Current Trends in Antibiotic Resistance Patterns of Pathogens in Urinary Tract Infections in Children in Karaganda, Kazakhstan
Shynar Yeleupayeva, Aigul Dinmukhamedova, Roman Aizman, Zhanat Mukataeva, Bibenur Baidalinova, Saule Bazarbaeva, Muhametkali Zhakupov, Zhanar Rakhimzhanova, Aisulu Kuzenbayeva

TL;DR
This study examines antibiotic resistance in urinary tract infections among children in Kazakhstan, finding higher resistance in older children.
Contribution
The study provides updated antibiotic resistance patterns in pediatric UTIs in Karaganda, highlighting age-related trends.
Findings
E. coli was the most common pathogen, with high resistance to amoxicillin and erythromycin.
Multidrug resistance increased with age, from 28% in infants to 43% in older children.
Imipenem, amikacin, and meropenem showed high effectiveness against E. coli.
Abstract
Urinary tract infections (UTIs) are common in children and result in frequent hospitalization, creating a social and economic burden for parents and the healthcare system. This study analyzes the patterns of antibiotic resistance of dominant uropathogens and assesses the impact of patient age and sex on these patterns. This retrospective cohort study was conducted in Karaganda, Kazakhstan, between 2017 and 2022. Antibiotic resistance was assessed in two age groups: 0-12 months (Group I) and 13-60 months (Group II). Standard microbiological methods were used to identify UTI pathogens, and antibiotic resistance patterns were determined using the Kirby-Bauer disk diffusion method. Among the 519 isolates (68.1%) from 762 children, the most common pathogens were Escherichia coli (170, 32.7%), Enterococcus faecalis (80, 15.4%), and Staphylococcus epidermidiss (46, 8.9%) in both age groups.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
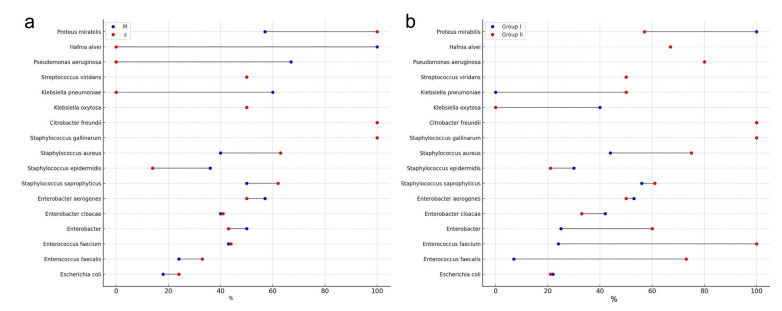 Figure 1
Figure 1| Pathogen | Group I (0-12 months) | Group II (13-60 months) | Total | P values |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||
|
| 85 (29.3) | 85 (37.1) | 170 (32.7) | 0.05 |
|
| 54 (18.6) | 26 (11.3) | 80 (15.4) | 0.02 |
|
| 17 (5.9) | 6 (2.6) | 23 (4.4) | 0.16 |
|
| 4 (1.4) | 5 (2.2) | 9 (1.7) | 0.74 |
|
| 19 (6.5)* | 3 (1.3) | 22 (4.2) | 0.003 |
|
| 15 (5.2) | 8 (3.5) | 23 (4.4) | 0.29 |
|
| 19 (6.5) | 17 (7.4) | 36 (6.9) | 0.73 |
|
| 27 (9.3) | 19 (8.3) | 46 (8.9) | 0.70 |
|
| 9 (3.1) | 4 (1.7) | 13 (2.5) | 0.33 |
|
| 1 (0.3) | - | 1 (0.2) | - |
|
| 1 (0.3) | - | 1 (0.2) | - |
|
| 5 (1.7) | 3 (1.3) | 8 (1.5) | 0.72 |
|
| - | 6 (2.6) | 6 (1.1) | - |
|
| - | 2 (0.9) | 2 (0.4) | - |
|
| 1 (0.3) | 5 (2.2) | 6 (1.1) | 0.03 |
|
| - | 3 (1.3) | 3 (0.6) | - |
|
| 2 (0.7) | 7 (3.0) | 9 (1.7) | 0.05 |
|
| 15 (5.2) | 16 (7.0) | 31 (5.9) | 0.38 |
|
| 16 (5.5) | 14 (6.1) | 30 (5.7) | 0.79 |
| Total | 290 (100) | 229 (100) | 519 (100) |
| Antibiotic | Frequency n (%) | Used as the only agent (n, %) | Combined with | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Furazidine (n, %) | Amikacin (n, %) | Gentamicin (n, %) | Cefuroxime (n, %) | Cefepime (n, %) | Azithromycin (n, %) | Cefotaxime (n, %) | Ceftazidime (n, %) | Nystatin (n, %) | Fluconazole (n, %) | |||
