Patient conversations that matter: assessing the role of TARGET TYI leaflets for respiratory care in England’s community pharmacies
Sejal Parekh, Lingqian Xu, Kieran Hand, Diane Ashiru-Oredope, Donna M Lecky

TL;DR
This study shows that using TARGET TYI leaflets in community pharmacies helped manage respiratory infections better, reduced the need for escalation, and supported patient self-care.
Contribution
The study demonstrates the effectiveness of incentivizing the use of TYI leaflets in community pharmacies to improve antibiotic stewardship and patient care.
Findings
The proportion of patients needing escalation to a pharmacist dropped from 23% to 15% after using the leaflets.
Over 80% of patients accepted over-the-counter remedies, and nearly all received self-care advice.
Incentivization led to widespread adoption of the leaflets by pharmacies, improving healthcare efficiency.
Abstract
The TARGET Treating Your Infection (TYI-RTI) leaflets are designed to support healthcare professionals in delivering tailored conversations with patients about respiratory tract infection (RTI) symptoms. This study evaluated their use across community pharmacies in England through the Pharmacy Quality Scheme (PQS). In 2022–23 and 2023–24, the PQS incentivized community pharmacies to use TYI-RTI leaflets for patients presenting with upper RTIs during a 4 week period each year. Across the 2 years, 225 615 patients were reviewed using TYI-RTI leaflets. A total of 7525 pharmacies participated in at least 1 year, with 7407 taking part in both. The proportion of patients requiring escalation to the pharmacist fell from 23% (26 678) in 2022–23 to 15% (16 417) in 2023–24. Approximately one-third of patients were managed entirely by the wider pharmacy team. Signposting to another healthcare…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
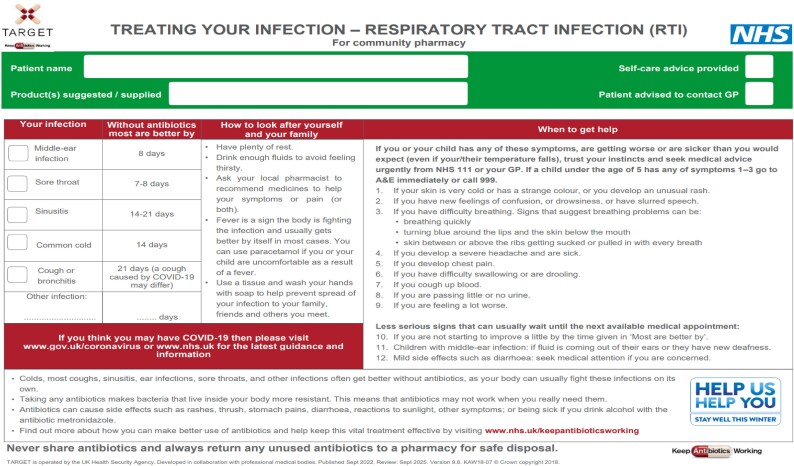 Figure 1
Figure 1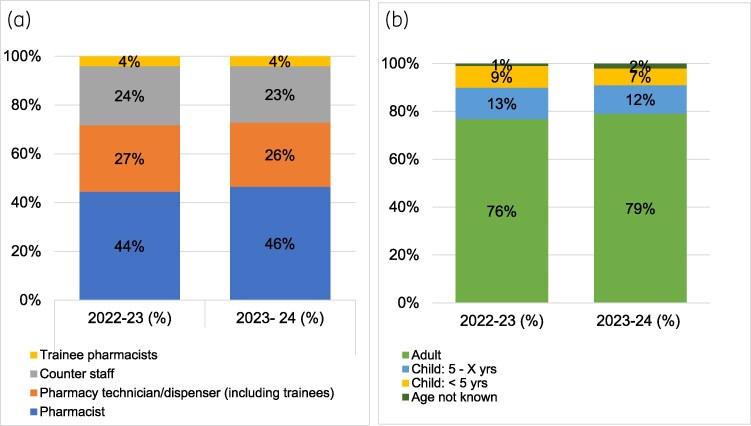 Figure 2
Figure 2| Suspected infections | Number of patients | Number of patients |
|---|---|---|
| Cough or bronchitis | 45 822 (33) | 38 848 (31) |
| Sore throat | 34 220 (25) | 31 099 (25) |
| Common cold | 29 802 (22) | 28 627 (23) |
| Sinusitis | 14 538 (10.5) | 15 331 (12) |
| Middle ear infection | 9596 (7) | 9012 (7) |
| COVID-19 | 1587 (1) | 1531 (1) |
| Other | 2091 (1.5) | 1453 (1) |
| Total number of suspected infections | 137 656 (100) | 125 901 (100) |
| Total number of patients | 115 094 | 110 521 |
| 2022–23 | 2023–24 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Condition | Escalation within the pharmacy | Under 5 years (%) | Over 5 years (%) | Adult (%) | Age unknown (%) | Total (%) | Escalation within the pharmacy | Under 5 years (%) | Over 5 years (%) | Adult (%) | Age unknown (%) | Total (%) |
| Cough or bronchitis | No—escalation was not needed | 1142 (1) | 2115 (2) | 15 998 (14) | 217 (0) | 19 489 (17) | No—escalation was not needed | 771 (1) | 1724 (2) | 13 193 (12) | 280 (0) | 15 982 (14) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 1727 (2) | 1785 (2) | 12 025 (10) | 113 (0) | 15 663 (14) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 1535 (1) | 1902 (2) | 13 382 (12) | 60 (0) | 16 894 (15) | |
