Single-stage repair of aortic arch hypoplasia and ventricular septal defect in a low-weight infant: a case report from a resource-limited center
Jesús García Pinzás, Cristhian J Cueva Alvarez, Martin Crosby Barabino

TL;DR
A low-weight newborn with a severe heart defect underwent successful one-stage surgery in a resource-limited setting.
Contribution
Demonstrates the feasibility of complex cardiac surgery in low-resource environments using adapted techniques.
Findings
A newborn with aortic arch hypoplasia and VSD underwent successful one-stage surgical repair.
The procedure used an interdigitating patch and SACP via direct cannulation in a low-resource setting.
The infant had an excellent clinical outcome despite limited equipment and monitoring.
Abstract
Aortic arch hypoplasia associated with ventricular septal defect (VSD) is a life-threatening congenital condition that demands early intervention. In low-resource settings, the lack of advanced tools complicates the safe use of selective antegrade cerebral perfusion (SACP) and innovative repair techniques such as interdigitating patch reconstruction. We describe the case of a newborn with severe aortic arch hypoplasia and a large perimembranous VSD who underwent successful one-stage surgical correction. The repair included aortic arch reconstruction using an interdigitating bovine pericardial patch and VSD closure under SACP delivered via direct brachiocephalic trunk cannulation. Despite the challenges of limited monitoring and equipment, the infant had an excellent clinical outcome. This case highlights the feasibility of adapting high-complexity cardiac techniques in resource-limited…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
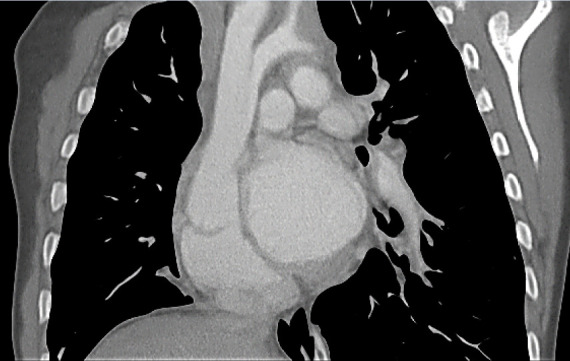 Figure 1
Figure 1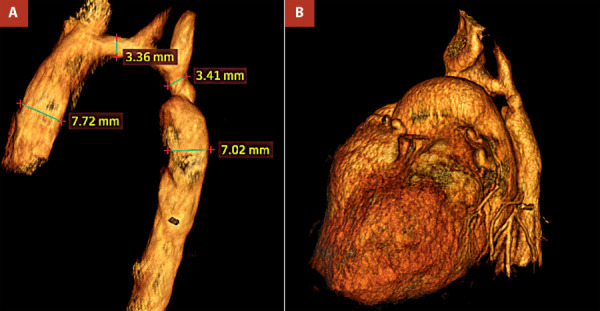 Figure 2
Figure 2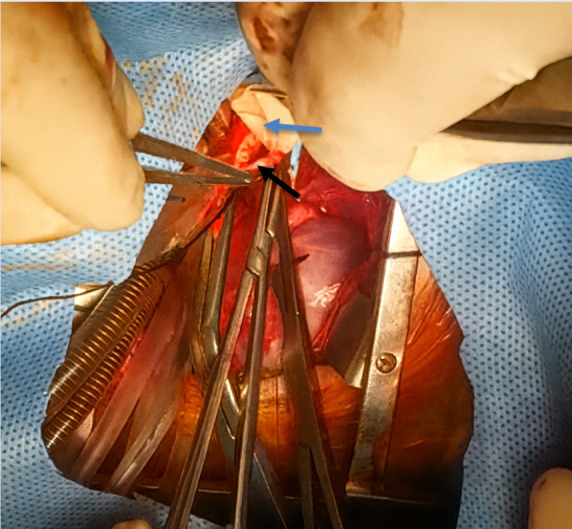 Figure 3
Figure 3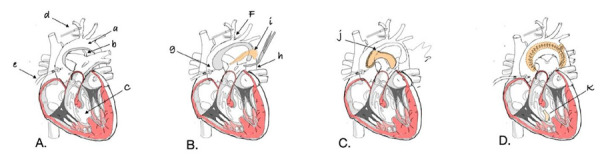 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Congenital Diaphragmatic Hernia Studies · Aortic Disease and Treatment Approaches
Introduction
Aortic arch hypoplasia combined with a ventricular septal defect (VSD) represents a challenging entity in neonatal cardiac surgery. 1 In high-income countries, one-stage neonatal repair using selective antegrade cerebral perfusion (SACP) and patch aortoplasty has become the standard for optimizing outcomes. 2^,^3 The presence of a hypoplastic aortic arch, especially in combination with a VSD, significantly increases the complexity of surgical repair due to altered hemodynamics, the risk of recoarctation, and the need for cerebral and visceral organ protection during cardiopulmonary bypass. 3^-^5
Over the past two decades, selective antegrade cerebral perfusion (SACP) has become the preferred neuroprotective strategy during neonatal aortic arch reconstruction, replacing deep hypothermic circulatory arrest (DHCA) in many high-volume centers. 6^-^8 SACP allows continuous oxygenation of the brain while reducing the risks of neurological injury and systemic inflammation. Various cannulation techniques-including direct brachiocephalic trunk artery cannulation-have been shown to be safe and effective even in neonates. 5^,^6
