Clinical efficacy of sitafloxacin-containing regimens for Mycobacterium avium complex pulmonary disease
Naohisa Urabe, Susumu Sakamoto, Nozomi Tokita, Takumi Kanokogi, Rio Tsunehara, Kazuma Kishi

TL;DR
This study evaluates the effectiveness of sitafloxacin in treating Mycobacterium avium complex pulmonary disease, finding limited clinical improvement in most patients.
Contribution
The study provides new clinical data on the efficacy of sitafloxacin-containing regimens for MAC pulmonary disease.
Findings
Fewer than 20% of patients showed radiologic, symptomatic, or microbiological improvement.
Only two patients achieved sputum culture conversion, both with clarithromycin-susceptible strains.
Sitafloxacin may serve as an adjunct when standard therapies are not feasible, but its overall role is limited.
Abstract
Fluoroquinolones (FQ) have shown efficacy against Mycobacterium avium complex (MAC) across experimental settings, in vitro and in vivo. Sitafloxacin (STFX) has demonstrated particularly strong anti-MAC activity, but clinical data on its effectiveness in treating MAC pulmonary disease (MAC-PD) are sparse. This study aimed to evaluate the efficacy of STFX-containing regimens in patients with MAC-PD. This retrospective cohort study included 50 patients with MAC-PD who received STFX-containing regimens for ≥6 months at a single center between January 2015 and March 2024. Patients were categorized into four groups: Group 1, STFX-treated without surgery (n = 49); Group 2, STFX started ≥6 months after guideline-based treatment (GBT) began (n = 40); Group 3, poor radiologic response to GBT (n = 38); and Group 4, persistent positive sputum cultures at STFX initiation (n = 19). Primary outcomes…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
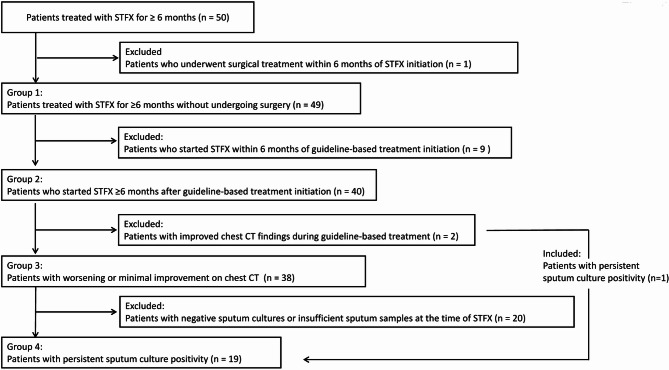 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Tuberculosis Research and Epidemiology · Neutropenia and Cancer Infections
Background
The incidence of pulmonary disease caused by nontuberculous mycobacteria (NTM) has been increasing globally [1]. Mycobacterium avium complex (MAC) is the most common causative agent of NTM lung disease in Japan [2]. Guideline-based treatment (GBT) for MAC pulmonary disease (MAC-PD)—consisting of a macrolide (clarithromycin [CLA] or azithromycin [AZM]), ethambutol (EB), and rifampin (RFP)—was first recommended in the 1997 American Thoracic Society (ATS) guidelines [3]. The 2020 ATS/European Respiratory Society/European Society of Clinical Microbiology/Infectious Disease Society of America (ATS/ERS/ESCMID/IDSA) guidelines still endorse this three-drug regimen as standard therapy [4]. Despite long-standing clinical use, GBT yields a treatment success rate of only approximately 60% [5], and patients who fail to achieve sputum culture conversion after six months of GBT are considered to have refractory MAC-PD. For these patients, the addition of aminoglycosides is recommended, of which amikacin liposome inhalation suspension (ALIS) has the strongest supporting clinical evidence. Its treatment success rate, however, is around only 30% [6, 7]. This underscores the urgent need for viable alternative therapeutic options for this difficult-to-treat condition.
