physical health status variable had the lowest importance, as illustrated in Fig. 1.
Table 4. Variable encoding and assignment in the random forest modelVariableCodeVariable AssignmentAgeX1≤ 25 years = 1, 26–30 years = 2, 31–35 years = 3, 36–40 years = 4, ≥ 41 years = 5Education levelX2Junior college or below = 1, Bachelor’s = 2, Master’s or above = 3Professional titleX3Nurse = 1, Senior nurse = 2, Nurse-in-charge = 3, Deputy chief nurse or above = 4Current positionX4Clinical nurse = 1, Head nurse = 2Total years of nursing experience (years)X5<6 years = 1, 6–10 years = 2, 11–15 years = 3, ≥16 years = 4Physical healthX6Good = 1, Fair = 2, Worse = 3The degree of love for nursing workX7Like = 1, More like = 2, Not sure = 3, Don’t like = 4Thriving at WorkX8Original value inputSpiritual ClimateX9Original value inputInformation LiteracyX10Original value input
Fig. 1. Importance ranking of factors influencing innovative behaviors in ICU nurses
Variable selection
Ranking results based on the importance of the variables, Lasso regression analysis was performed in R Studio using the glmnet function on 10 variables identified as statistically significant in the univariate analysis. As shown in Fig. 2, the vertical dashed line on the left represents lambda. min, while the line on the right represents lambda.1se. When the lambda (λ) value was 1.531, the model achieved the minimum error, corresponding to six influencing factors. Consequently, the top six variables—spiritual climate, information literacy, thriving at work, the degree of love for nursing work, educational level, and age—were included in the multivariate stepwise regression analysis.
Fig. 2LASSO regression with cross-validation
Multivariate analysis of influencing factors of innovative behaviors of ICU nurses
Taking the total score of ICU nurses’ innovative behaviors as the dependent variable and combining the results of LASSO regression, the independent variables screened by the random forest model with the top 6 importance were included in the multivariate stepwise linear regression analysis. The results showed that spiritual climate, information literacy, thriving at work, the degree of love for nursing work, educational level, and age were the main influencing factors of ICU nurses’ innovative behaviors (all p < 0.05), which could explain 55.7% of the variance in innovative behaviors. See Table 5.
Table 5. Multiple Stepwise regression results of factors influencing innovative behavior of ICU nurses (n = 587)FactorBSE of BBetatP-valueConstant16.7604.384-3.823<0.001Thriving at work0.1540.0700.1072.1950.029Spiritual climate0.2220.0360.3016.254<0.001Information literacy0.2950.0490.2606.047<0.001Age1.3370.4150.0933.2180.001Educational level7.2841.0270.2027.096<0.001The degree of love for nursing work-2.1730.598-0.130-3.637<0.001B Regression coefficient, SE of B Standard error of B, Beta Standardized beta coefficient, R = 0.750, R^2^ = 0.562, adjusted R^2^ = 0.557, F = 124.035, P < 0.001
Discussion
Intensive care units possess distinct workforce profiles and specialized professional capacities, utilizing advanced technologies to manage critically ill patients. Nurses must be innovative, especially in specialized and complex areas, such as intensive care [48]. The total score of Innovation Behaviour among ICU nurses in this study was (76.43 ± 14.67), with an average score of all items at (3.82 ± 0.73), which is at a moderate to high level compared to the median score of 3.00 on the scale. These scores exceeded those reported by Wang et al. [49]. for psychiatric nurses and Hashemian et al. [50] for clinical nurses, suggesting ICU nurses generally possess substantive innovative capacity. Several factors may explain these findings. First, China’s national innovation-driven development strategy and enhanced healthcare innovation ecosystems have elevated nursing innovation levels, aligning with empirical evidence for online psychological capital interventions and transformational leadership theories in nursing interventions [51, 52]. Second, this study employed the IBI-20 scale, selected for its predictive validity and comprehensive measurement, which differs from the instruments used in prior research. Finally, ICU-specific characteristics (e.g., rapid technological iteration, high-risk clinical environments) necessitate continuous knowledge updating, which may foster greater innovation than in non-acute settings. The findings of study, Zhang, et al. [26] showed that the practical wisdom developed by ICU nurses in the process of coping with the complex conditions of acutely ill patients not only provides empirical evidence for the development of the nursing discipline but also promotes the innovation and optimization of the nursing education model through knowledge translation. Among the five dimensions of the ICU nurses’ Innovative Behavior Scale assessed in this study, the relatively high scores observed in the “Overcoming Obstacles” and “Idea Generation and Search” dimensions can be attributed to the higher educational attainment of the participating ICU nurses. Specifically, 82.8% of the nurses held a bachelor’s degree or higher. An increased level of education has been positively associated with enhanced critical thinking and clinical decision-making abilities, which may encourage nurses to engage in autonomous reasoning and adopt