| Yes | 1522 (1) | 1620 (1) | 7466 (6) | 92 (0) | 10 709 (9) | Yes | 771 (1) | 955 (1) | 4104 (4) | 171 (0) | 6006 (5) | |
| Total | 4391 (4) | 5520 (5) | 35 489 (31) | 422 (0) | 45 861 (40) | Total | 3077 (3) | 4581 (4) | 30 679 (28) | 511 (0) | 38 883 (35) | |
| Sore throat | No—escalation was not needed | 508 (0) | 1809 (2) | 12 547 (11) | 257 (0) | 15 134 (13) | No—escalation was not needed | 248 (0) | 1177 (1) | 10 546 (10) | 316 (0) | 12 298 (11) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 1028 (1) | 1845 (2) | 8577 (7) | 109 (0) | 11 569 (10) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 677 (1) | 2229 (2) | 11 778 (11) | 157 (0) | 14 854 (13) | |
| Yes | 908 (1) | 1698 (1) | 4855 (4) | 79 (0) | 7546 (7) | Yes | 325 (0) | 908 (1) | 2686 (2) | 52 (0) | 3975 (4) | |
| Total | 2444 (2) | 5352 (5) | 25 979 (23) | 445 (0) | 34 249 (30) | Total | 1250 (1) | 4314 (4) | 25 010 (23) | 525 (0) | 31 127 (28) | |
| Common cold | No—escalation was not needed | 1047 (1) | 1984 (2) | 12 041 (10) | 218 (0) | 15 303 (13) | No—escalation was not needed | 721 (1) | 1569 (1) | 10 641 (10) | 271 (0) | 13 214 (12) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 1292 (1) | 1321 (1) | 6108 (5) | 74 (0) | 8803 (8) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 1387 (1) | 1712 (2) | 8730 (8) | 142 (0) | 11 982 (11) | |
| Yes | 1127 (1) | 1210 (1) | 3324 (3) | 56 (0) | 5722 (5) | Yes | 580 (1) | 740 (1) | 2095 (2) | 39 (0) | 3457 (3) | |
| Total | 3466 (3) | 4515 (4) | 21 473 (19) | 348 (0) | 29 828 (26) | Total | 2688 (2) | 4021 (4) | 21 466 (19) | 452 (0) | 28 652 (26) | |
| Sinusitis | No—escalation was not needed | 74 (0) | 184 (0) | 5446 (5) | 85 (0) | 5794 (5) | No—escalation was not needed | 44 (0) | 119 (0) | 4870 (4) | 123 (0) | 5161 (5) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 127 (0) | 191 (0) | 4679 (4) | 51 (0) | 5052 (4) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 114 (0) | 265 (0) | 7131 (6) | 78 (0) | 7595 (7) | |
| Yes | 116 (0) | 182 (0) | 3355 (3) | 48 (0) | 3704 (3) | Yes | 77 (0) | 109 (0) | 2360 (2) | 41 (0) | 2589 (2) | |
| Total | 317 (0) | 557 (0) | 13 480 (12) | 184 (0) | 14 550 (13) | Total | 235 (0) | 493 (0) | 14 361 (13) | 242 (0) | 15 345 (14) | |
| Middle ear infection | No—escalation was not needed | 190 (0) | 289 (0) | 1268 (1) | 34 (0) | 1783 (2) | No—escalation was not needed | 97 (0) | 147 (0) | 882 (1) | 30 (0) | 1157 (1) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 699 (1) | 746 (1) | 2307 (2) | 36 (0) | 3791 (3) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 1035 (1) | 1220 (1) | 2892 (3) | 78 (0) | 5230 (5) | |
| Yes | 758 (1) | 865 (1) | 2352 (2) | 52 (0) | 4030 (4) | Yes | 463 (0) | 603 (1) | 1519 (1) | 46 (0) | 2633 (2) | |
| Total | 1647 (1) | 1900 (2) | 5927 (5) | 122 (0) | 9604 (8) | Total | 1595 (1) | 1970 (2) | 5293 (5) | 154 (0) | 9020 (8) | |