| Ceftriaxone | 238 (35.4) | 118 (49.6) | 53 (22.3) | 42 (17.6) | 4 (1.7) | 9 (3.8) | 1 (0.4) | 11 (4.6) | - | - | - | - |
| Cefuroxime | 221 (32.9) | 82 (37.1) | 42 (19) | 39 (17.6) | 18 (8.1) | - | - | 5 (2.7) | 9 (4.1) | 7 (3.2) | 19 (8.6) | |
| Furazidine | 83 (2.3) | 29 (34.9) | - | - | - | - | - | - | - | - | - | - |
| Amikacin | 82 (12.2) | 71 (86.5) | - | - | - | - | - | - | - | - | - | - |
| Levofloxacin | 48 (7.1) | 41 (85.4) | - | - | - | - | - | - | - | - | - | - |
| Antibiotic | 0-12 months | 13-60 months | Total | P value | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Amoxicillin | S | 10 (23.2) | 16 (26.2) | 26 (25.0) | 0.67 |
| R | 33 (76.7) | 45 (73.8) | 78 (75.0) | ||
| Cefuroxime | S | 90 (72.6) | 46 (55.4) | 136 (65.7) | 0.02 |
| R | 34 (27.4) | 37 (44.6) | 71 (34.3) | ||
| Amikacin | S | 66 (80.4) | 56 (75.7) | 122 (78.2) | 0.43 |
| R | 16 (19.5) | 18 (24.3) | 34 (21.8) | ||
| Ceftriaxone | S | 62 (75.6) | 37 (67.0) | 99 (72.3) | 0.21 |
| R | 20 (24.4) | 18 (33.0) | 38 (27.7) | ||
| Erythromycin | S | 5 (26.3) | 4 (44.4) | 9 (32.1) | 0.24 |
| R | 14 (73.7) | 5 (55.5) | 19 (67.8) | ||
| Gentamicin | S | 23 (62.1) | 35 (77.0) | 58 (69.9) | 0.09 |
| R | 14 (37.8) | 11 (23.0) | 25 (30.1) | ||
| Ceftazidime | S | 35 (56.4) | 44 (72.0) | 79 (64.2) | 0.04 |
| R | 27 (43.5) | 17 (28.0) | 44 (35.8) | ||
| Meropenem | S | 56 (72.7) | 60 (82.0) | 116 (77.3) | 0.24 |
| R | 21 (27.2) | 13 (18.0) | 34 (22.7) | ||
| Cefotaxime | S | 26 (53.1) | 36 (62.1) | 62 (58.0) | 0.32 |
| R | 23 (46.9) | 22 (37.9) | 45 (42.0) | ||
| Cefazolin | S | 17 (34.0) | 25 (57.0) | 42 (44.7) | 0.02 |
| R | 33 (66.0) | 19 (43.0) | 52 (55.3) | ||
| Imipenem | S | 17 (94.4) | 32 (74.4) | 49 (80.3) | 0.05 |
| R | 1 (5.5) | 11 (25.6) | 12 (19.7) | ||
| Levofloxacin | S | 8 (80.0) | 28 (82.3) | 36 (81.8) | 0.83 |
| R | 2 (20.0) | 6 (17.6) | 8 (18.2) | ||
| Оfloxacin | S | 12 (63.1) | 45 (80.0) | 57 (76.0) | 0.01 |
| R | 7 (36.8) | 11 (20.0) | 18 (24.0) | ||
| Furazolidone | S | 17 (70.8) | 43 (81.1) | 60 (77.9) | 0.21 |
| R | 7 (29.2) | 10 (18.9) | 17 (22.1) | ||
| Azithromycin | S | 10 (66.7) | 26 (59.1) | 36 (61.0) | 0.57 |
| R | 5 (33.3) | 18 (40.9) | 23 (39.0) | ||
| Ciprofloxacin | S | 13 (81.2) | 34 (83.0) | 47 (82.4) | 0.83 |
| R | 3 (18.8) | 7 (17.0) | 10 (17.5) | ||
| Cefepime | S | 21 (80.8) | 45 (80.4) | 66 (80.5) | 0.96 |
| R | 5 (19.2) | 11 (19.6) | 16 (19.5) | ||
| Vancomycin | S | 5 (55.5) | 14 (82.0) | 19 (73.1) | 0.06 |
| R | 4 (44.4) | 3 (18.0) | 7 (26.9) | ||
| Ampicillin | S | 5 (33.3) | 8 (33.3) | 13 (33.3) | >0.99 |
| R | 10 (66.7) | 16 (66.6) | 26 (66.7) | ||
| Doripenem | S | 2 (66.7) | 7 (87.5) | 9 (81.8) | 0.04 |
| R | 1 (33.3) | 1 (12.5) | 2 (18.2) | ||
| Antibiotic | First episode of UTI | Relapse | P value | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Amoxicillin | S | 26 (25.0) | 4 (13.0) | 0.24 |