creative strategies when addressing clinical challenges [24]. This cognitive flexibility likely facilitates both the generation of innovative ideas and the capacity to overcome barriers in the pursuit of clinical objectives. Nursing managers should actively encourage ICU nurses to enhance their educational background. Conversely, the lower scores obtained in the “Involving others” dimension may be linked to the heavy workloads commonly experienced by ICU nurses, as well as a perceived lack of organizational support for implementing innovative nursing practices [53]. This discrepancy may be attributed to the influence of transformational leadership [54], due to a lack of effective team cooperation skills, they face difficulties in establishing their own innovative teams; consequently, they often undertake scientific research tasks independently resulting in a lower score for involving others dimension. Previous studies have indicated that organizing team collaboration and allocating tasks efficiently can save time while avoiding disruptions to daily nursing duties and facilitating successful completion of scientific research innovations [55]. Therefore, nursing managers should actively foster an innovative cultural atmosphere, carry out theoretical and practical innovative training teaching based on the ADDIE teaching model [56] and also form a professional nurse innovation service team to investigate and analyze nurses’ innovative ideas, seek available resources for them, assist in formulating implementation plans, and conduct utility evaluations to promote the realization of nurses’ innovative ideas. At the same time, an innovation reward system has been established, with sufficient attention and organizational support given to encourage nurses to take the initiative and continuously promote their learning, practice, and innovation.
The results of this study showed that the Spiritual Climate of the work environment was the most critical factor influencing the innovative behavior of ICU nurses (β = 0.222, P < 0.05). It was able to positively promote innovative behavior, which is consistent with the findings of He et al. [57]. The Conservation of resources Theory, proposed by Hobfoll [58], a positive work environment Spiritual Climate (e.g., teamwork, leadership empowerment, and organizational support) is a core conditioning resource that can lead to ICU nurses not needing to consume additional resources to cope with interpersonal conflict or managerial stress and can devote more energy to innovative behaviors. Previous studies support this notion: a favorable Spiritual Climate directly affects clinical nurses’ work commitment and job satisfaction, which in turn prompts them to be able to devote more time and energy to optimizing the functional framework of the position and the elements of the operational process, etc., and to innovate to enhance the level of innovation continuously [34, 59]. Xie et al. [60] suggested improving the Spiritual Climate of the working environment for nurses by enhancing teamwork. It is suggested that managers encourage ICU nurses to actively express their innovative ideas and spiritual needs, promote trust and effective communication among team members, proactively share innovative knowledge and experiences, facilitate the sharing of tacit knowledge within the team, and stimulate more innovative behaviors among nurses.
The findings of this study revealed that information literacy was the second most influential factor affecting the innovative behavior of ICU nurses (β = 0.295, P < 0.05). Information literacy can positively impact the innovative behavior of ICU nurses, which is consistent with studies by Zhong et al. [61] investigating nursing students and Wang et al. [24] examining specialized nurses. Information literacy, as a core competency for nurses’ lifelong learning and professional development, plays a fundamental role in innovative behaviors, enabling them to accurately retrieve and utilize information, evaluate its credibility and authority, and integrate practical information into their innovative ideas and approaches [61, 62]. Nurses who possess good information literacy skills can not only recognize the value of information but also locate relevant knowledge resources through professional information platforms and apply critical thinking to assess the truth, usefulness, and authenticity of information in various areas. In this mental process, nurses add verified information to their professional knowledge base, use reverse thinking to break down existing problems, and employ forward-looking thinking to explore new ways of doing things. They then realize the innovation of the nursing knowledge base by reassembling information, which leads to new technologies, methods, and ideas that are useful in real-life applications. This suggests that when hospital administrators consider the factors influencing nurses’ innovative behaviors, they can enhance nurses’ innovative behaviors by improving their information literacy. An ongoing education office can be established to systematically develop and implement information literacy training programs tailored to the needs of clinical nurses [63], integrating various forms of learning such as virtual training platforms [64], and scenario simulation [65] to enhance their level of information literacy.
