Amyloid Deposits in a Bone Marrow Biopsy Alongside a Presumed Causative Clone
Rahul Banerjee, Marie K. Das, Kelly D. Smith

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
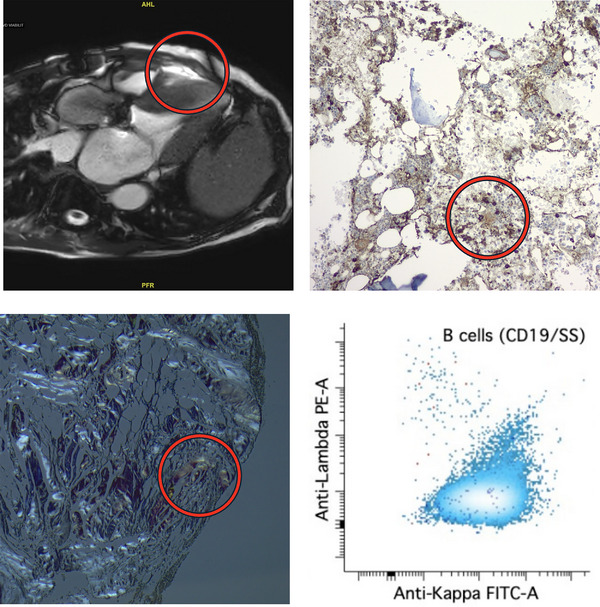 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmyloidosis: Diagnosis, Treatment, Outcomes · Hematological disorders and diagnostics · Bone and Joint Diseases
1
A 73‐year‐old male presented with worsening exertional dyspnea. Transthoracic echocardiography showed normal left ventricular size, preserved left ventricular ejection fraction (55%–60%), severe biatrial enlargement, and a dense speckling pattern. The left ventricular posterior wall measured 2.1 cm and the intraventricular septum measured 2.6 cm during diastole. Given that diastolic wall thicknesses over 1.2 cm can be seen in cardiac amyloidosis [1], this raised suspicion for an infiltrative process rather than more common processes such as hypertensive cardiomyopathy. Indeed, cardiac magnetic resonance imaging (top left) showed late gadolinium enhancement consistent with cardiac amyloidosis.
The patient denied any neuropathy and no pedal edema was noted on examination. While serum protein electrophoresis (SPEP) and serum immunofixation were unremarkable, serum kappa free light chain (FLC) was elevated at 54.4 milligrams per liter (mg/L, upper limit of normal [ULN] 19.4 mg/L). The serum lambda FLC was 8.5 mg/L (ULN 26.3 mg/L), yielding an abnormally elevated FLC ratio of 6.4 (reference range: 0.26–1.65). Troponin I was 0.041 nanograms per milliliter (ng/mL, ULN 0.110 ng/mL), but N‐terminus pro B‐type natriuretic peptide (nt‐proBNP) was significantly elevated at 4510 picograms per milliliter (pg/mL, ULN 125 pg/mL). Immunohistochemistry for kappa light chain on a trephine bone marrow (BM) core biopsy revealed that the majority of plasma cells and small lymphocytes were kappa‐restricted (top right). Congo red staining of the same specimen was positive with green birefringence in periosteal tissue (bottom left). Flow cytometry showed an abnormal kappa‐restricted population (bottom right) of CD5‐variable CD10‐negative B cells phenotypically consistent with marginal zone lymphoma (MZL). No MYD88 or CXCR4 mutations were noted.
Given the presence of Congo red positivity with a presumed causative clone within the same biopsy sample, a diagnosis of AL amyloidosis secondary to MZL was made. While rare, this entity has been reported [2]. The patient was immediately scheduled to begin rituximab and bendamustine, given his worsening symptoms; however, he opted to defer treatment to seek a second opinion at our center. We performed amyloid typing using liquid chromatography with tandem mass spectrometry (using methods described previously) [3], which demonstrated ATTR (transthyretin)‐type amyloidosis. The patient was instead started on the transthyretin stabilizer tafamidis and experienced gradual improvement in his dyspnea.