Fluoroquinolones (FQ) have demonstrated in vitro and in vivo activity against MAC pathogens [8, 9], and certain agents in this class have shown promise as components of initial treatment regimens [10, 11]. Notably, sitafloxacin (STFX) has been reported to exhibit more potent anti-MAC activity than other FQ [9]. Nevertheless, the clinical utility of STFX in the treatment of MAC-PD remains unclear, and the 2020 guidelines do not include STFX as a recommended treatment option. Therefore, the objective of this study was to evaluate the clinical efficacy of STFX-containing regimens in patients with MAC-PD.
Methods
Study population
This single-center retrospective cohort study included 50 patients diagnosed with MAC-PD who received antimicrobial therapy regimens inclusive of STFX for at least six consecutive months at Toho University Omori Medical Center between January 2015 and March 2024. All patients satisfied the ATS/ERS/ESCMID/IDSA guidelines diagnostic criteria for MAC-PD [4]. The cohort included both newly diagnosed and previously treated (recurrent) cases: 39 newly diagnosed and 11 recurrent after prior treatment. Patients who had co-infection with non-MAC NTM or other fungi were excluded.
Study design
We retrospectively reviewed the clinical indications for initiating STFX, the timing of initiation, and the duration of treatment. Based on the timing and indication for STFX initiation, patients were classified into four groups (Fig. 1). Group 1: Patients who received STFX for ≥ 6 months without undergoing surgical resection. Group 2: Patients for whom STFX was initiated ≥ 6 months after the start of GBT. Group 3: Patients with worsening or no improvement in chest CT findings while receiving GBT. Group 4: Patients with persistently positive sputum cultures at the time of STFX initiation. For each group, treatment outcomes were assessed at six months after STFX initiation, including sputum culture conversion, radiologic improvement on chest computed tomography (CT), and improvement in patient-reported symptoms.Fig. 1. Flowchart of patient selection and classification into four groups based on clinical criteria. STFX: sitafloxacin
In addition, within Group 1, we analyzed the characteristics of patients who demonstrated radiologic improvement on chest CT following an STFX-containing regimen. Factors associated with radiologic improvement were evaluated using univariate logistic regression analyses. We also assessed the characteristics of patients who achieved sputum culture conversion. In Group 4, serial changes in sputum culture results were evaluated to assess microbiological response over time.
Definitions
Sputum specimen collection was frequently incomplete in this retrospective cohort; therefore, the conventional definition of culture conversion (three consecutive negative cultures) could not be applied in many cases. As shown in Table 8, only 6 of 19 patients had ≥ 3 sputum specimens obtained between 6 and 12 months after STFX initiation. Therefore, culture conversion was defined as ≥ 2 consecutive negative cultures obtained ≥ 4 weeks apart. Radiologic improvement was assessed using the NICE (Nodule, Infiltration, Cavity, Ectasis) scoring system [12], with a decrease in score indicating improvement. Subjective symptom improvement was evaluated using the COPD Assessment Test (CAT) score [13]; a reduction of ≥ 3 points, corresponding to the minimal clinically important difference (MCID) as defined in previous studies on bronchiectasis, was considered clinically meaningful improvement [14]. Based on the Clinical and Laboratory Standards Institute (CLSI) M24A standard, clarithromycin (CLA) resistance was defined as a minimum inhibitory concentration (MIC) ≥ 32 µg/mL [15].
Data collection
We collected data on patient age, sex, body mass index (BMI), smoking history, comorbidities, concomitant medications, chest CT findings, sputum culture results, drug susceptibility testing of MAC isolates, indications for initiating STFX or reasons for discontinuing, and CAT scores. At our institution, all patients with MAC-PD—including those treated with STFX—routinely undergo chest CT scans and CAT score assessments approximately six months after treatment initiation to assess therapeutic response. The data used in this study were retrospectively collected from these evaluations, which were performed as part of standard clinical care. Baseline chest CT scans were performed within 3 months prior to STFX initiation, and follow-up CT scans used to assess treatment response were obtained between five and seven months after starting STFX. All relevant data are summarized in Supplementary Table 1.