| R | 78 (75.0) | 27 (87.0) | ||
| Cefuroxime | S | 136 (66.0) | 12 (43.0) | 0.03 |
| R | 71 (34.0) | 16 (57.0) | ||
| Amikacin | S | 122 (78.0) | 7 (58.0) | 0.22 |
| R | 34 (22.0) | 5 (42.0) | ||
| Ceftriaxone | S | 99 (72.0) | 9 (60.0) | 0.49 |
| R | 38(28.0) | 6 (40.0) | ||
| Erythromycin | S | 9 (32.0) | 2 (50.0) | 0.89 |
| R | 19 (68.0) | 2 (50.0) | ||
| Gentamicin | S | 58 (70.0) | 10 (67.0) | >0.99 |
| R | 25 (30.0) | 5 (33.0) | ||
| Ceftazidime | S | 79 (64,2) | 13 (52.0) | 0.36 |
| R | 44 (35,8) | 12 (48.0) | ||
| Meropenem | S | 116 (77.0) | 10 (59.0) | 0.17 |
| R | 34 (23.0) | 7 (41.0) | ||
| Cefotaxime | S | 62 (58.0) | 6(67.0) | 0.87 |
| R | 45 (42.0) | 3 (33.0) | ||
| Cefazolin | S | 42 (45.0) | 11 (55.0) | 0.55 |
| R | 52 (55.0) | 9 (45.0) | ||
| Vancomycin | S | 19 (73.0) | 2 (67.0) | >0.99 |
| R | 7 (27.0) | 1 (33.0) | ||
| Furazolidone | S | 60 (78.0) | 5 (71.0) | >0.99 |
| R | 17 (22.0) | 2 (29.0) | ||
| Azithromycin | S | 36 (61.0) | 4 (50.0) | 0.83 |
| R | 23 (39.0) | 4 (50.0) | ||
| Ciprofloxacin | S | 47 (82.0) | 5 (71,5) | 0.85 |
| R | 10 (18.0) | 2 (28,5) | ||
| Ampicillin | S | 13 (33.0) | 2 (25.0) | 0.97 |
| R | 26 (67.0) | 6 (75.0) | ||
| Doripenem | S | 9(82.0) | 3 (75.0) | >0.99 |
| R | 2(18.0) | 1 (25.0) | ||
| Imipenem | S | 49 (80.0) | 1 (25.0) | 0.05 |
| R | 12 (20.0) | 3 (75.0) | ||
| Оfloxacin | S | 57 (76.0) | 8 (67.0) | 0.74 |
| R | 18 (24.0) | 4 (33.0) | ||
| Cefepime | S | 66 (80.0) | 8 (73.0) | 0.84 |
| R | 16 (20.0) | 3 (27.0) | ||
| Levofloxacin | S | 36 (82.0) | 2 (50.0) | 0.39 |
| R | 8 (18.0) | 2 (50.0) | ||
| Antibiotic | P values between | ||||||
|---|---|---|---|---|---|---|---|
| Isolates | 1 and 2 | 1 and 3 | 2 and 3 | ||||
| n (%) | n (%) | n (%) | |||||
| Amoxicillin | S | 12 (32.4) | 6 (28.0) | 2 (28.6) | 0.76 | 0.84 | 0.98 |
| R | 25 (67.6) | 15 (72.0) | 5 (71.4) | ||||
| Cefuroxime | S | 33 (64.7) | 15 (68.0) | 16 (88.9) | 0.84 | 0.05 | 0.05 |
| R | 18 (35.3) | 7 (32.0) | 2 (11.1) | ||||
| Amikacin | S | 45 (90.0) | 24 (83.0) | 8 (73.0) | 0.37 | 0.13 | 0.42 |
| R | 5 (10.0) | 5 (17.0) | 3 (27.0) | ||||
| Ceftriaxone | S | 43 (81.1) | 31 (97.0) | 8 (88.9) | 0.03 | 0.62 | 0.44 |
| R | 10 (18.9) | 1 (3.0) | 1 (11.1) | ||||
| Erythromycin | S | 2 (66.7) | 2 (66.7) | 2 (50.0) | >0.99 | 0.60 | 0.60 |
| R | 1 (33.3) | 1 (33.3) | 2 (50.0) | ||||
| Gentamicin | S | 38 (86.4) | 7 (70.0) | 5 (83.3) | 0.21 | 0.88 | 0.52 |
| R | 6 (13.6) | 3 (30.0) | 1 (16.7) | ||||
| Ceftazidime | S | 22 (64.7) | 12 (52.0) | 6 (66.7) | 0.15 | 0.65 | 0.49 |
| R | 12 (35.3) | 11 (48.0) | 3 (33.3) | ||||
| Meropenem | S | 47 (87.0) | 7 (63.6) | 5 (83.3) | 0.06 | 0.83 | 0.50 |
| R | 7 (13.0) | 4 (36.4) | 1 (16.7) | ||||
| Cefotaxime | S | 25 (78.0) | 14 (58.0) | 9 (90.0) | 0.10 | 0.47 | 0.07 |
| R | 7 (22.0) | 10 (42.0) | 1 (10.0) | ||||
| Cefazolin | S | 19 (76.0) | 10 (66.7) | 5 (83.3) | 0.33 | 0.87 | 0.51 |
| R | 6 (24.0) | 5 (33.3) | 1 (16.7) | ||||
| Imipenem | S | 31 (94.0) | 4 (57.0) | 6 (86.0) | 0.01 | 0.26 | 0.59 |