This case reinforces the importance of typing amyloidosis in virtually all cases. Late gadolinium enhancement and an FLC ratio over 5.0 are collectively quite suggestive of AL amyloidosis [4], especially when a lymphoproliferative clone is identified simultaneously. However, over 10% of cases of cardiac amyloidosis with abnormal SPEP/FLC results and BM amyloid deposits are actually due to ATTR deposition [5]. Periosteal congophilic deposits, although more common in ATTR amyloidosis, can be seen in AL amyloidosis as well [5]. While the desire to initiate treatment quickly is understandable for symptomatic patients, a complete diagnostic workup is mandatory given the high frequency of concurrent abnormal SPEP/SFLC results in older adults with ATTR amyloidosis (Figure 1). In our case, a brief delay for amyloid typing led to initiation of the correct treatment without unnecessary exposure to the potentially serious toxicities of alkylating agents such as bendamustine [6].
Workup for a patient with cardiac amyloidosis.
Author Contributions
R.B. wrote the first draft. R.B., M.K.D., and K.D.S. provided critical feedback and approved the final manuscript.
Funding
The authors have nothing to report.
Consent
The patient provided consent for de‐identified discussion of his case.
Conflicts of Interest
R.B. reports consulting: Abbvie, Adaptive Biotech, BMS, Caribou Biosciences, Genentech, Gilead/Kite, GSK, Janssen, Karyopharm, Legend Biotech, Pfizer, Poseida Therapeutics, Sanofi, SparkCures; Research: Abbvie, BMS, Janssen, Novartis, Pack Health, Prothena, Sanofi. The other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. A. Gertz , R. Comenzo , R. H. Falk , et al., “Definition of Organ Involvement and Treatment Response in Immunoglobulin Light Chain Amyloidosis (AL): A Consensus Opinion From the 10th International Symposium on Amyloid and Amyloidosis,” American Journal of Hematology 79, no. 4 (2005): 319–328, 10.1002/ajh.20381.16044444 · doi ↗ · pubmed ↗
- 2C. Parale , H. Parale , and G. Parale , “Cardiac Amyloidosis Associated With Marginal Zone Lymphoma,” European Heart Journal‐Case Reports 9, no. 8 (2025): ytaf 359, 10.1093/ehjcr/ytaf 359.40800551 PMC 12342999 · doi ↗ · pubmed ↗
- 3W. S. Phipps , K. D. Smith , H.‐Y. Yang , et al., “Tandem Mass Spectrometry–Based Amyloid Typing Using Manual Microdissection and Open‐Source Data Processing,” American Journal of Clinical Pathology 157, no. 5 (2022): 748–757, 10.1093/ajcp/aqab 185.35512256 PMC 9071319 · doi ↗ · pubmed ↗
- 4M. K. Halushka , G. Eng , A. B. Collins , D. P. Judge , M. J. Semigran , and J. R. Stone , “Optimization of Serum Immunoglobulin Free Light Chain Analysis for Subclassification of Cardiac Amyloidosis,” Journal of Cardiovascular Translation Research 8, no. 4 (2015): 264–268, 10.1007/s 12265-015-9628-2.25925232 · doi ↗ · pubmed ↗
- 5A. Chiu , S. Dasari , P. J. Kurtin , et al., “Bone Marrow Amyloid: A Comprehensive Analysis of 1,469 Samples, Including Amyloid Type, Clinical Features, and Morphologic Distribution,” Amyloid 29, no. 3 (2022): 156–164, 10.1080/13506129.2022.2031963.35135386 · doi ↗ · pubmed ↗
- 6P. Martin , P. M. Barr , L. James , A. Pathak , and B. Kahl , “Long‐Term Safety Experience With Bendamustine for Injection in a Real‐World Setting,” Expert Opinion on Drug Safety 16, no. 6 (2017): 647–650, 10.1080/14740338.2017.1318125.28395515 · doi ↗ · pubmed ↗