Statistical analysis
Data are presented as number of patients (percentage), and age is expressed as median with interquartile range. Associations between categorical and continuous variables across the two groups were tested using the Chi-squared or Fisher’s exact test, and the Mann–Whitney U test, respectively. Factors independently associated with radiologic improvement were evaluated using univariate logistic regression analyses. A p-value of < 0.05 was considered indicative of statistical significance. Statistical analyses were performed using SPSS software version 25 (IBM Corp., Armonk, NY).
Results
Patient characteristics
A total of 50 patients with MAC-PD were treated with STFX-containing regimens for ≥ 6 months. As summarized in Table 1, the median age was 68 years, and 82% were female. Radiologic patterns included non-cavitary nodular bronchiectasis (NBE) in 56%, cavitary NBE in 32%, and fibro-cavitary (FC) type in 12%. Clarithromycin resistance was identified in 14% (6/43) of isolates tested. Table 2 presents the primary indications for initiating STFX. These include worsening chest CT findings (56%) and lack of radiologic improvement (22%), persistent sputum culture positivity (40%), with some patients meeting multiple criteria. Additional reasons included the need for initial intensive therapy (4%) and discontinuation of EB (12%) or rifampin (RFP) (6%) due to intolerance. STFX was started as part of the initial regimen in 14%, and after ≥ 6 months of GBT in 82% (median, 14.7 months). At the time of data cutoff, 44% of patients remained on treatment. Among those who had discontinued therapy, the median treatment duration was 12.2 months. As shown in Table 3, most patients received either a three-drug (54%) or a two-drug (40%) regimen. All regimens included a macrolide; the commonly used concomitant medications were EB (88%) and RFP (70%).Table 1. Clinical characteristics of patients treated with sitafloxacinCharacteristicNo. of patients (n = 50)Age, years; median (range)^a^68 (61.3–75)Sex, female; n (%)41 (82)BMI (kg/m^2^); median (range)^a^18.3 (16.5–19.6)Smoking, never; n (%)35 (70)Comorbidities; n (%)Rheumatoid arthritis5 (10)Sinusitis3 (6)Malignancy1 (2)Underlying pulmonary disease; n (%)Emphysema3 (6)Interstitial pneumonia3 (6)Concomitant drug; n (%)Corticosteroids3 (6)Immunosuppressant2 (4)Biopharmaceutical2 (4)Infective MAC isolate; n (%)M. avium41 (82)M. intracellulare9 (18)Subjective symptoms (range)^a^CAT score11 (6–18)Cough score^b^2 (1–3)Sputum score^b^1 (0–3)Radiographic pattern; n (%)Non-cavitary NBE type28 (56)FC type6 (12)Cavitary NBE type16 (32)Total chest CT score; median (range)^a^9 (7–12)Cavitary lesion; n (%)22 (44)Proportion of resistant strains; n (%)Clarithromycin6/43 (14)BMI, Body Mass Index; MAC, Mycobacterium avium complex;CAT COPD assessment test, CT Computed tomography, NBE nodular bronchiectatic,* FC* fibrocavitarya, interquartile range; b, Score for subjective symptoms of cough and sputum, included in CAT score.Table 2. Reasons for sitafloxacin introduction and timing of initiationCharacteristicNo. of patients (n = 50)Reason for STFX introduction; n (%)Persistent sputum culture positivity20*(40)Worsening chest CT findings28 (56)Lack of improvement on chest CT11 (22)Severe disease (initial concomitant use)2 (4)EB discontinuation6 (12)RFP discontinuation3 (6)Timing of STFX introduction; n (%)Initial concomitant use7 (14)Within 6 months of GBT initiation2 (4)After 6 months of