Muscle Strength, Functional Capacity, and Quality of Life Responses to Pilates Exercises in Children with Burn Injuries: A Single-Blinded Randomized Clinical Trial
Alshimaa R Azab, Nourah Basalem, Mshari Alghadier, Humaira Khanam, Julie George, Saleh M. Aloraini, Feras Alsultan, Maged A. Basha, Intsar S. Waked, FatmaAlzahraa H. Kamel

TL;DR
Adding Pilates to traditional therapy improves muscle strength, function, and quality of life in children recovering from burns.
Contribution
This study is the first to show Pilates improves recovery outcomes in children with burn injuries.
Findings
Pilates group showed significantly better lower extremity muscle strength than traditional therapy alone.
Functional capacity and quality of life scores were higher in the Pilates group after 12 weeks.
No significant difference was found in the psychological subscale of quality of life between groups.
Abstract
Burns are a common childhood injury that can affect physical health for a long time, which has an impact on quality of life. This study aimed to determine whether adding Pilates exercise to a traditional physical therapy program improves lower extremity muscle strength, functional capacity, and quality of life in burned children. This single-blinded randomized clinical trial was conducted at Prince Sattam bin Abdulaziz University in Saudi Arabia from 2022 to 2023. A simple randomization method was followed in this study. The control group (n=30) received a traditional physical therapy program, while the Pilates group (n=30) received a Pilates training in addition to the traditional physical therapy program. All participants attended the intervention 3 days a week, for 12 weeks. Measurements were made at baseline and after 3 months of the intervention. The outcome measurements included…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
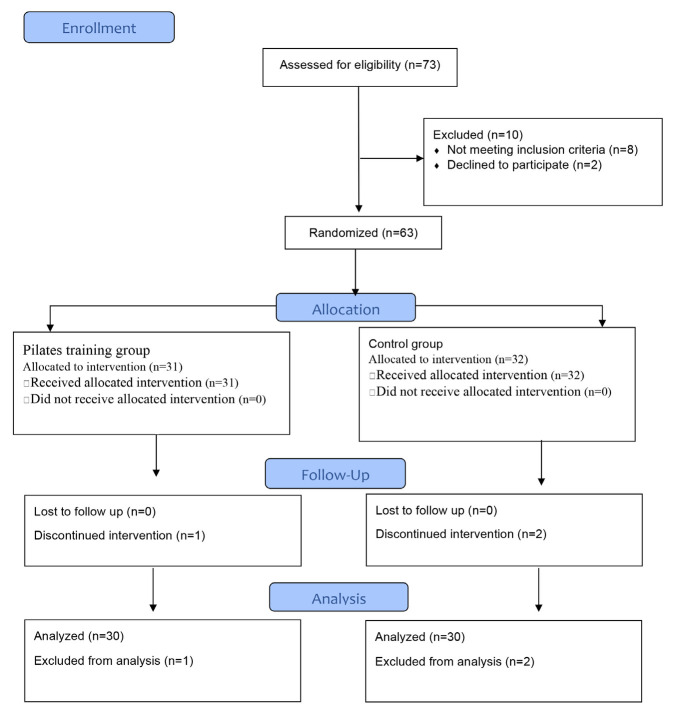 Figure 1
Figure 1| Variables | Pilates group (n=30) | Control group (n=30) | P value | |
|---|---|---|---|---|
| Age (years) | 12.30±1.73 | 12.03±1.54 | 0.53 | |
| Sex (n, %) | Male | 14 (46.7%) | 19 (63.3%) | 0.20 |
| Female | 16 (53.3%) | 11 (36.7%) | ||
| Cause of burn (n, %) | Thermal | 12 (40%) | 16 (53.3%) | 0.30 |
| Scald | 15 (50%) | 12 (40%) | ||
| Chemical | 3 (10%) | 2 (6.7%) | ||
| Height (m) | 1.49±0.09 | 1.48±0.07 | 0.71 | |
| Weight (Kg) | 41.00±9.02 | 41.87±7.66 | 0.69 | |