This study reveals that Thriving at Work is the third major factor influencing the innovative behavior of ICU nurses (β = 0.154, P < 0.05), and it can positively promote innovative behavior. Nurses with a high level of Thriving at Work will deepen their understanding of clinical problems through continuous learning, come into contact with new ideas and perspectives, broaden their thinking horizons, and facilitate the identification of problems and the search for solutions, thus enhancing innovative behaviors. This finding is consistent with that of Liu et al. [25], who concluded that nurses with increasing Thriving at Work will experience stronger self-efficacy in carrying out innovative work due to their personal growth, which will encourage them to exhibit more innovative behaviors. The study carried out by Nguyen and McGuirk et al. [66] in Vietnam reported that when the level of Thriving at Work of nurses is high, individuals deepen their understanding of clinical problems through continuous learning, come into contact with more new concepts and perspectives, broaden their horizons of thinking, are better able to identify problems and seek solutions, and their innovative behavior is enhanced. The findings of Bai et al.‘s [67] study in China indicate that focusing on strengths promotes continuous learning and growth, fostering a sense of thriving at work. It is recommended that nursing administrators or leaders pay attention to differences in individual levels of strengths use, encourage strengths-based practices, and design interventions that foster hope, thereby promoting greater thriving in their professional roles [68]. In addition, nursing managers draw on magnetic hospital management strategies to build flexible scheduling systems, reasonable empowerment mechanisms, and hierarchical training systems in the clinical work environment, simultaneously guaranteeing the optimization of the practice environment and the maintenance of organizational fairness, as well as multi-dimensional interventions to improve the level of nurses’ work prosperity and ultimately stimulate their clinical innovation effectiveness.
One major contribution of our study was to find that these demographic characteristics did not uniformly impact innovative behavior, as we linked the selected demographic characteristics to innovative behavior using a random forest. For example, the results of this study show that the demographic characteristic factors influencing the innovative behavior of ICU nurses are, in order, the degree of love for nursing work, educational level, and age. Positive attitudes toward nursing work help promote innovative behavior. This study shows that the degree of love for nursing work is a key factor influencing the innovative behavior of ICU nurses, and the more positive the attitude toward nursing work, the higher the score of innovative behavior (β =-2.173, P < 0.05). According to Masaoud’s study [69], the degree of fondness for nursing work reflects the nurses’ work attitude to a certain extent and also determines the nurses’ efforts. The findings of this study also indicate that educational level is directly related to the level of innovative behavior of ICU nurses participating in this study. In line with this study, Xiang et al. [70] in China and Dayan et al. [48] in Turkey revealed that highly educated nurses may stem from their advantages in systematic knowledge reserves and theory-practice transformation capabilities. They possess stronger abilities in identifying clinical problems and generating innovative thinking, and are more likely to access support resources for innovative practices. Furthermore, the results of this study revealed that age is a significant factor influencing the innovative behavior of ICU nurses (β = 1.337, P < 0.05). Other studies, in line with the findings of this study, have noted that senior nurses possess rich clinical experience and exhibit active, innovative thinking. It is easier to form the output ability of scientific research results driven by the demand for title promotion. In contrast, junior nurses are often faced with insufficient organizational support, time and resource constraints, and environmental constraints due to seniority limitations, which makes it difficult to implement their innovative programs effectively and ultimately leads to a low rate of innovation transformation [71]. This study suggests that nursing managers should prioritize nurses’ career development needs and enhance work motivation by listening to their expressions of work attitudes and understanding their career motivations and goals. This study reveals that only 1.70% of clinical nurses hold a master’s degree, and the lack of continuing education may hinder the development of their innovative abilities. It is recommended that a tiered training system be constructed based on the differences in nurses’ seniority and competence levels, that innovative courses be designed to match their positions, and that an innovative mentorship system be developed for highly educated and senior nurses to provide sustainable support for the innovative practice of nursing teams.