GBT initiation41 (82)GBT initiation to STFX introduction interval; months, median (range)14.7 (6.1–28.1)STFX Treatment DurationOngoing as of January 31, 2024; n (%)22 (44)Median duration in discontinued cases, months (range)12.2 (6.8–19.1)Reasons for STFX discontinuationTreatment completion (all medications)10 (20)Treatment failure9 (18)Adverse events6 (12)Patient request1 (2)Death2 (4)STFX sitafloxacin, EB ethambutol, RFP rifampicin, GBT guideline-based treatment*Of the 20 patients, 16 also met the criterion of worsening chest CT findings, 3 overlapped with lack of improvement on chest CT, and 1 had concurrent difficulty with ethambutol use.Table 3. Baseline treatment at sitafloxacin initiationCharacteristicNo. of patients (n = 50)Number of GBT drugs in regimen (at baseline)2/3/420/27/3Baseline drugs (generic name)Clarithromycin34Azithromycin16Ethambutol44Rifampin35Streptomycin2Amikacin2GBT, guideline-based treatment
Assessment of treatment efficacy by group
Treatment outcomes for each group are summarized in Table 4. In Group 1, radiologic improvement was observed in 18.4% (9/49) of patients, subjective symptom improvement in 19.1% (9/47), and sputum culture conversion in 20% (4/20). The corresponding proportions in Group 2 were 12.5% (5/40), 20% (8/40), and 12.5% (2/16), respectively; in Group 3, 13.2% (5/38), 18.4% (7/38), and 13.3% (2/15); and in Group 4, 5.3% (1/19), 15.8% (3/19), and 12.5% (2/16), respectively.Table 4. Evaluation of treatment efficacy across clinical subgroupsCharacteristicGroup 1Group 2Group 3Group 4No. of patients49403819Age, years; median (range)^a^68 (61–75)67.5 (57.8–74.3)67.5 (58.8–74.8)68 (59.5–74.5)Sex, female; n (%)40 (81.6)35 (87.5)33 (86.8)14 (73.7)BMI (kg/m^2^); median (range)^a^18.3 (16.4–19.6)18.3 (16.6–19.6)18.3 (16.5–19.6)18.7 (16.6–19.7)Radiographic pattern; n (%)Non-cavitary NBE type28 (57.1)25 (62.5)23 (60.5)8 (42.1)FC type6 (12.2)4 (10)4 (10.5)4 (21.1)Cavitary NBE type15 (30.6)11 (27.5)11 (28.9)7 (36.8)Sputum Culture Analysis; n (%)Positive culture prior to STFX initiation24 (49%)19 (47.5%)18 (47.4%)19 (100%)Culture conversion at 6–12 months post-STFX4/20 (20%)2/16 (12.5%)2/15 (13.3%)2/16 (12.5%)Chest CT Assessment; median (range)^a^Baseline chest CT score before STFX initiation9 (7–12)9 (7.8–12)9 (8–12)9 (7.5–12)Chest CT score at 5–7 months post-STFX9 (6–12)9 (7.5–12)9 (8–12)9 (8.5–12.5)Patients with improved chest CT scores; n (%)9/49 (18.4%)5/40 (12.5%)5/38 (13.2%)1/19 (5.3%)CAT score; median (range)^a^Baseline CAT score before STFX initiation11 (6–18)11 (6–18)11 (6.3–18)11 (6–19.5)CAT score at 5–7 months post-STFX12 (5.5–17.5)13.5 (6.8–17.3)14.5 (7–17.8)16 (8.5–17.5)Patients with improved CAT scores; n (%)9/47 (19.1%)8/40 (20%)7/38 (18.4%)3/19 (15.8%)BMI Body Mass Index, NBE nodular bronchiectatic, FC fibrocavitary, STFX Sitafloxacin, CT Computed tomographyCAT COPD assessment testa, interquartile range
Table 5 presents the characteristics of patients in Group 1 with improved chest CT findings. A significantly higher proportion of these patients had received STFX within six months of starting GBT (44.4% vs. 12.5%; p = 0.046). On univariable analysis, early administration of STFX (within six months) was associated with radiologic improvement (odds ratio [OR], 5.6; 95% confidence interval [CI], 1.114–28.143; p = 0.036; Table 6). However, among the nine patients who received early STFX, seven had it introduced as part of their initial treatment regimen. Therefore, the