| COVID-19 | No—escalation was not needed | 11 (0) | 20 (0) | 524 (0) | 13 (0) | 568 (0) | No—escalation was not needed | 4 (4) | 13 (0) | 483 (0) | 20 (0) | 520 (0) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 20 (0) | 16 (0) | 549 (0) | 14 (0) | 600 (1) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 14 (0) | 34 (0) | 659 (0) | 17 (0) | 725 (1) | |
| Yes | 16 (0) | 22 (0) | 375 (0) | 7 (0) | 420 (0) | Yes | 6 (0) | 18 (0) | 258 (0) | 5 (0) | 287 (0) | |
| Total | 47 (0) | 58 (0) | 1448 (1) | 34 (0) | 1588 (1) | Total | 24 (0) | 65 (0) | 1400 (1) | 42 (0) | 1532 (1) | |
| Other | No—escalation was not needed | 39 (0) | 45 (0) | 560 (0) | 12 (0) | 657 (1) | No—escalation was not needed | 19 (0) | 29 (0) | 352 (0) | 23 (0) | 423 (1) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 114 (0) | 86 (0) | 546 (0) | 16 (0) | 763 (1) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 68 (0) | 67 (0) | 533 (0) | 25 (0) | 694 (1) | |
| Yes | 125 (0) | 106 (0) | 430 (0) | 12 (0) | 674 (1) | Yes | 25 (0) | 28 (0) | 278 (0) | 6 (0) | 337 (1) | |
| Total | 278 (0) | 237 (0) | 1536 (1) | 40 (0) | 2093 (2) | Total | 112 (0) | 124 (0) | 1163 (1) | 54 (0) | 1454 (1) | |
| Total | No—escalation was not needed | 2659 (0) | 5505 (5) | 40 915 (36) | 734 (1) | 49 813 (43) | No—escalation was not needed | 1731 (2) | 4198 (4) | 35 863 (32) | 939 (1) | 42 731 (39) |
| N/A—the pharmacist was the person who spoke to the patient about their symptoms | 4257 (4) | 4965 (4) | 29 028 (25) | 353 (0) | 38 603 (34) | N/A—the pharmacist was the person who spoke to the patient about their symptoms | 4389 (4) | 6574 (6) | 39 804 (36) | 606 (1) | 51 373 (46) | |
| Yes | 3859 (39 | 4653 (4) | 17 879 (16) | 287 (0) | 26 678 (23) | Yes | 2017 (2) | 2919 (3) | 11 266 (10) | 215 (0) | 16 417 (15) | |
| Total | 10 775 (9) | 15 123 (13) | 87 822 (76) | 1374 (1) | 115 094 (100) | Total | 8137 (7) | 13 691 (12) | 86 933 (79) | 1760 (2) | 110 521 (100) | |
| Symptoms requiring further escalation outside of community pharmacy | Number of patients (%) 2022–23 | Number of patients (%) 2023–24 |
|
|---|---|---|---|
| No | 101 846 (88) | 102 271 (93) | <0.001 |
| Yes | 13 248 (12) | 8250 (7) | <0.001 |
| Total | 115 094 (100) | 110 521 (100) |
| Number of urgent referrals (%), 2022–23 | Number of urgent referrals (%), 2023–24 |
| |
|---|---|---|---|
| Signposted | |||
| Immediately | 6859 (6) | 4075 (4) | <0.001 |
| If symptoms did not improve within 48 h | 3082 (3) | 2044 (2) | <0.001 |
| If symptoms got worse | 2929 (3) | 1905 (2) | <0.001 |
| N/A (not referred to other services) | 378 (0) | 226 (0) | <0.001 |
| Total number of patients | 115 094 | 110 521 | |
| Escalation destination | |||
| Yes—GP | 5507 (5) | 3333 (3) | <0.001 |
| Yes—out-of-hours/NHS 111 service | 980 (1) | 504 (0) | <0.001 |
| Yes—Accident and Emergency | 280 (0) | 177 (0) | <0.001 |
| Yes—other | 92 (0.08) | 61 (0.06) | <0.05 |
| Total number of patients | 115 094 | 110 521 |
| Type of escalation symptoms identified for immediate referral | Number of symptoms (%), 2022–23 | Number of symptoms (%), 2023–24 |
|
|---|---|---|---|
| Symptoms are getting worse | 3927 (42) | 2511 (47) | <0.001 |