| BMI (Kg/cm2) | 18.24±3.37 | 18.79±2.28 | 0.46 | |
| TBSA (%) | 46.83±5.85 | 45.67±7.02 | 0.49 | |
| Hospital Stay (day) | 96.60±16.54 | 101.63±12.12 | 0.18 | |
| Outcomes | Pilates group (n=30) | Control group (n=30) | P value | |
|---|---|---|---|---|
| FC | 624.97±14.63 | 629.7±13.98 | 0.21 | |
| QoL | Physical | 70.17±11.18 | 69.83±10.21 | 0.90 |
| Psychological | 66.83±7.82 | 68.50±6.71 | 0.38 | |
| Total | 70.0±9.56 | 69.50±10.7 | 0.85 | |
| HF | Dominant | 27.05±4.39 | 26.43±4.86 | 0.60 |
| Nondominant | 25.95±3.80 | 25.29±4.71 | 0.55 | |
| HE | Dominant | 23.13±2.93 | 21.5±5.789 | 0.17 |
| Nondominant | 22.43±2.27 | 21.37±5.70 | 0.35 | |
| HAbd | Dominant | 15.53±2.63 | 14.62±2.20 | 0.16 |
| Nondominant | 14.67±1.97 | 13.89±1.97 | 0.13 | |
| HER | Dominant | 13.90±1.76 | 13.25±1.87 | 0.17 |
| Nondominant | 12.97±1.36 | 12.88±1.75 | 0.82 | |
| KF | Dominant | 14.35±3.16 | 13.75±1.42 | 0.34 |
| Nondominant | 13.28±2.58 | 12.28±1.25 | 0.06 | |
| KE | Dominant | 18.23±4.04 | 18.66±3.65 | 0.66 |
| Nondominant | 17.03±2.79 | 17.46±2.99 | 0.56 | |
| AD | Dominant | 9.39±1.45 | 9.97±1.5 | 0.13 |
| Nondominant | 10.29±2.15 | 9.44±1.45 | 0.08 | |
| AP | Dominant | 14.24±2.30 | 14.32±2.29 | 0.90 |
| Nondominant | 13.68±1.70 | 13.72±2.0 | 0.93 | |
| Outcomes | Pilates (n=30) | Control (n=30) | MD (95% CI) | P value | |
|---|---|---|---|---|---|
| FC | 648.17±23.38 | 631.43±13.06 | 16.73 (6.95,26.52) | 0.001 | |
| QoL | Physical | 82.33±12.51 | 75.50±11.17 | 6.83 (0.71, 12.96) | 0.03 |
| Psychological | 73.0±10.14 | 71.50±5.75 | 1.50 (-2.76, 5.76) | 0.48 | |
| Total | 81.67±12.06 | 74.50±10.45 | 7.17 (1.34, 13.0) | 0.02 | |
| HF | Dominant | 30.91±5.37 | 27.27±4.79 | 3.64 (1.01, 6.27) | 0.01 |
| Nondominant | 29.74±4.75 | 26.85±4.63 | 2.89 (0.47, 5.32) | 0.02 | |
| HE | Dominant | 26.59±4.19 | 22.94±6.37 | 3.65 (0.87, 6.44) | 0.01 |
| Nondominant | 26.63±3.35 | 23.54±6.39 | 3.08 (0.45, 5.72) | 0.02 | |
| HAbd | Dominant | 17.99±3.34 | 16.12±3.01 | 1.87 (0.22, 3.51) | 0.03 |
| Nondominant | 17.22±3.01 | 15.42±2.47 | 1.80 (0.38, 3.22) | 0.01 | |
| HER | Dominant | 14.95±2.38 | 13.61±1.83 | 1.34 (0.24, 2.43) | 0.02 |
| Nondominant | 14.81±1.92 | 13.61±1.83 | 1.20 (0.23, 2.17) | 0.02 | |
| KF | Dominant | 16.84±3.91 | 14.80±1.75 | 2.05 (0.48, 3.61) | 0.01 |
| Nondominant | 15.14±2.94 | 13.93±1.66 | 1.21 (-0.02, 2.45) | 0.05 | |
| KE | Dominant | 22.68±5.22 | 20.03±3.99 | 2.65 (0.25, 5.95) | 0.03 |