observed association may partly reflect the effect of initial therapy rather than salvage treatment, hence the potential for confounding must be considered.Table 5. Characteristics of group 1 patients with improved chest CT findingsCharacteristicImprovement on chest CTNo improvementp valueNo. of patients940Age, years; median (range)^a^76 (67–77)67.5 (57.8–73.3)0.085Sex, female; n (%)7 (77.8)33 (82.5)0.663BMI (kg/m^2^); median (range)^a^18.3 (16.2–18.7)18.3 (16.6–19.6)0.992Absence of cavitary lesions; n (%)5 (55.6)23 (57.5)1.000Early STFX Introduction*; n (%)4 (44.4)5 (12.5)0.046EB co-administration; n (%)8 (88.9)35 (87.5)1.000CLA-susceptible strain; n (%)7/7 (100)30/35 (85.7)0.569M. avium, n (%)8 (88.9)32 (80)1.000STFX initiation with negative sputum culture**; n (%)6 (66.7)19 (47.5)0.463STFX-induced culture conversion at 6–12 months***; n (%)1/3 (33.3)3/17 (17.6)BMI Body Mass Index, STFX sitafloxacin, EB ethambutol, CLA clarithromycin, M. avium Mycobacterium aviumIntroduction of sitafloxacin within six months of guideline-based treatment initiationPatients with negative sputum culture at the time of STFX initiationPatients who achieved sputum culture conversion 6–12 months after STFX initiationTable 6Univariate logistic regression analyses of factors associated with improved chest CT findings in group 1Univariate logistic regressionVariableOR95%CIp-valueAge, years1.0620.982–1.1480.13Sex, female0.7420.126–4.3610.742BMI (kg/m^2^)1.0020.737–1.3600.992Early STFX initiation*5.61.114–28.1430.036EB co-administration1.1430.117–11.1770.909Absence of cavitary lesions0.9240.215–3.9650.915Negative sputum culture2.2110.484–10.0920.306M. avium0.500.054–4.5970.54BMI Body Mass Index, STFX sitafloxacin, EB ethambutol, M. avium,* Mycobacterium aviumIntroduction of sitafloxacin within six months of guideline-based treatment initiation
Table 7 presents the characteristics of Group 1 patients who achieved sputum culture conversion; however, no variables were significantly associated with this outcome.Table 7. Characteristics of group 1 patients with sputum culture conversionCharacteristicCulture conversionNo conversionp-valueNo. of patients416Age, years; median (range)^a^74.5 (68.3–80.3)66.5 (72.8–57.8)0.219Sex, female; n (%)2 (50)12 (75)0.549BMI (kg/m^2^); median (range)^a^18.6 (17.5–18.9)18.8 (16.6–20.4)0.748Absence of cavitary lesions; n (%)3 (75)4 (25)0.101Early STFX Introduction; n (%)2 (50)2 (12.5)0.162EB co-administration; n (%)3 (75)14 (87.5)0.509CLA-susceptible strain; n (%)4 (100)13 (81.3)1.000M. avium, n (%)3 (75)11 (68.8)1.000BMI Body Mass Index, STFX sitafloxacin, EB ethambutol, CLA clarithromycin; M. avium,* Mycobacterium avium.*
Table 8 summarizes the clinical, radiologic, and microbiological data of patients in Group 4 with MAC-PD following STFX treatment initiation. Among the two patients (#2,#12) who achieved sputum culture conversion, both had CLA-susceptible strains at baseline, received EB, and exhibited non-cavitary disease.Table 8. Changes in sputum culture results and drug susceptibility among patients in group 4Case numberSputum culture conversionSexAge, yearsSputum examination results by TimelineBaseline MIC [CLA] (µg/mL)Baseline MIC [LVFX] (µg/mL)6–12 months post-MIC [CLA] (µg/mL)6–12 months post-MIC [LVFX] (µg/mL)Drugs at STFX initiationRadiologic pattern6 months pre-STFX (Baseline)6–12 months post-STFX initiationCountCulturePCRSmearCountCulturePCRSmear1−F8642443133> 160.5> 328C, E, RFC type2་F70310030000.252C, E, RNon-cavitary