Nevertheless, these strategies are highly dependent on advanced perfusion equipment, specialized monitoring (e.g., near-infrared spectroscopy), and well-trained perfusion teams. In low-resource settings, these components are often limited or absent. Consequently, the adaptation of neuroprotective strategies such as SACP must be carefully tailored to institutional capacity while maintaining surgical safety. 2^,^9
The surgery was carried out at a tertiary cardiac surgery unit with significant resource limitations, including the absence of advanced cardiac computed tomography (CT), nitric oxide therapy, and extracorporeal membrane oxygenation (ECMO), as well as only three pediatric intensive care unit beds. At the time, no vascular grafts were available. We report the case of a full-term neonate with hypoplastic aortic arch and ventricular septal defect who underwent single-stage repair using selective antegrade cerebral perfusion through direct innominate artery cannulation.
Case report
A full-term male infant was delivered at 38 weeks of gestation with a birth weight of 2,200 g. Soon after birth, he developed respiratory distress with persistent hypoxemia (oxygen saturation around 70% in room air) and signs of congestive heart failure, requiring supplemental oxygen and diuretic therapy.
Echocardiography revealed a large perimembranous ventricular septal defect with a left-to-right shunt, severe transverse aortic arch hypoplasia with critical narrowing at the isthmus, and a large patent ductus arteriosus (PDA) carrying retrograde flow to the descending aorta-indicating ductus-dependent systemic perfusion. CT confirmed the diagnosis, showing marked underdevelopment of the transverse arch and isthmus, with distal systemic flow sustained via the PDA (Figure 1-2).
Figure 1. Computed tomography with coronal view: A severe hypoplasia of the distal aortic arch is observed. The persistent ductus arteriosus is visualized as a vascular connection between the left pulmonary artery and the descending aorta.
Figure 2A. Three-dimensional volume-rendered computed tomography (CT) reconstruction of the thoracic great vessels demonstrates severe hypoplasia of the aortic arch, with significant narrowing of the proximal and distal segments measuring 3.36 mm and 3.41 mm, respectively. A markedly enlarged patent ductus arteriosus (PDA), measuring 7.02 mm, connects the pulmonary artery to the descending aorta. Postductal dilation of 7.72 mm is observed, consistent with retrograde systemic perfusion via the PDA. B. The 3D volume-rendered CT angiogram reveals a markedly hypoplastic transverse aortic arch, with critical narrowing at the level of the PDA, severely compromising the continuity of systemic flow through the arch.
Medical stabilization was achieved with prostaglandin E1 infusion to maintain ductal patency. At one month of age, with a weight of 2,920 g, the patient was taken to the operating room for urgent single-stage repair. Through a median sternotomy, surgical inspection confirmed severe arch hypoplasia, 4 mm at its narrowest point, a large perimembranous VSD (10 mm), and an 8 mm PDA. Cardiopulmonary bypass was established under moderate systemic hypothermia 30 °C. SACP was delivered via direct brachiocephalic trunk cannulation at 25 °C and maintained for 60 minutes during circulatory arrest to allow safe reconstruction of the arch.