| Nondominant | 21.93±4.15 | 19.50±3.82 | 2.43 (0.37, 4.49) | 0.02 | |
| AD | Dominant | 12.83±2.55 | 11.03±1.53 | 1.79 (0.70, 2.88) | 0.002 |
| Nondominant | 12.04±2.28 | 10.88±1.79 | 1.16 (0.1, 2.22) | 0.03 | |
| AP | Dominant | 16.72±3.21 | 15.0±2.21 | 1.71 (0.29, 3.14) | 0.02 |
| Nondominant | 15.90±2.17 | 14.74±1.98 | 1.17 (0.09, 2.24) | 0.03 | |
| Outcomes | Pilates group (n=30) | Control group (n=30) | |||
|---|---|---|---|---|---|
| MD (95% CI) | P value | MD (95% CI) | P value | ||
| FC | -23.2 (-26.38, -20.03) | <0.001 | -1.73 (-4.91,1.44) | 0.28 | |
| QoL | Physical | -12.17 (-14.40, -9.93) | <0.001 | -5.67 (-7.90, -3.43) | <0.001 |
| Psychological | -6.17 (-7.91, -4.43) | <0.001 | -3.0 (-4.74, -1.26) | 0.001 | |
| Total | -11.67 (-13.77, -9.57) | <0.001 | -5.0 (-7.10, -2.90) | <0.001 | |
| HF | Dominant | -3.86 (-4.88, -2.85) | <0.001 | -0.85 (-1.87,0.17) | 0.10 |
| Nondominant | -3.8 (-4.70, -2.89) | <0.001 | -1.56 (-2.47, -0.66) | 0.001 | |
| HE | Dominant | -3.47 (-4.36, -2.57) | <0.001 | -1.44 (-2.34, -0.55) | 0.002 |
| Nondominant | -4.20 (-5.19, -3.21) | <0.001 | -2.18 (-3.17, -1.19) | <0.001 | |
| HAbd | Dominant | -2.46 (-3.10, -1.83) | <0.001 | -1.50 (-2.14, -0.86) | <0.001 |
| Nondominant | -2.55 (-3.17, -1.94) | <0.001 | -1.53 (-2.14, -0.92) | <0.001 | |
| HER | Dominant | -1.04 (-1.40, -0.69) | <0.001 | -0.37 (-0.72, -0.01) | 0.04 |
| Nondominant | -1.84 (-2.31, -1.38) | <0.001 | -0.73 (-1.20, -0.27) | 0.003 | |
| KF | Dominant | -2.49 (-2.98, -2.0) | <0.001 | -1.05 (-1.54, -0.56) | <0.001 |
| Nondominant | -1.87 (-2.42, -1.32) | <0.001 | -1.65 (-2.20, -1.10) | <0.001 | |
| KE | Dominant | -4.46 (-5.58, -3.34) | <0.001 | -1.37 (-2.49, -0.25) | 0.02 |
| Nondominant | -4.90 (-5.83, -3.98) | <0.001 | -2.04 (-2.96, -1.11) | <0.001 | |
| AD | Dominant | -3.44 (-4.13, -2.74) | <0.001 | -1.06 (-1.76, -0.36) | 0.004 |
| Nondominant | -1.76 (-2.27, -1.24) | <0.001 | -1.45 (-1.97, -0.93) | <0.001 | |
| AP | Dominant | -2.47 (-2.95, -1.99) | <0.001 | -0.69 (-1.17, -0.21) | 0.01 |
| Nondominant | -2.23 (-2.71, -1.74) | <0.001 | -1.02 (-1.51, -0.54) | <0.001 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurn Injury Management and Outcomes · Wound Healing and Treatments · Sports injuries and prevention
What’s Known
- Pilates does appear to improve flexibility, strength, and postural control and reduce pain in children with musculoskeletal pathology.