| Difficulty breathing | 953 (10) | 455 (9) | <0.001 |
| Difficulty swallowing or are drooling | 834 (9) | 422 (8) | <0.001 |
| Chest pains | 684 (7) | 395 (7) | <0.001 |
| Severe headache and vomiting | 318 (3) | 139 (3) | <0.001 |
| Skin is very cold | 324 (4) | 95 (2) | <0.001 |
| Coughing up blood | 289 (3) | 218 (4) | <0.001 |
| Confusion, very drowsy or have slurred speech | 142 (2) | 49 (1) | <0.001 |
| Passed little to no urine | 108 (1) | 68 (1) | <0.001 |
| Other (non-specified symptoms) | 1682 (18) | 974 (18) | <0.001 |
| Total | 9261 (100) | 5326 (100) |
| OTC medicines offered to patient | Consultations (%), 2022–23 | Consultations (%), 2023–24 |
|
|---|---|---|---|
| Yes—supplied | 91 480 (80) | 93 057 (84) | <0.001 |
| Yes—declined | 6071 (5) | 5286 (5) | <0.001 |
| No | 17 543 (15) | 12 178 (11) | <0.001 |
| Total | 115 094 (100) | 110 521 (100) |
| Self-care advice given | 2022–23 | 2023–24 |
|
|---|---|---|---|
| Yes—verbal advice only provided | 73 850 (64) | 72 528 (65) | <0.001 |
| Yes—verbal advice and patient information leaflets provided | 35 624 (31) | 34 242 (31) | 0.8801 |
| No | 5620 (5) | 3751 (3) | <0.001 |
| Total | 115 094 (100) | 110 521 (100) |
- —NHS England
- —Department of Health and Social Care10.13039/501100000276
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmaceutical Practices and Patient Outcomes · Medication Adherence and Compliance · Antibiotic Use and Resistance
Introduction
The greatest proportion of antibiotics for human use are prescribed in the primary healthcare sector for the treatment of two common infections—respiratory tract infection (RTI) and urinary tract infection (UTI).^1^ Barriers to appropriate antibiotic use include patients demanding antibiotics, the perception that patients expect antibiotics, and prescribing antibiotics to save time rather than explain why antibiotics are not needed.^2–4^
Upper RTIs (URTIs) are primarily caused by viruses or bacteria infecting the nose, sinuses, pharynx and larynx.^5^ The infections present acutely, when patients can experience laryngitis, pharyngitis, nasopharyngitis and rhinitis whilst complaining of symptoms such as a cough, sore throat or sinusitis.^6^ As the majority of the URTIs are viral in nature, there is limited evidence that antibiotics are effective in treating these conditions in adults and children.^7^ However, in England, it is common for patients to attend GP appointments where there is a 50%–100% chance of receiving an antibiotic such as amoxicillin.^8,9^
Community pharmacy teams are trusted members of the healthcare workforce, with community pharmacies being open at unsocial hours and at weekends.^10^ It is common for patients to seek over-the-counter (OTC) remedies for symptom relief. Some of these medications are classified as pharmacy-only or ‘P’ medicines and can only be bought under a pharmacist’s supervision. Pharmacy teams utilize patient symptoms and past medical history to assess which product(s) are suitable. These conversations provide an opportunity to offer symptom management advice to the patient.