| R | 2 (6.0) | 3 (43.0) | 1 (14.0) | ||||
| Levofloxacin | S | 21 (81.0) | 7 (77.8) | 3 (75.0) | 0.83 | 0.78 | 0.91 |
| R | 5 (19.0) | 2 (22.2) | 1 (25.0) | ||||
| Оfloxacin | S | 31 (84.0) | 7 (54.0) | - | 0.03 | - | - |
| R | 6 (16.0) | 6 (46.0) | - | ||||
| Furazolidone | S | 29 (88.0) | 15 (75.0) | - | 0.22 | - | - |
| R | 4 (12.0) | 5 (25.0) | - | ||||
| Azithromycin | S | 23 (68.0) | 3 (33.3) | 4 (80.0) | 0.06 | 0.59 | 0.10 |
| R | 11 (32.0) | 6 (66.7) | 1 (20.0) | ||||
| Сiprofloxacin | S | 32 (88.9) | 6 (60.0) | - | 0.03 | - | - |
| R | 4 (11.1) | 4 (10.0) | - | ||||
| Cefepime | S | 45 (82.0) | 7 (63.6) | - | 0.17 | - | - |
| R | 10 (18.0) | 4 (36.4) | - | ||||
| Ampicillin | S | 6 (35.3) | 4 (31.0) | 1 (20.0) | 0.80 | 0.55 | 0.64 |
| R | 11 (64.7) | 9 (69.0) | 4 (80.0) | ||||
| Doripenem | S | 7 (77.8) | - | - | - | - | - |
| R | 2 (22.2) | - | - | ||||
| Pathogen | Total number of isolates (I/II) | Number of multidrug-resistant isolates (I/II) | Prevalence of multidrug-resistant uropatogens (%) (I/II) |
|---|---|---|---|
|
| 170 (85/85) | 37 (19/18) | 22 (22/21) |
|
| 80 (54/26) | 23 (4/19) | 29 (7/73) |
|
| 23 (17/6) | 10 (4/6) | 43 (24/100) |
|
| 9 (4/5) | 4 (1/3) | 44 (25/60) |
|
| 22 (19/3) | 9 (8/1) | 41 (42/33) |
|
| 23 (15/8) | 12 (8/4) | 52 (53/50) |
|
| 36 (19/17) | 21 (10/11) | 58 (53/65) |
|
| 46 (27/19) | 12 (8/4) | 26 (30/21) |
|
| 13 (9/4) | 7 (4/3) | 54 (44/75) |
|
| 1 (1/0) | 1 (1/0) | 100 (100/0) |
|
| 1 (1/0) | 1 (1/0) | 100 (100/0) |
|
| 8 (5/3) | 4 (2/2) | 50 (40/67) |
|
| 6 (0/6) | 3 (0/3) | 50 (0/50) |
|
| 2 (0/2) | 1 (0/1) | 50 (0/50) |
|
| 6 (1/5) | 4 (0/4) | 67 (0/80) |
|
| 3 (0/3) | 2 (0/2) | 67 (0/67) |
|
| 9 (2/7) | 6 (2/4) | 67 (100/57) |
| Total | 458 (259/199) | 157 (72/85) | 34 (28/43) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Pediatric Urology and Nephrology Studies · Escherichia coli research studies
What’s Known
- Urinary tract infections are among the most common and serious diseases in children, leading to frequent relapses and potentially serious complications and requiring significant treatment costs. The prevalence of uropathogens and antibiotic resistance varies by region and medical institution, influenced by local factors, including antibiotic usage, epidemiology, and patient characteristics.
What’s New
- The novelty of this study lies in its geographic, population and demographic specificity, allowing to take into account local features of the prevalence of uropathogens and their resistance, which have not been sufficiently studied in this region before.
- The study allows optimizing the choice of antibacterial drugs, creating a theoretical database and clinical recommendations that will reduce the risks of global antibiotic resistance.
- The dominant uropathogens isolated in the study were Escherichia coli, Enterococcus faecalis, and Staphylococcus epidermidis. Antibiotic resistance was found to increase almost twofold with age, with higher rates of resistance observed in boys compared to girls.