- Pilates has some potential for improving postural misalignment of the thoracic and lumbar angles in children and adolescents.
What’s New
- Adding Pilates exercises to a traditional physical therapy program had a positive impact on the strength of muscles in the lower limb, functional capacity, and quality of life in children with burn injury.
- Pilates exercises could be considered as part of a rehabilitation program for children who have suffered burn injuries.
Introduction
The World Health Organisation (WHO) reports that burn trauma is the fourth most common type of accidental injury, with approximately 11 million burn injuries and 180,000 deaths worldwide each year. ^ 1 ^ Burn survivors often experience long-term physical and psychological effects. Their functional level may be affected by these limitations, which may require long-term inpatient care as well as both mental and physical rehabilitation. ^ 2 ^ The number of burn-related surgeries, hospital-acquired comorbidities, and prolonged hospital stays negatively affects physical well-being and general quality of life. ^ 2 , 3 ^
Breakdown of skeletal muscle, systemic inflammation, and elevated resting energy expenditure are hallmarks of the pathophysiological response to significant burn trauma. ^ 4 , 5 ^ Skeletal muscle is the greatest protein reserve in humans and constitutes approximately 70% of total lean body mass in healthy people. Therefore, one of the main sources of amino acids for post-burn survival and regeneration is muscle protein. It is believed that the release of amino acids from skeletal muscle promotes wound healing, the synthesis of acute-phase and inflammatory proteins, and the provision of substrate for hepatic gluconeogenesis during burn recovery. ^ 4 , 5 ^ Up to two years after burn injury, this hypermetabolic and enduring catabolic reaction may continue. Consequently, the ongoing breakdown of muscles leads to a decrease in muscle mass and strength, which hinders the recovery of functional mobility. As a result, techniques that support the preservation of skeletal muscle mass and function may benefit patients in the long run as they recover from severe burns. ^ 4
- 8 ^
To lower hypermetabolism and speed up burn survivors’ social reintegration, muscle strength and aerobic capacity are crucial aspects of health that must be addressed in post-burn treatment as well as in the early post-burn rehabilitation phase. ^ 8 , 9 ^ Consequently, a successful training regimen may be necessary to improve the muscular endurance and work capacity of pediatric burn patients. Burned patients are frequently involved in a resistance and aerobic exercise program as part of their physical therapy to lessen muscle weakness and deconditioning, as well as burn-induced catabolism. ^ 9 , 10 ^
Among the numerous kinds of physical therapy exercises, Pilates is a popular form. Pilates is popular today not only for physical fitness but also for rehabilitation programs. It is a set of exercises composed of stretching, coordination, and strengthening exercises, which focus on developing stability, flexibility, muscle control, and muscle strength, especially the muscles of the trunk (core training), through the utilization of the body-mind-spirit connection. ^ 11 ^
However, there is limited data on the effects of Pilates on lower limb muscle strength, particularly in burned children. Thus, the current study sought to determine whether adding Pilates exercise to a traditional physical therapy program improves lower extremity muscle strength, functional capacity, and quality of life in children with lower limb burn.
Patients and Methods
Study Design
This investigation was a controlled, randomized clinical trial performed between June 2022 and October 2023 at the outpatient physical therapy clinic of the College of Applied Medical Science, Prince Sattam bin Abdulaziz University in Saudi Arabia. The protocol was approved by the Physical Therapy Research Ethics Committee (RHPT/023/014), and the study met the 1964 Declaration of Helsinki. The parents or legal guardians of the burned children were given a brief explanation of the study’s procedures, and they were requested to sign a consent form indicating their agreement to enroll their children in this study. This study is registered at ClinicalTrials.gov NCT06237361.