Outcome 2 of the UK’s 5-year National Action Plan on AMR states: ‘By 2029, the public are empowered and equipped to engage on and help address AMR through an improved understanding of the scale and nature of the risk, and the individual behavioural actions that can be taken to address it’.^11^
The UK Health Security Agency (UKHSA)-led ‘Treat Antibiotics Responsibly Guidance, Education and Tools’ (TARGET) Toolkit consists of a range of evidence-based tools to support and promote antimicrobial stewardship (AMS) for healthcare professionals and patients.^12^
The TARGET Treating Your Infection leaflets for RTI (TYI-RTI) are designed for healthcare professionals to have structured discussions with patients about their symptoms (Figure 1).^13^ They can be tailored and personalized to patients, to explain the average duration of their ailment, self-care and management of their symptoms with safety-netting, advising when patients should seek further advice and reconsult with a healthcare professional.^12,14^
TARGET: TYI-RTI leaflet.
Since 2020, England’s community pharmacy teams have received AMS and infection prevention and control (IPC) training, as well as being incentivized to use the TARGET tools through the Pharmacy Quality Scheme (PQS).^15–17^ The PQS is designed to reward community pharmacy contractors for delivering three quality dimensions, specifically clinical effectiveness, patient safety and patient experience.^18^ In 2023–24, the PQS re-incentivized all three TARGET Tools—the TARGET Antibiotic Checklist, and the TARGET TYI leaflets for both RTI and UTI.^19^ This study evaluates the 2 years 2022–23 and 2023–24 and the impact of the TARGET TYI-RTI leaflets in community pharmacy, comparing the uptake of the leaflets, staff groups using the leaflets, and numbers of patients adequately managed in the pharmacy, including identifying triggers for escalation and OTC recommendations.
Materials and methods
The detailed methodology has been outlined previously, where both TARGET TYI leaflets for UTI and RTI were incentivized simultaneously.^17^
Study design
This is a service evaluation of the scaling of the use of the TARGET TYI-RTI leaflet in community pharmacies via the national incentive scheme. In this structured observational study, researchers assessed the outcomes of how community pharmacists implemented the use of the leaflets within the AMS domain of the PQS criteria.
Setting and participants
There were 11 051 and 11 043 registered community pharmacies in England in March 2023 and March 2024, respectively.^20^ Community pharmacy teams were asked to record data from walk-in patients requesting advice for the management of symptoms of RTIs. Community pharmacy teams consist of registered pharmacy professionals (pharmacists and technicians) and non-registered pharmacy staff (trainee pharmacists, trainee technicians, dispensary staff and medicines counter assistants), all being patient-facing staff who provide advice on medicines.
Any patient with RTI symptoms was eligible for inclusion. The data collected were subdivided by age, specifically patients under 5 years of age, over 5 (up to 17 years) and adults (18 years and over).^21^ The follow-up of the outcome of patients signposted to other healthcare settings was outside the scope of this study.
Data collection
Pharmacy teams were required to submit the data collected via the Manage Your Service (MYS) software portal by either the date of their PQS declaration or no later than 31 March 2023 or 31 March 2024. They could complete the data collection from the launch of the scheme on 10 October 2022 to its closure on 31 March 2023 in PQS 2022–22, and from 1 June 2023 to 31 March 2024 for PQS 2023–24. The NHS Business Services Authority (NHSBSA) produced a digital version of the questions from the TARGET TYI leaflets, which pharmacy teams were required to input for data collection. These were made available to all pharmacy contractors via the MYS portal for data submission. A single form submission was required per patient. Pharmacy teams could complete the data collection at any timepoint during the duration of the PQS.