Introduction
Urinary tract infections (UTIs) are the most common and serious infections in children. Every year, more than one million children with UTIs visit a doctor, and 500,000 children are transported to hospitals by emergency services. ^ 1 ^ Moreover, 30-50% of children with a UTI have subsequent relapses. ^ 2 ^ The primary incidence of UTI in children under 5 years of age in Kazakhstan was 1333.7 per 100,000 children in 2017. ^ 3 ^ These infections can lead to significant complications, such as chronic kidney disease and arterial hypertension, ^ 4 ^ which incur significant financial costs for subsequent treatment. For example, treatment for UTIs is valued at USD 9.2 billion in 2022 and will rise to USD 11.9 billion by 2032. ^ 5 ^
UTIs are characterized by a high recurrence rate ^ 6 ^ and are associated with anatomical and functional abnormalities of the urinary system. ^ 7 ^ The peak of relapse occurs at the age of 2–4 years. During the first year of life, the incidence of UTI was higher in boys than in girls. After one year, the probability of developing UTI in girls increased by 10-12 times. ^ 8 ^
A study conducted at the French Medical Institute for Children in 2018 found that the dominant pathogens of urinary tract infections were Escherichia coli (63.9%), Enterococcus (11.1%), Serratia (10.8%), Staphylococcus (8.2%). ^ 9 ^ Although Staphylococcus epidermidis was previously considered a contaminant in urine tests, the literature suggests that it can cause UTIs. ^ 10 ^ Moreover, when the frequency of certain types of staphylococci changes, the proportion of S. epidermidis and Staphylococcus haemolyticus increases, which can act as pathogens, especially in the presence of local immunodeficiency. ^ 11 ^
The most common pathogen of UTI is E. coli, ^ 12 ^ among other Gram-negative bacteria are Proteus mirabilis and Proteus vulgaris. ^ 13 ^ Moreover, UTI caused by E. coli are lower in neonates. ^ 14 ^ In children with urinary tract abnormalities or a weakened immune system, S. aureus, S. epidermidis, Haemophilus influenzae, Streptococcus pneumoniae, Streptococcus viridians, and Streptococcus agalactiae are the common causes of UTI. ^ 10 ^
Studies show that treatment of UTIs is becoming increasingly difficult due to increasing antibiotic resistance among uropathogens, especially E. coli, which is associated with widespread antibiotic use (25-40%). ^ 15 ^ Resistance patterns vary by region: resistance of E. coli to co-amoxiclav increased by 13.7% in Ireland (2016-2021), ^ 16 ^ Extended–Spectrum Beta-Lactamase positive E. coli increased from 6.1% to 25.4% in Israel (2007-2021), ^ 17 ^ and increased resistance to major antibiotic classes was observed in the European Economic Area from 2013 to 2016. ^ 18 ^
The rise in antimicrobial resistance in children is a global issue requiring localized responses due to regional variability. While multicenter studies in Kazakhstan have focused on community-acquired infections across all ages, showing sensitivity data only for E. coli, ^ 19 ^ our study specifically addresses the etiological structure and resistance in pediatric UTIs, including children under 1 year, a group often overlooked in previous research, ^ 20 ^ especially in industrial regions where data remain limited.
This study aimed to investigate the microbial spectrum and resistance profile of uropathogens among patients at the Regional Children’s Clinical Hospital of Karaganda, Kazakhstan, to identify patterns of resistance to antibacterial drugs and develop recommendations for preventing the spread of resistant strains.
Materials and Methods
This study was performed in accordance with the principles of the Declaration of Helsinki (1978). The study protocol was approved by the local ethical committee of the Faculty of Natural Sciences of the L. N. Gumilyov Eurasian National University (No. 7 dated March 24, 2021). Informed consent was obtained from the parents or legal guardians.
This retrospective cohort study was conducted at the Regional Children’s Clinical Hospital of Karaganda over 6 years, from January 2017 to December 2022. Analysis was carried out on the medical records (the date of sample collection, sex and age of patients, bacterial isolates, and antibiotics prescribed) of 762 children aged 0 to 60 months. The inclusion criteria included all children born and living since birth in a given city with a diagnosis of UTI, while the exclusion criteria excluded patients with incomplete data or chronic diseases. The subjects were divided into two age groups: Group I (0-12 months) and Group II (13-60 months) on the basis of anatomical and physiological characteristics.
This study examined the clinical and laboratory characteristics of patients with positive urine cultures showing ≥10^5^ colony-forming units per milliliter (CFU/mL) using midstream or catheterized samples collected before antibiotic therapy and analyzed using the VITEK2 Compact system (BioMérieux SA, France) at the GIO TRADE laboratory (Karaganda, Kazakhstan). Antibiotic sensitivity was determined using the Kirby-Bauer test (Nutrient medium produced by the State Research Center for Applied Microbiology and Biotechnology, Russia). Antibiogram results categorized the isolates as susceptible or resistant. Standardized reference strains provided by organizations such as American Type Culture Collection (ATCC), Collection of Institute Pasteur (CIP), German Collection of Microorganisms and Cell Culture (DSM), National Collection of Type Cultures (NCTC), Culture Collection University of Gothenburg (CCUG), Spanish Type Culture Collection (CECT), and other national collections (E. coli ATCC 25922, E. coli CIP 7624, E. coli DSM 1103, E. coli NCTC 11954, E. coli CCUG 30600, E. coli CECT 943, and others) were used to calibrate and verify the performance of VITEK 2 Compact. Quality control included both internal control (checking test results using control cartridges) and external control (participation in external quality control programs, such as interlaboratory comparison programs provided by the College of American Pathologist and Clinical and Laboratory Standards Institute) to evaluate its performance. Analyses were performed by two bacteriology doctors and three laboratory assistants.