Patients
In this study, 60 children with healed burns between the ages of 10 and 15 (33 males and 27 females) participated. The inclusion criteria for the trial were children with lower limb healed burns, 6 months after injury, a total body surface area between 35–55 percentages, patients involved in the study presented with second- and third-degree burns located on the anterior and posterior thighs, anterior and posterior legs, and the foot, and the capacity to walk securely without assistance. Exclusion from the study was justified in cases of any lower limb joint range of motion limits, mental illnesses, significant behavioral or cognitive impairments, incapacity to exercise, metabolic diseases, neuropathy, visual or vestibular abnormalities, and medical instability.
Sample Size Calculation and Randomization
The sample size calculation was performed before the study commenced using G*POWER statistical software (version 3.1.9.2; Germany). The sample size was estimated based on: [F tests- multivariate analysis of variance: repeated measures, within-between interaction; Type I error(α)=0.05, power=80%, effect size=0.37]. The effect size was calculated for the quality-of-life total score from unpublished data in a pilot study with five subjects per group, where mean and standard deviation (mean±SD) were 72.25±4.45 and 70.69±3.99 for the Pilates and the control groups, respectively. The estimated sample size was calculated to be 60 participants. To accommodate potential dropouts, the sample size was increased by 5%, resulting in a final study sample size of 63 participants.
Participants were randomly allocated to the Pilates training group (which received Pilates training in addition to the traditional physical therapy program) and the control group (which received the traditional physical therapy program) after baseline assessment. Simple randomization was done by allocating patients with odd numbers into the Pilates training group and those with even numbers into the control group. To reduce allocation bias, the assignments were concealed in sequentially numbered, opaque, sealed envelopes, which were opened only after baseline assessment by an author not involved in outcome evaluation. Outcome assessments were conducted by a separate author blinded to group allocation. To ensure the assessor’s blindness, participants were requested not to discuss their intervention during follow-up.
Outcome Measures
Measurements of lower limb muscle strength, functional capacity, and quality of life were made at baseline (6 months post injury) and after the group intervention (12 weeks) by an independent researcher who was not aware of it.
Muscle Strength Assessment
Using a calibrated handheld dynamometer (Micro FET2, Hoggan Health Technologies Inc., UT, USA), the maximum voluntary isometric muscular strength of hip flexors, extensors, abductors, external rotators, flexors and extensors of the knee, as well as the ankle dorsi- and plantar flexors, was measured. All participants attended a demonstration session to become more familiar with the assessment processes. Each participant was urged to put in their best effort. Three 5-sec contractions were made for each muscle group, and the average score in kilogram-force was then calculated and used for the study. The placement of the dynamometer and the position of the child were explained in our previous research. ^ 12 ^ The handheld dynamometer provides good to excellent intra-rater reliability (ICCs ranging from 0.80 to 0.96) and inter-rater reliability (ICCs between 0.83 and 0.95). ^ 13 ^
Functional Capacity
The 6-minute walk test was used to evaluate functional capacity. It is a submaximal test that has been demonstrated to be useful and well-tolerated in burn victims. ^ 14 ^ The assessor timed the participants and gave them 6 min to walk as far as they could along a straight course. They were not allowed in any way to run, jump, or hop. The 6-min walk test reported high test-retest reliability, with an intraclass correlation coefficient (ICC) of 0.94, indicating consistent results upon repeated administrations. ^ 15 ^
Quality of Life
The Arabic version of the self-reported Pediatric Quality of Life Inventory^TM^ 4.0 generic core scale was implemented to assess health-related quality of life. The Pediatric Quality of Life Inventory was successfully validated in children who have experienced trauma and has shown excellent psychometric characteristics in children and adolescents between 2 to 18, as Cronbach’s alpha coefficients exceed 0.70 across total scores and subscales, indicating satisfactory internal consistency and high test-retest reliability, with coefficients exceeding 0.90, confirming the instrument’s stability over time. ^ 16 , 17 ^