The results from the PQS 2022–23 TARGET TYI-RTI data were published on the NHS England website, with findings and recommendations that community pharmacy teams needed to implement into day-to-day practice.^22^ The use of the TARGET TYI-RTI leaflets was re-incentivized in the PQS 2023–24, where pharmacy teams were asked to use this resource after implementing the findings and recommendations from the report.^21^
Data analysis
Descriptive analysis was conducted by using R statistical software version 4.2.1 (R Foundation for Statistical Computing) and the results were reported as frequencies and percentages.
Ethics
This study is a service evaluation and therefore did not require ethical approval.^17^ Further institutional ethical approval was not required, as confirmed through the UKHSA Research Ethics and Governance Group and the NHS Health Research Authority Decision tool. No patient identifiable data were recorded within the data collection. All files were handled in accordance with the Data Protection Act 2018 and the UK General Data Protection Regulation (GDPR). All community pharmacies consented to participate through the online portal.
Results
A total of 225 615 patients were reviewed using the TARGET TYI-RTI leaflets over the 2 years, with 7525 community pharmacies participating in either PQS scheme, and 7407 community pharmacies participating in both PQS schemes. A total of 115 094 TARGET TYI-RTI leaflets were submitted in 2022–23 and 110 521 in 2023–24. Assessment using the TARGET TYI-RTI leaflet was mainly via the pharmacist in both years [44% (50 799) in 2022–23, and 46% (51 373) in 2023–24], followed by the pharmacy technicians/dispensers [27% (31 609) in 2022–23, and 26% (28 500) in 2023–24], counter staff and trainee pharmacists [4% (4774) in 2022–23, and 4% (4655) in 2023–24] (Figure 2). Most patients being assessed were adults in both years [76% (87 822) in 2022–23, and 79% (86 933) in 2023–24], with children over 5 years accounting for 13% (15 123) in 2022–23, and 12% (13 691) in 2023–24, and children under 5 years accounting for 9% (10 775) in 2022–23, and 7% (8137) in 2023–24] (Figure 2).
Community pharmacy consultations for an RTI during the 2022–23 and 2023–24 PQSs. (a) Pharmacy staff role managing the patient; (b) RTI consults by patient age.
The most frequently suspected infections were similar for both years, with cough and bronchitis being the most common symptoms [33% (45 822) in 2022–23, and 31% (38 848) in 2023–24], followed by sore throat, [25% (34 220) in 2022–23, and 25% (31 099) in 2023–24] and the common cold [22% (29 802) in 2022–23, and 23% (28 627) in 2023–24] (Table 1). COVID-19 infections were one of the lowest types of infection for both years with only 1% (1587) infections in 2022–23, and 1% (1531) in 2023–24.
Forty-three percent (49 813) of patients in 2022–23, and 39% (42 731) in 2023–24 were seen and managed by community pharmacy teams, requiring no escalation to the pharmacist. The pharmacists dealt with more patients in 2023–24 (46%; 51 373) compared with 2022–23 (34%; 38 603). There was a decline in the number of patients requiring escalation to the pharmacist from 23% (26 678) in 2022–23 to 15% (16 417) in 2023–24 (Table 2).
From these consultations, 12% (13 248) of patients were signposted to another healthcare provider in 2022–23, and 7% (8250) in 2023–24, of which 6% (6859) required immediate escalation in 2022–23, and 4% (4075) in 2023–24 (Table 3). The most common signposting destination was the patient’s GP [5% (5507) in 2022–23, and 3% (3333) in 2023–24] (Table 4).
The most common types of reason for escalation identified for immediate referral were ‘symptoms getting worse’ [42% (3927) in 2022–23, and (47%) 2511 in 2023–24] and other (non-specified symptoms) [18% (1682) in 2022–23, and 18% (974) in 2023–24] (Table 5). Confusion, being very drowsy or having slurred speech was one of the least common symptoms in both years [2% (142) in 2022–23, and 1% (49) in 2023–24]. Passing little to no urine was the least common escalation symptom [1% (108) patients in 2022–23, and 1% (68) in 2023–24].