Karaganda is a large industrial center where large deposits of coal, lead, zinc, iron, manganese, and rare metals are concentrated. The city ranks 23^rd^ among the countries in the world with the most polluted air. ^ 21 ^ Karaganda is an economically developed region of Kazakhstan, with an unemployment rate of 4.2%. ^ 22 ^
Statistical Analysis
Data were collected and analyzed using Microsoft Excel 2007 (Microsoft Corporation, USA) and RStudio (Posit PBC, USA). Quantitative variables were described as mean and standard deviation using the t test and Chi square test to analyze differences and relationships at a significance level of 0.05.
Results
In total, 762 patients aged 0–60 months were hospitalized for UTI. The patients included Kazakhs (65.3%), Russians (12.3%), Ukrainians (9.4%), Jews (3.7%), Germans (3.1%), Tatars (2.5%), Koreans (1.9%), Chechens (1%), and others (Belarusians, Uzbeks, Azerbaijanis, Romanians, Georgians-0.8%). The number of isolated uropathogens was 519 (68.1%), of which 313 (60.3%) were detected in girls and 206 (39.7%) in boys with a first episode of UTI. By age, the number of isolated uropathogens was distributed as follows: 286 (55.1%) from to 0-12 months and 233 (44.9%) from to 13-60 months.
The most common pathogens were E. сoli, E. faecalis, and S. epidermidis.
With age, the role of E. coli increased, accounting for 37.1% of all uropathogens by 13-60 months, and the role of E. faecalis and S. epidermidis decreased from 18.6% to 11.3% and from 9.3% to 8.3%, respectively. Age-related increases were also observed in Pseudomonas aeruginosa (7.3 times) and P. mirabilis (4.3 times). A decrease in the incidence of Enterobacter cloacae and Enterococcus faecium, by five times and 2.3 times, respectively, was also noted. S. аureus and Staphylococcus gallinarium were mainly found in children under one year, whereas Klebsiella pneumoniae, S. viridans, and Hafnia alvei were more common in children over one year of age (table 1).
Recurrent episodes of UTI were reported in 100 patients (13%), of whom 46 (46%) were boys and 54 (54%) were girls. Thirty-three patients were in Group I, including 17 boys (51.5%) and 16 girls (48.5%). Group II consisted of 67 children, of whom 29 were boys (43.3%) and 38 were girls (56.7%).
During the relapse period, 72 isolates were identified, of which 23 (31.9%) E. coli, 16 (22.2%) were S. epidermidis, 11 (15.3%) E. faecalis, 7 (9.7%) were Candida, 3 (4.2%) were E. cloacae, 2 (2.8%) were E. аerogenes, Klebsiella oxytosa, E. faecium, and S. аureus, 1 (1.4%) was Staphylococcus saprophyticus, P. mirabilis, H. alvei, S. viridians.
Of the 762 patients, 672 (88.2%) were prescribed antibiotics. The most frequently used antibiotics are listed in table 2.
Ninety patients (11.8%) did not receive empiric antibiotic therapy and were switched to vitamin sparing therapy and special diets for UTI after receiving urine culture results. 32 children (4.7%) received antibiotics during the month preceding the actual hospitalization for UTI. A total of 398 patients (59.2%) started taking antibiotics on the day of hospitalization.
A study of sensitivity to 20 antibiotics showed a high sensitivity of uropathogens to imipenem (94.4%), ciprofloxacin (81.2%), cefepime (80.8%), and amikacin (80.4%) in children under one year of age. In the group of children older than one-year, high sensitivity was observed for doripenem (87.5%), cefepime (84.0%), ciprofloxacin (83.0%), and vancomycin (82.0%).
In both groups, high resistance was observed to amoxicillin (76.7% and 73.8%), erythromycin (73.7% and 55.5%), and ampicillin (66.7% and 66.6%), to group I and II, respectively. With age, a reduction in the number of susceptible strains to сefuroxime (72.6% and 55.4%) and imipenem (94.4% and 74.4%) was observed in group I and II, respectively. In contrast, the number of strains susceptible to gentamicin (62.1% and 77.0%), ceftazidime (56.4% and 72%), cefazolin (34.0% and 57.0%), ofloxacin (63.1% and 80.0%), vancomycin (55.5% and 82.0%), and doripenem (66.7% and 87.5%) was higher among children older than one year. Comparable levels of susceptibility and resistance were noted for amikacin, levofloxacin, ciprofloxacin, and cefepime across different age groups (table 3).
The results of studying the antibiotic sensitivity of urine strains in children from 0 to 60 months of age showed that more than half of the strains were resistant to amoxicillin, erythromycin, ampicillin, and cefazolin, while maintaining sensitivity to carbapenems (imipenem-80%, doripenem-82%, meropenem-77%), aminoglycosides (amikacin-78%, gentamicin-70%), fluoroquinolones (ciprofloxacin, levofloxacin-82%, ofloxacin-76%), nitrofurans (furazolidone-78%), and IV fourth-generation cephalosporins (cefepime-80%). However, with repeated infections, the antibiotic sensitivity of uropathogens decreased (table 4).