It is a 23-item scale with four functional domains that include physical, emotional, social, and school function. Items were graded on a five-point Likert scale (0 for never, 4 for almost always). Entries are reverse-scored and linearly interpreted to a 0-100 scale, with 0=100, 1=75, 2=50, 3=25, and 4=0. Domain-specific scores are then calculated as follows: 1) Physical health the sum of the items over the number of answers in the physical function subscale; 2) Psychosocial health=the sum of the items over the number of answers in the emotional, social, and school function subscales; and 3) Total score=the sum of all the items over the number of answers on all subscales. Higher scores indicate improved health-related quality of life. ^ 17 ^
Intervention
Traditional Physical Therapy Program: All participants in each group completed the traditional physical therapy program, which lasted one hour per day, three days a week, for a period of twelve weeks. Range of motion exercises, aerobic exercise, resistance exercises, scar management, occupational therapy, and hand therapy are all part of the traditional physical therapy program. Scar care was accomplished using scar massage and garments. The aerobic training consisted of walking, running, jogging, biking, and swimming, while resistance exercises included eight upper and lower body exercises such as leg press, leg curl, leg squats (with or without weights), toe raises, shoulder press, bench press, and biceps and triceps curl. ^ 18 , 19 ^
Pilates Training Program: For 12 weeks, subjects assigned to the Pilates training group completed three sessions weekly of Pilates routines. The exercises were done in three sets of eight repetitions for the first 2 weeks, three sets of 10 repetitions for the next 5 weeks, and three sets of 15 repetitions for the following weeks.
Each training session consisted of three parts: the warm-up exercises (10 repetitions of lateral neck flexion, shoulder elevation, flexion and rotation, body rotation and lateral flexion, flexion of the knees, dorsal flexion of the ankle, and mini squats). After the warm-up activities, Pilates routines were performed. Following the Pilates exercises, cool-down activities included breathing, stretching (shoulder and pectoral muscles, gastrocnemius-soleus, hip flexors and rotators, back muscles), and relaxation techniques. The subjects had spent the previous week becoming acquainted with the correct implementation of the motions as well as the concepts of the Pilates approach. ^ 20 , 21 ^ The Pilates exercise is detailed in Appendix 1.
Statistical Analysis
The measured variables were statistically analyzed and compared using the Statistical Package for the Social Sciences programme for Windows version 25 (IBM, SPSS, Inc., Chicago, IL) with a level of significance set at 0.05. Data were screened for normality assumption, homogeneity of variance, and presence of extreme scores. To test the homogeneity of variances between the groups, Levene’s test was used. The Shapiro-Wilk test for normality showed that the measured variables were normally distributed (P>0.5). Data were expressed as means and standard deviations for all outcomes except for gender and cause of burn (counts/percentages). Considering the data were normally distributed, parametric tests were employed for summarizing and analyzing age, height, weight, body mass index, total body surface area, hospital stay, muscle strength, functional capacity, and quality of life scores. The univariate analysis of variance with Bonferroni correction was performed for each outcome measure to protect against type I error.
Results
The CONSORT flow diagram displays participant enrolment, the randomization process, and retention throughout the study (figure 1). Seventy-three participants were evaluated for eligibility, and 63 participants met the inclusion criteria and were then randomly assigned to the control (n=32) or pilates (n=31) groups. Three of the participants [two in the control group and one in the study group] did not finish the study because they either relocated or had schedule conflicts, and the results they provided were not utilized in the statistical analysis. For the final analysis, data were provided for 60 patients: 30 from the control group (n=30) and 30 from the Pilates group (n=30). As shown in table 1, there were no statistically significant differences between the Pilates group and control group, respectively; as: age was (12.30±1.73 years vs. 12.03±1.54 years; P=0.53), height (1.49±0.09 vs. 1.48±0.07 m; P=0.71), weight (41.00±9.02 vs. 41.87±7.66 Kg; P=0.69), body mass index (18.24±3.37 vs. 18.79±2.28 Kg/m^2^; P=0.46), total body surface area (46.83±5.85 vs. 45.67±7.02%; P=0.49), and hospital stay (96.60±16.54 vs. 101.63±12.12 days; P=0.18).
The figure represents the CONSORT flow diagram of the study.