Limitations
This study has several limitations that need to be considered. First, the questionnaire utilized for this survey was self-reported by ICU nurses, potentially resulting in findings that are somewhat inflated compared to the actual levels. To mitigate this bias, subsequent researchers may employ evaluations conducted by others or utilize interviews. Second, this is a cross-sectional survey, which may limit the ability to infer causal relationships. Future longitudinal studies may investigate the long-term effects and causal relationships among these variables. Third, the relational paradigm in this research requires validation across diverse demographics and urban areas. Finally, this study employed a restricted set of fundamental personal and professional characteristics as independent variables, potentially overlooking significant elements such as methods of continuing education. Future studies should meticulously investigate the aspects related to continued education.
Conclusion
This multicentre cross-sectional study, utilizing a random forest model combined with multivariate stepwise linear regression, identified and ranked key factors influencing innovative behaviours among ICU nurses in China. Our findings demonstrate that ICU nurses exhibit moderately high levels of innovative behaviour. Spiritual Climate, Information Literacy, and Thriving at Work emerged as significant positive predictors. The degree of love for nursing work, education level, and age were also identified as influential factors, ranked according to their relative importance by the random forest algorithm. These results provide crucial insights for nurse managers and healthcare leaders. Specifically, developing targeted interventions to enhance spiritual climate, foster information literacy, and promote thriving at work offers a strategic pathway to support and amplify innovative practices among ICU nurses within the healthcare context.
Practical implications of the study
This research is the first to use a random forest model to analyse factors associated with ICU nurses’ innovative behaviours, offering a fresh perspective compared with linear or logistic regression studies. The findings of this study have significant practical implications in several aspects: Firstly, the innovative behaviour of Chinese ICU nurses is at a moderate to high level. Nursing managers should recognize that enhancing innovative behaviour has crucial implications for nursing quality and industry development. Organizations should formulate innovation-centric policies to motivate nursing leaders to support innovation and foster an environment that promotes new practices [72]. Secondly, nursing managers should promote the information literacy of ICU nurses to enable them to effectively acquire, evaluate, and utilize information, thereby establishing a strong foundation for nursing innovation. Nursing administrators can expand nurses’ innovative information acquisition and access by carrying out professional courses such as resource and interactive exchange platforms, scientific research lectures, and literature searches, establish a scientific information literacy cultivation system for nurses, and cultivate their critical and dialectical thinking, and promote their innovative behaviors in the process [73]. Thirdly, nursing managers pay attention to nurses’ work emotions, monitor their work status, and timely understand and defuse negative work emotions. This helps build a spiritually friendly, comfortable, and safe work culture atmosphere, stimulates nurses’ work enthusiasm and initiative, and ultimately improves work performance and innovation levels. Finally, leaders should prioritize shaping an empowering work environment to enhance the innovation efficiency of nursing work. For example, establishing a fair and equitable system and evaluation process, building a feedback environment, and providing mental health resources, as well as more opportunities for career development, are ways to enhance nurses’ Thriving at Work [74], which in turn promotes innovative behaviors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Nurses Association. ANA Enterprise 2023–2025 Strategic Plan.2023. https://www.nursingworld.org/globalassets/ana-enterprise/about-us/ana-strategic-plan-2024.pdf
- 2Duan X, Shen T, Xu W, Wu A, Xie H. Examining the mediating role of role identity and knowledge sharing in the association between leadership support and nurses’ innovative behaviour: a multicentre cross-sectional study. J Adv Nurs. 2025;1–13.10.1111/jan.1703840349116 · doi ↗ · pubmed ↗
- 3Norman G, Monteiro S, Salama S. Sample size calculations: should the emperor’s clothes be off the Peg or made to measure? BMJ. 2012;345.10.1136/bmj.e 527822918496 · doi ↗ · pubmed ↗