Analysis of the antibiograms of the dominant strains revealed that E. coli showed high sensitivity to amikacin (90%), ciprofloxacin (88.9%), and furazolidone (88%), whereas E. faecalis was sensitive to ceftriaxone (97%) and amikacin (83%), S. epidermidis showed high sensitivity to cefuroxime (88.9%) (table 5).
Of the 458 uropathogens, 157 (34%) were resistant to two or more antibiotics. Among them, E. coli showed a prevalence of multidrug-resistant strains, 22%, E. faecalis 29%, S. epidermidis 26%, S. aureus 54%, and Staphylococcus saprophyticus 58% (table 6).
The figures show the resistance profiles of UTI pathogens according to the sex (figure 1a) and age (figure 1b) of patients.
Distribution of pathogen resistance by sex (a) and age (b). (a) shows the proportion of antibiotic-resistant pathogens isolated from male and female patients. (b) illustrates the distribution of antibiotic-resistant pathogens by age groups I and II.
Interestingly, the graph shows that certain bacteria (Staphylococcus gallinarum, Citrobacter freundii, Klebsiella oxytoca, and S. viridans) were found only in girls, whereas K. pneumoniae, P. aeruginosa, and H. alvei were found only in boys, with resistance levels exceeding 50% (figure 1a). Overall, resistance was higher in girls for E. coli, E. faecalis, S. saprophyticus, S. aureus, and P. mirabilis, and higher in boys for Enterobacter aerogenes and S. epidermidis, while resistance was generally greater in the older age group, except for a few species.
Discussion
This study examined uropathogenic bacteria that cause UTIs in children, and in some cases, multidrug resistance was observed with varying levels of sensitivity to different classes of antibiotics. A total of 286 uropathogens (55,1%) were isolated from children aged under 12 months, while 233 (44,9%) were isolated from children aged 13-60 months.
The dominant species were E. coli 170 (32,7%), E. faecalis 80 (15,4%), and S. epidermidis 46 (8,9%). In children of both age groups, the leading causative agents of urinary infections are bacteria of the Enterobacteriaceae family. However, in children under one year of age, enterococci (E. faecalis 54 [18.6%], E. faecium [17 5.9%]) and staphylococci (S. epidermidis [27 9.3%], S. saprophyticus 19 [6.,5%]) also predominate, while in children over one year of age, staphylococci (S. epidermidis [19 8.3%], S. saprophyticus [17 7.4%]) and enterococci (E. faecalis 26 [11.3%], E. faecium 6 [2.6%]) predominate. Our study is similar to other studies that confirmed that the identified dominant uropathogens are opportunistic strains capable of migrating from the intestine to the urinary system, causing opportunistic infections when exposed to adverse environmental factors. ^ 23 ^ The occurrence of UTIs as a result of violation of the qualitative and quantitative composition of the host microbiome was noted by Kim and Lee. ^ 24 ^
A study of children treated at Nanjing Children’s Hospital ^ 25 ^ found that the leading etiological agent was Enterococcus spp. (35.15%), whereas in a study of children with febrile UTIs in Kawasaki, ^ 26 ^ the most common pathogen was E. coli, followed by E. faecalis, which was similar to our study. In our study, one of the dominant uropathogens was S. epidermidis, which was considered a contaminant, but is now considered a uropathogen of UTI ^ 10 ^ in conjunction with other clinical tests and functional studies. Among the admitted patients, 69 (11.8%) had congenital renal and urogenital abnormalities. To diagnose diseases of the kidneys and urinary tract, leukocyturia was defined as more than 25 leukocytes in 1 μL or more than 10 leukocytes in a field of view (FOV). Leukocytes from 4 to 15 in the FOV were observed in urine analyses in 44 patients (7.5%) and from 16 or more in 170 patients (29.1%). Continuous leukocyturia (pyuria) and turbid urine were detected in urine analyses of 132 patients (22.6%).
An increase in the resistance to various antibiotics has been observed in various countries. In the present study, the highest resistance of uropathogens was noted against amoxicillin (75%), whereas for E. coli, it was 67.6%. In several studies, it has been noted that the resistance of uropathogenic E. coli to amoxicillin depends on the region, since in European countries, resistance to amoxicillin/clavulanic acid is up to 40%. ^ 27 ^ Research reports conducted in various regions of Iran in 1992-2015 showed resistance of E. coli isolates to amoxicillin in 76% of cases. ^ 28 ^ In a study conducted among children in Bhaktapur, Nepal, 80.3% of uropathogens were resistant to amoxicillin. ^ 29 ^
A study evaluating adequate treatment with aminoglycosides suggested their use for the treatment of lower UTI. ^ 30 ^ In the present study, uropathogens were resistant to gentamicin in 30% of cases and amikacin in 22% of cases, and aminoglycosides were effective in treating relapses. Amikacin was also effective against E. coli (90%), E. faecalis (83%), and S. epidermidis (73%). Previous research has revealed high resistance to amikacin; only 3.17% of uropathogens were sensitive. ^ 25 ^ Another retrospective study from to 2014-2016 showed that strains resistant to gentamicin were associated with higher levels of cefuroxime and cefotaxime, while all isolates resistant to gentamicin were sensitive to amikacin. ^ 31 ^ In our study, a similar relationship was observed between gentamicin and cefotaxime. Patients with Gram-positive UTIs received cefazolin (71.0%) and/or gentamicin (50.8%) as empirical treatment. ^ 32 ^ In the present study, cefazolin was effective against S.epidermidis.