Baseline clinical outcome measures are demonstrated in table 2. Functional capacity was similar between groups at baseline: 624.97±14.63 meters (Pilates) vs. 629.7±13.98 meters (Control), with no significant difference (P=0.21). Likewise, baseline outcome measures for physical, psychological, and total quality of life, and muscle strength measures across ankle, knee, and hip joints show no statistically significant difference between the Pilates and control groups.
Between-Groups Effects
Table 3 shows the differences between the Pilates and the control groups after 3 months of intervention. The Pilates group showed statistically significant differences in functional capacity (648.17±23.38) compared to the control group (631.43±13.06), with a mean difference (MD) of 16.73 and a 95% confidence interval (CI) of 6.95 to 26.52 (P=0.001). Regarding to physical subscale of quality of life, there were statistically significant differences in the Pilates group (82.33±12.51) than in the control group (75.50±11.17), with an MD of 6.83 (95% CI: 0.71 to 12.96; P=0.03). Similarly, the total quality of life score has statistically significant differences in the Pilates group (81.67±12.06) over the control (74.50±10.45) with an MD of 7.17 (95% CI=1.34-13.0; P=0.02). However, no statistically significant difference was observed for the psychological subscale (MD=1.50; 95% CI=-2.76-5.76; P=0.48).
Moreover, there were statistically significant differences in muscle strength in favour for Pilates group for example: hip flexors (dominant side): Pilates (30.91±5.37) vs. Control (27.27±4.79); MD=3.64 (95% CI: 1.01 to 6.27; P=0.01), Knee extensors (non-dominant side): Pilates (21.93±4.15) vs. Control (19.50±3.82); MD=2.43 (95% CI: 0.37 to 4.49; P=0.02) and Ankle dorsiflexors (dominant side): Pilates (12.83±2.55) vs. Control (11.03±1.53); MD=1.79 (95% CI: 0.70 to 2.88; P=0.002). However, no statistically significant difference was found between groups in the non-dominant side of muscle strength of knee flexors, Pilates (15.14±2.94) vs. Control (13.93±1.66); MD=1.21 (95% CI=-0.02, 2.45; P=0.05).
Moreover, statistically significant differences between groups (favoring the Pilates group) were found in other ankle, knee, and hip muscle strength measures, as detailed in table 3.
Within-Groups Effects
In the Pilates groups, there were statistically significant differences after 3 months of intervention between the pre- and post-intervention in all measures, as shown in table 4. For example, functional capacity: MD=-23.2 meters, 95% CI [-26.38, -20.03], P<0.001, physical quality of life score: MD=-12.17, 95% CI [-14.40, -9.93], P<0.001, psychological quality of life score: MD=-6.17, 95% CI [-7.91, -4.43], P<0.001 and quality of life total score: MD=-11.67, 95% CI [-13.77, -9.57], P<0.001.
In the control groups, there was no statistically significant improvement in functional capacity: MD=-1.73 meters, 95% CI [-4.91,1.44], P=0.28, and hip flexors (dominant side) MD=-0.85, 95% CI [-1.87,0.17], P=0.10 after 3 months of intervention between the pre- and post-intervention. However, there were statistically significant improvements in quality of life (P<0.001), and muscle strength of hip flexor (nondominant), extensors, abductors, and external rotators for both dominant and non-dominant limbs after 3 months of intervention between the pre- and post-intervention. In addition, there were statistically significant improvements in muscle strength of knee flexors and extensors as well as ankle dorsiflexors and plantar flexors for both dominant and non-dominant limbs after 3 months of intervention between the pre- and post-intervention, as shown in table 4.
The Pilates group’s median treatment adherence was 93.75% (interquartile ranges: 87.50%-98.95%), whereas the control group was 95.83% (interquartile ranges: 91.67%-100%); there was no significant difference between groups (P=0.26).