Most patients were offered OTC remedies [85% (97 551) in 2022–23, and 89% (98 343) in 2023–24], of which the majority accepted [80% (91 480) in 2022–23, and 84% (93 057) in 2023–24]. There was a decline in the number of patients who were not offered any OTC remedies [15% (17 543) in 2022–23 to 11% (12 178) in 2023–24] (Table 6). The most common OTC remedies were pain relief medication, expectorant cough syrups, throat lozenges and oral decongestants in both years. In contrast, nasal sprays and all-in-one preparations were the least commonly offered OTC remedies.
Self-care advice was given to 95% (109 474) of patients in 2022–23, with 31% (35 624) receiving additional patient information leaflets, and 97% (106 770) in 2023–24, of whom 34 242 (31%) received additional patient information leaflets (Table 7).
Discussion
Use of the TARGET TYI-RTI leaflets and escalations
Most patients were managed within the community pharmacy, with a significant proportion being managed by the extended community pharmacy team, (technicians and counter staff), which increased from 2022–23 to 2023–24. Further, fewer patients in 2023–24 required escalation outside the community pharmacy to other healthcare providers such as GPs. Evidence from the principal findings of a cohort study showed that it is very unlikely that patients would develop pneumonia within 7 days of an RTI illness against predictive indicators such as pulse, temperature, chest crackles and O_2_ saturation levels, and therefore would not require a course of antibiotics.^23^ Patient reassurance is supported by the TARGET TYI-RTI leaflet, which explains which symptoms require escalation, as well as reassuring patients about the trajectory of current ones.^24^ These findings agree with a randomized controlled trial (RCT) confirming that the use of the leaflet was associated with a lower likelihood of referrals to GPs for certain RTIs (P < 0.05) and more frequent provision of self-care advice than the control group (P = 0.06).^14^
As part of historic PQS, community pharmacists have also received red flag and sepsis training, and are therefore able to assess patients’ symptoms so they can receive the similar/same assessment that they would have received with the GP or an urgent care centre (UCC) setting.^25^ An explanation for the reduction in the referrals could be the launch of the Community Pharmacy—Pharmacy First service. This service was launched on 31 January 2024, where patients in England can receive treatment (and, if appropriate, antibiotics) for seven common conditions including sinusitis, sore throat and ear infection.^26^
Antibiotics are often misused because they are thought of as ‘benign’ drugs.^27^ Primary care is a key component of a high-performing national healthcare system, where in England, the majority of antibiotics are prescribed.^28^ It is therefore important that the public is regularly educated to push positive behaviours regarding antibiotic use and to promote AMS. The TARGET TYI-RTI leaflets allow structured conversations with patients specific to the most common ailment—RTI. It is also important for healthcare professionals, particularly community pharmacy teams, to be aware of the latest evidence-based research, which can be applied practically to counsel their patients. The TARGET TYI-RTI leaflets have aided in England’s community pharmacies counselling and educating patients about their symptoms, helping to safety-net and reassure patients, as well as escalate where appropriate. This in turn can help with reducing inappropriate GP appointments and hospital admissions, and prevent the inappropriate use of emergency departments. The use of incentivization via the PQS has allowed significant clinical progress in and awareness of AMS to be made at pace for all of England’s community pharmacies. It is not clear if such progress could be achieved in any other way.