In the present research, resistance rates to ceftazidime, cefotaxime, cefazolin, and cefuroxime were 35.8, 42, 55%, and 34%, respectively. High resistance of uropathogens to cefuroxime (71.6%) was observed in children aged 0–18 years admitted to the Department of Pediatrics at the Hospital of the Faculty of Medicine of Harran University, Turkey. ^ 33 ^ Ten-year monitoring of the antibiotic sensitivity of the leading pathogen, E. coli, showed a high dynamic resistance to antibiotics; in 2019, the resistance was 70±4.06%. Of the 252 isolates, 135 were susceptible to cefuroxime (53.6±5.76). ^ 34 ^ In another study, 71% of E. coli isolates were resistant to cefazolin. ^ 35 ^ However, several authors note that cefazolin-resistant isolates may be sensitive to third-generation oral cephalosporins. ^ 36 ^
Our study demonstrated a low frequency of multi-resistant uropathogens (34%) in the context of international practice. However, with age, resistance increased from 23% to 43%, indicating that antibiotic susceptibility changes over time. Moreover, resistance in boys increased with age by almost two times, while in girls, it increased by 1.4 times. A antibiotic resistance study conducted in Kazakhstan showed the irrational use of antibiotics in the adult population. ^ 37 ^ The increasing antibiotic resistance in Kazakhstan may be due to the inappropriate use of antibiotics and low awareness about this issue.
The present study found that recurrent UTIs (13% of cases) are associated with reduced chances of selecting an effective antibiotic due to rising multidrug resistance, with no significant sex differences observed, while other studies reported high recurrence rates (up to 68.4%) ^ 38 ^ and mixed findings on sex influence, some showing no difference, ^ 39 ^ while others noted higher recurrence in girls under one year. ^ 40 ^
This study had several limitations. Findings on uropathogen etiology and resistance are institution-specific and may not be generalizable. The focus on dominant pathogens may underestimate the role of less common ones, and the antibiotic data from 2017 to 2022 may not reflect current treatment practices.
Conclusion
The identified dominant pathogens, such as E. coli, E. faecalis and S. epidermidis, showed high resistance to widely used antibiotics, such as amoxicillin and erythromycin. At the same time, E. coli and E. faecalis were sensitive to amikacin, while E. faecalis and S. epidermidis were sensitive to ceftriaxone. Infection was more common in girls than in boys. However, differences in the diversity of multidrug-resistant uropathogens were observed in both sexes. The study also showed a progressive increase in the prevalence of multi resistant uropathogens with age.
The results of this study highlight the importance of regular bacteriological monitoring in hospital settings, as the species spectrum of UTI pathogens and their susceptibility to antibiotics tend to change over time.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alsaywid BS Alyami FA Alqarni N Neel KF Almaddah TO Abdulhaq N Metal Urinary tract infection in children: A narrative review of clinical practice guidelines Urol Ann 20231511332[ PMC Free Article ]10.4103/ua.ua_147_2237304508 PMC 10252788 · doi ↗ · pubmed ↗
- 2Uwaezuoke S Ayuk A Muoneke U Urinary tract infection in children: A review of the established practice guidelines EMJ Microbiol Infect Dis 20201576510.33590/emjmicrobiolinfectdis/20-00001 · doi ↗
- 3Health and healthy lifestyle [Internet]. Primary Incidence among Children under the Age of 5 Years. [cited 2024 15 May].Available from: https://bala.stat.gov.kz/en/pervichnaya-zabolevaemost-detej-do-5-let/.
- 4Buettcher M Trueck J Niederer-Loher A Heininger U Agyeman P Asner Setal Correction to: Swiss consensus recommendations on urinary tract infections in children Eur J Pediatr 20211806757[ PMC Free Article ]10.1007/s 00431-020-03820-333001233 PMC 7886751 · doi ↗ · pubmed ↗
- 5Gotadki R [Internet] UTI Treatment Market Research Report Source 2025. [cited 2024 15 May].Available from: https://www.marketresearchfuture.com/reports/uti-treatment-market-3146
- 6Larcombe J Urinary tract infection in children: recurrent infections BMJ Clin Evid 20152015[ PMC Free Article ]26067232 PMC 4463760 · pubmed ↗
- 7Rodriguez MM Congenital Anomalies of the Kidney and the Urinary Tract (CAKUT) Fetal Pediatr Pathol 201433293320[ PMC Free Article ]10.3109/15513815.2014.95967825313840 PMC 4266037 · doi ↗ · pubmed ↗
- 8Leung AKC Wong AHC Leung AAM Hon KL Urinary Tract Infection in Children Recent Pat Inflamm Allergy Drug Discov 201913218[ PMC Free Article ]10.2174/1872213 X 1366618122815494030592257 PMC 6751349 · doi ↗ · pubmed ↗