The hypoplastic arch was augmented using an anterior bovine pericardial patch with the interdigitating technique, and the PDA was ligated. The VSD was closed with a bovine pericardial patch (Figure 3). Due to myocardial edema, the sternum was left open and closed 24 hours later without infectious complications, with sinus rhythm preserved throughout.
Figure 3. Intraoperative photograph during aortic arch reconstruction in a neonate with severe arch hypoplasia. The anterior bovine pericardial patch is being sutured using the interdigitating technique to augment the hypoplastic aortic arch. Black arrow: Aortic arch. Blue arrow: Pericardial patch.
The postoperative course included transient low cardiac output and supraventricular tachycardia, both of which resolved with medical therapy. The patient was extubated after 72 hours and transferred out of the intensive care unit on postoperative day 9. At discharge, the neurological examination was normal, with preserved reflexes, spontaneous limb movements, and visual tracking.
By the last follow-up in July 2025, six months after surgery, he demonstrated normal psychomotor development, no neurological deficits, and weighed 8 kg.
Discussion
The coexistence of severe aortic arch hypoplasia and a large perimembranous VSD in a neonate represents a critical surgical challenge. Early complete repair is preferred to avoid circulatory instability, minimize pulmonary overcirculation, and prevent irreversible end-organ dysfunction. 1^,^2 The current case highlights the feasibility of performing such complex reconstruction in a resource-limited setting, utilizing SACP and interdigitating arch augmentation, strategies typically reserved for high-complexity centers.
In recent decades, one-stage repair with arch reconstruction and VSD closure has become standard for neonates with complex aortic arch obstruction. 3^,^4 Several techniques for arch reconstruction are described, including extended end-to-end, end-to-side, and patch aortoplasty. Among these, the interdigitating technique has demonstrated superior anatomical alignment and reduced rates of restenosis or reintervention. 10 In a series by Winder et al., the interdigitating method decreased reintervention rates from 31% to 13%, even in Norwood patients. 10 Our decision to employ an anterior bovine pericardial patch with interdigitating suture was guided by the arch geometry and the desire to minimize tension and maintain laminar flow across the repair site. 10^,^11 A schematic diagram of the surgical technique, detailing the placement of the patch and interdigitating suture, is presented to illustrate the procedure (Figure 4).
Figure 4. Schematic representation of the surgical technique. (A) Depicts the hypoplastic aortic arch (a), persistent ductus arteriosus (b), and ventricular septal defect (c). Arterial cannulation (d) is performed through the brachiocephalic artery, and a coronary perfusion cannula (e) is inserted into the ascending aorta. (B) At 28°C, the brachiocephalic artery (f), ascending aorta (g), and descending aorta (h) are clamped to enable continuous selective cerebral and myocardial perfusion while performing aortic arch reconstruction with a bovine pericardial patch (i). (C) Following aortoplasty, cardiac arrest is induced, and the proximal anastomosis is performed with the open ascending aorta (j). (D) Finally, systemic flow is resumed, rewarming is initiated, and the ventricular septal defect is closed with a heterologous patch (k). Illustration created by the author.
Cerebral protection is paramount during arch reconstruction. Historically, DHCA was widely used but has been associated with an increased risk of neurologic injury and delayed neurodevelopment. 6^,^7 SACP is now favored in many centers due to its superior metabolic and neurological profile. 8^,^9^,^12^-^15 Studies such as those by Soynov et al. and Kulyabin et al. support the use of SACP in neonates, showing preserved end-organ function, stable lactate clearance, and lower biomarkers of neurologic injury. 3^,^15 Our patient underwent SACP via direct brachiocephalic artery cannulation, a technique shown to be safe and reproducible even in neonates with small vessel diameters. 5 Despite a 60-minute arrest period, the patient had no postoperative neurologic deficits, highlighting the protective effect of SACP, even without neuromonitoring.
This is particularly relevant in low-resource environments, where near-infrared spectroscopy (NIRS), continuous electroencephalography, or dedicated perfusion teams may be unavailable. Studies like those of Fraser and Andropoulos emphasize the critical balance between technique and available infrastructure. 13 Our approach relied on meticulous perfusion control and team coordination, using SACP at moderate hypothermia (25 °C) to maintain cerebral flow while minimizing systemic ischemia.