NBE type3−F7121105100160.540.5C, ENon-cavitary NBE type4−F5232232110> 320.5> 328C, E, ACavitary NBE type5M742111100024Z, E, RCavitary NBE type6−F56412021200.12510.252C, E, RCavitary NBE type7−F822111544311> 3216C, EFC type8−F68110011110.1250.50.1251C, RNon-cavitary NBE type9−M52211022220.25424C, EFC type10−F573100211116181C, E, RCavitary NBE type11−M5821222221> 324> 324C, E, RCavitary NBE type12་F63222020000.54C, E, RNon-cavitary NBE type13−F6621102100140.52C, E, RNon-cavitary NBE type14−M62111122221214C, E, R, SCavitary NBE type15−F79311141100.0610.54C, E, RFC type16−F6133332222> 321> 322C, E, R, ACavitary NBE type17−F75323233330.50.50.50.5C, E, RNon-cavitary NBE type18F702111100012C, E, RNon-cavitary NBE type19M803110100020.25 (STFX)Z, E, RNon-cavitary NBE typeM male, F female, MIC minimum inhibitory concentration, CLA clarithromycin, LVFX Levofloxacin, STFX sitafloxacin, C clarithromycin, E ethambutol, R rifampicin, S streptomycin, A amikacin, Z azithromycin, NBE nodular bronchiectatic, FC fibrocavitary*All MICs were measured using BrothMIC NTM, except this value, which was obtained using BrothMIC SGM.
Discussion
This study evaluated the therapeutic impact of STFX-containing regimens administered for ≥ 6 months in patients with MAC-PD. Across all clinical subgroups, rates of sputum culture conversion, radiologic improvement, and symptom relief consistently remained below 20%, indicating limited overall efficacy.
In contrast, two previous studies documented more favorable outcomes with STFX. Fujita et al. reported culture conversion, radiologic improvement, and symptom relief rates of 44.4%, 55.8%, and 70%, respectively, in 18 patients treated for at least 4 weeks [16]. Similarly, Asakura et al. observed corresponding rates of 23%, 19%, and 26% in patients with refractory MAC-PD [17]. However, both studies employed shorter treatment durations (≥ 4 weeks) compared to this study (≥ 6 months), which may have led to an overestimation of the clinical effectiveness of STFX.
Key differences in patient characteristics among the studies by Fujita et al., Asakura et al., and this study were as follows: CLA resistance rates (not reported/48%/14%), proportion of cavitary lesions (55.6%/42%/44%), median BMI (18.7/18.1/18.3), EB co-administration rates (44.4%/71%/88%), median time from GBT initiation to STFX addition (not reported/60 months/14.7 months), and persistent sputum culture positivity at STFX initiation (100%/100%/40%). Based on these comparisons, our cohort appeared to have a more favorable baseline profile for treatment success: the proportion of CLA-susceptible isolates was higher, EB co-administration was more frequent, and STFX was introduced earlier relative to GBT initiation. Additionally, the proportion of patients with cavitary lesions and the median BMI were generally comparable across studies. It should also be noted that our study applied a less stringent definition of sputum culture conversion—two consecutive negative cultures at least four weeks apart—whereas previous studies used the conventional criterion of three consecutive negative cultures [18]. Despite favorable clinical characteristics and a more lenient methodologically different definition of culture conversion, treatment success rates in our cohort were lower than those previously reported. Although small sample sizes may have contributed to variability in outcomes, the underlying reasons for this discrepancy remain unclear.