Self-care, lifestyle advice and benefit from the use of nasal sprays
The majority of patients were offered and supplied with OTC remedies, which showed a statistically significant increase in 2023–24 (84%; 93 057) (P < 0.001). Although only 10% of those who received OTC medicines were given nasal sprays, a recent RCT demonstrated that nasal sprays reduce the duration of illness and the need for antibiotics for URTI symptoms (including coughs, colds, sore throat, sinus or ear infections, influenza or COVID-19).^29^ Evidence suggests that nasal sprays containing carrageenan reduce both the duration and severity of symptoms, whilst saline sprays are thought to reduce the viral load.^30,31^ This is a scalable intervention that has an important and practical role in managing the public during NHS peak times whilst promoting AMS principles.^32^ This intervention is suitable for adults, including those over 65 years of age, with comorbidities (such as heart disease, asthma, lung disease, diabetes, stroke and obesity). Community pharmacy teams should promote this evidence to patients when counselling them. In addition, amendments to the TARGET toolkit resources could also help remind both patients and healthcare professionals about the use of this intervention. Further counselling could promote the use of physical activity (where applicable) and stress management, with the same study showing a reduction in the severity, incidence of symptoms and the use of antibiotics.^29^
Strengths and limitations
Just under a quarter of a million patients were reviewed using the TARGET TYI-RTI leaflets over the 2 years of the PQS, with nearly 7500 community pharmacies participating in both years. Much like similar PQS studies, it is recognized that community pharmacy teams are likely to behave differently when they are incentivized.^16,17,33–35^ Further, there was a decline in participation in the scheme due to the lack of capacity and financial investment.^36^ Further studies could involve extrapolating the use of the TARGET TYI-RTI leaflets with the launch of the Pharmacy First Service (31 January 2024), where community pharmacy is now able to treat patients with antibiotics, if required, for common respiratory infections including sore throat, sinusitis and acute otitis media.^36^
Conclusions
Community pharmacy teams have successfully used the TARGET TYI-RTI leaflets to manage the large number of patients providing self-care and reassurance, as well as safety-netting and when to reconsult a healthcare provider. A significant number of these patients were managed by the wider community pharmacy team and did not require escalation to the pharmacist. Further, few patients required escalation to other healthcare providers and were suitably managed by community pharmacy teams. Implementing the TARGET TYI RTI leaflet—a primary care intervention (which was originally designed for GPs) into existing community pharmacy infrastructure proved scalable, demonstrating its national (and international) potential for AMS impact. There has been significant improvement in AMS within the community pharmacy sector, which has been driven by financial incentivization from the pharmacy quality scheme.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1UK Health Security Agency . English surveillance programme for antimicrobial utilisation and resistance (ESPAUR) Report 2022 to 2023. 2023. https://www.gov.uk/government/publications/english-surveillance-programme-antimicrobial-utilisation-and-resistance-espaur-report.
- 2Butler CC, Rollnick S, Kinnersley P et al Reducing antibiotics for respiratory tract symptoms in primary care: consolidating ‘why’ and considering ‘how’. Br J Gen Pract 1998; 48: 1865–70. https://pmc.ncbi.nlm.nih.gov/articles/instance/1313298/pdf/10198512.pdf 10198512 PMC 1313298 · pubmed ↗
- 3Alves PG, Hayward G, Leydon G et al Antibiotic prescribing in UK out-of-hours primary care services: a realist-informed scoping review of training and guidelines for healthcare professionals. BJGP Open 2021; 5: BJGPO.2020.0167. 10.3399/BJGPO.2020.016733757961 PMC 8278500 · doi ↗ · pubmed ↗
- 4Teixeira Rodrigues A, Roque F, Falcão A et al Understanding physician antibiotic prescribing behaviour: a systematic review of qualitative studies. Int J Antimicrob Agents 2013; 41: 203–12. 10.1016/j.ijantimicag.2012.09.00323127482 · doi ↗ · pubmed ↗
- 5Wang DY, Eccles R, Bell J et al Management of acute upper respiratory tract infection: the role of early intervention. Expert Rev Respir Med 2021; 15: 1517–23. 10.1080/17476348.2021.198856934613861 · doi ↗ · pubmed ↗
- 6Incze M, Grady D, Gupta A. I have a cold—what do I need to know? JAMA Intern Med 2018; 178: 1288. 10.1001/jamainternmed.2018.262130014134 · doi ↗ · pubmed ↗
- 7NICE . Respiratory Tract Infections—Antibiotic Prescribing: Prescribing of Antibiotics for Self-Limiting Respiratory Tract Infections in Adults and Children in Primary Care. NICE Clinical Guidelines, No. 69. 2008. https://www.ncbi.nlm.nih.gov/books/NBK 53632/.21698847 · pubmed ↗
- 8Ashworth M, Charlton J, Ballard K et al Variations in antibiotic prescribing and consultation rates for acute respiratory infection in UK general practices 1995–2000. Br J Gen Pract 2005; 55: 603–8.16105368 PMC 1463221 · pubmed ↗