Moreover, anatomical definitions of arch hypoplasia vary. Parikh et al. proposed using arch diameter ratios specifically distal transverse arch diameter/carotid artery diameter (DT/CA < 0.9), as an indicator of the surgical threshold for median sternotomy and full arch repair. 16 Our patient’s transverse arch measured 4 mm, consistent with severe hypoplasia. 16 Additional data from Li et al. and Margarint et al. support early intervention in patients with borderline arch geometry to prevent systemic hypertension and long-term recoarctation. 11^,^17
Despite transient postoperative supraventricular tachycardia and low cardiac output, our patient stabilized with medical therapy. Notably, sternal closure was delayed for 24 hours, a strategy often adopted to reduce tamponade risk in neonates with myocardial edema. 8 The absence of infectious complications and the preserved neurological status at discharge support the overall safety of our approach.
Finally, this case demonstrates that advanced surgical techniques can be successfully applied in resource-constrained settings, provided that the core principles of congenital heart surgery are respected and adapted. As echoed by Kozyrev et al. and Onalan et al., even in less equipped centers, structured protocols, careful perfusion planning, and judicious technique selection can yield outcomes comparable to those of high-volume institutions. 7^-^9
In conclusion this case demonstrates the feasibility of one-stage aortic arch and VSD repair in low-weight infants within resource-limited centers. The use of an interdigitating patch and direct SACP provided anatomical and neurological protection, even in the absence of advanced support tools. Such results reinforce the viability of evidence-based approaches in diverse healthcare contexts. 11^,^16
Our experience reinforces that meticulous surgical planning, adherence to cerebral protection principles, and adaptation of high-complexity techniques are essential to improving outcomes for neonates with complex congenital heart disease even in centers with limited resources. This case highlights a replicable model for other institutions facing similar constraints and contributes to the growing global discourse on equity and excellence in pediatric cardiac surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Doyurgan O Balik H Aortic arch repair with extended end-to-side anastomosis in neonates and infants with transverse arch hypoplasia J Surg Med 20237850450810.28982/josam.7905 · doi ↗
- 2Provost B Fournier E Hascoët S Le Bret E Roussin R Zoghbi J Aortic coarctation associated with distal aortic arch hypoplasia in neonates can be effectively repaired through left thoracotomy J Card Surg 202338755956610.1155/2023/5599161 · doi ↗
- 3Kulyabin YY Bogachev-Prokophiev AV Soynov IA Omelchenko AY Zubritskiy AV Gorbatykh YN Clinical assessment of perfusion techniques during surgical repair of coarctation of aorta with aortic arch hypoplasia in neonates Semin Thorac Cardiovasc Surg 202032486087110.1053/j.semtcvs.2020.04.01532446921 · doi ↗ · pubmed ↗
- 4Kilic Y Selcuk A Korun O Ceyda H Cicek M Yurdakok O Comparison of cases with and without additional lower body perfusion in newborns undergoing aortic arch reconstruction with antegrade selective cerebral perfusion Turk Gogus Kalp Damar 202230219219810.5606/tgkdc.dergisi.2022.22805 PMC 947359136168563 · doi ↗ · pubmed ↗
- 5Amir G Frenkel G Shukrun G Gogia O Bachar O Bruckheimer E Direct innominate artery cannulation for antegrade cerebral perfusion in neonates undergoing arch reconstruction Ann Thorac Surg 201395395696110.1016/j.athoracsur.2012.10.02923261118 · doi ↗ · pubmed ↗
- 6Rüffer A Knieling F Cesnjevar R Regensburger A Purbojo A Dittrich S Equal cerebral perfusion during extended aortic coarctation repair Eur J Cardiothorac Surg 202261229930610.1093/ejcts/ezab 41534718510 · doi ↗ · pubmed ↗
- 7Onalan MA Temur B Aydin S Basgoze S Guzelmeric F Odemis E Management of aortic arch hypoplasia in neonates and infants J Card Surg 202035123737374310.1111/jocs.1521233225505 · doi ↗ · pubmed ↗
- 8Oppido G Napoleone CP Turci S Davies B Frascaroli G Martin-Suarez S Moderately hypothermic cardiopulmonary bypass and low-flow antegrade selective cerebral perfusion for neonatal aortic arch surgery Ann Thorac Surg 20068262233223910.1016/j.athoracsur.2006.06.04217126140 · doi ↗ · pubmed ↗