Group 4, comprising patients with refractory MAC-PD and persistent sputum culture positivity, demonstrated a sputum culture conversion rate of only 12.5% (2/16) using the definition of two consecutive negative cultures. In contrast, ALIS has shown greater efficacy in refractory MAC PD. The CONVERT trial reported a 6-month culture conversion rate of 29% [6], and real-world data from Japan demonstrated rates of 58.3% [19] and 56.8% [20]. In addition, culture conversion was 8.9% (10/112) in the CONVERT GBT-alone arm under a three-negative criterion [6], compared with 12.5% (2/16) in our refractory subgroup treated with GBT plus STFX using the two-negative criterion. Although cross-trial comparisons should be interpreted with caution, these findings suggest that adding STFX to GBT confers, at best, limited incremental benefit. Compared to these outcomes, STFX appears less effective and is unlikely to be suitable as a first-line agent in the treatment of refractory MAC-PD. Its use may be limited to patients in whom aminoglycosides are contraindicated or poorly tolerated.
In this study, early initiation of STFX, defined as within 6 months of GBT initiation, was the only factor independently associated with radiologic improvement in Group 1. However, in most cases of these cases STFX was introduced as part of the initial treatment regimen. Thus, the observed benefit may be partially attributable to the effects of initial therapy rather than STFX alone. In Group 2, which excluded patients who received early STFX initiation and included those with more refractory disease, no significant predictors of radiologic improvement were identified (data not shown). These findings suggest that while early introduction of STFX may offer some clinical benefit, this should be interpreted with caution, due to potential confounding factors. Notably, previous studies have also reported an association between improved outcomes and the early use of FQ-containing regimens. For example, a gatifloxacin-containing regimen achieved a culture conversion rate of 84.6% [10], and a randomized trial comparing RFP/EB/CAM with RFP/EB/ciprofloxacin demonstrated comparable cure rates [11]. However, other studies have reported that early addition FQs to GBT did not significantly improve culture conversion rates [21], underscoring the uncertainty regarding their clinical benefit.
Recent studies have cautioned that substituting EB with FQs may reduce treatment efficacy [22, 23] and increase the risk of CLA resistance when EB is omitted from macrolide–FQ regimens [24]. These findings highlight the importance of maintaining EB co-administration when using FQ-based therapies, including STFX. In our study, previously recognized negative prognostic indicators—such as absence of EB co-administration, cavitary disease [25], CLA resistance [24], and M. intracellulare infection [26]—were not significantly associated with treatment response. However, among Group 4 patients with persistent sputum culture positivity, the two individuals who achieved culture conversion shared three favorable features: CLA-susceptible isolates, EB co-administration, and non-cavitary disease. These observations suggest that STFX may be most effective in a distinct subgroup of patients who exhibit this triad of clinical factors.
This study has several limitations. First, this was a retrospective single-center study with a limited sample size, which may affect the generalizability of the findings. Second, the standard definition for sputum culture conversion could not be fully applied because sputum sampling was insufficient in some cases. Third, minimum inhibitory concentration (MIC) data for STFX were unavailable, as susceptibility testing at our institution during the study was conducted using the BrothMIC NTM^®^ Far East system, which does not include STFX. Fourth, in Group 1, only nine cases showed radiologic response at six months. This small number of events per variable limited the feasibility of multivariable modeling, therefore, univariable associations, as reported here, should be regarded as primarily exploratory and potentially confounded. Fifth, the safety of STFX could not be comprehensively assessed because only patients who continued treatment for ≥ 6 months were included, and adverse events not resulting in discontinuation were not recorded systematically. Finally, comparative analysis between EB-intolerant and RFP-intolerant patients was not feasible due to the limited number of cases and the clinical similarity between these groups (Supplementary Table 2).
Conclusions
STFX-containing regimens demonstrated limited efficacy in patients with MAC-PD, with response rates below 20%. Early introduction of STFX may offer some clinical benefit, however, its overall impact remains uncertain. STFX should thus be considered only when standard treatment options are not feasible.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.