Discussion
The current study provides support related to the use of Pilates exercises in combination with a traditional physical therapy program in improving the muscle strength, functional capacity, and quality of life in burned children. The results showed that Pilates training is likely an effective adjuvant therapy that can improve the lower limb muscle strength, along with the traditional program, which has been evidenced by the more increase in “hip flexors, hip extensors, hip abductors, hip external rotators, knee flexors, knee extensors, ankle dorsiflexors, ankle planter flexors,” in Pilates group as compared with the control group. Moreover, the Pilates training designed in this study resulted in more improvement in functional capacity, physical component of daily life, and total quality of life. However, there was no improvement in the quality of life psychosocial component.
The muscle strength findings in this study are consistent with those reported by Azab and others, ^ 20 ^ who found significant improvements in hip abductor, external rotator, and knee extensor strength, functional performance, and quality of life in patients with patellofemoral pain syndrome after incorporating Pilates exercises into a conventional rehabilitation program, as well as enhanced muscle strength and postural control in children with Down syndrome. ^ 12 ^ Similarly, Güngör and others ^ 21 ^ reported that Pilates workouts substantially improved lower extremity muscular strength and postural sway in persons with multiple sclerosis. Furthermore, Bertoli and colleagues ^ 22 ^ found that mat Pilates exercises improved numerous isokinetic torque parameters in elderly women, including knee and hip flexors and extensors. This study’s findings are in line with previous research on patients with lower limb burns, which has found significant increases in knee flexor and extensor strength, balance, and functional status. ^ 23 ^
Multiple pathways contribute to the Pilates approach’s beneficial effects. Pilates is an exercise regimen that improves lower limb strength, core stability, flexibility, and coordination by combining strengthening, stretching, and core-focused exercises. By lowering stress and enhancing focus, it also enhances mental health and improves posture, balance, and general physical fitness. ^ 24 ^ Pilates uses isometric, eccentric, and concentric muscle contractions to create synergistic movement patterns that are directly transferable to functional activities. ^ 25 ^ Furthermore, body weight is used as resistance in Pilates mat movements, which improves functional performance, balance, and muscle strength. ^ 26 ^
According to the 6-min walk test, Pilates exercises improved functional capacity, which is consistent with earlier studies. ^ 27
- 30 ^ This is consistent with the findings of Alvarenga’s ^ 27 ^ study, which found that inspiratory muscle training linked with the Pilates method improves lung function and physical conditioning in the elderly. Rayes and colleagues ^ 30 ^ discovered that Pilates can be used as an alternative physical training approach for overweight or obese people, since it causes considerable improvements in cardiorespiratory fitness. Furthermore, Azab and others ^ 31 ^ found that incorporating Pilates exercises into conventional physical therapy is more likely to improve cardiorespiratory fitness, functional ability, and quality of life in children with polyarticular juvenile idiopathic arthritis than conventional physical therapy alone.
Strengthening the lumbopelvic area, increasing ribcage flexibility, and breathing exercises are three potential sources of improvement that may explain the positive impact of Pilates intervention on aerobic capacity. First, Pilates-induced lumbopelvic and core muscular strengthening may result in a more effective motion pattern in the upper and lower limbs, as well as better strength in the expiratory muscles. ^ 27 , 28 ^
Second, when flexibility improves, a more efficient ribcage motion pattern may be established. ^ 29 ^ Lastly, the respiration strategies used during Pilates activity may improve lung capacity and intercostal muscle performance. ^ 30 ^ Increased ventilation performance would be obtained on these grounds, resulting in a larger flow of oxygenated blood into muscle tissues, increased local circulation, ^ 27
- 29 ^ muscle oxidative capacity, ^ 30 ^ and less energy waste. As a result, Pilates could achieve the bare minimum intensity required to develop functional ability. ^ 32 ^
In this study, Pilates exercises improved physical functioning and the overall quality of life. This is consistent with the findings of de Oliveira and colleagues ^ 26 ^ who discovered that the Pilates program considerably improved older individuals’ functional capacity and aspects of their health-related quality of life. Similarly, the study on practitioners yielded higher outcomes in the domains of physical function, general health, and mental health in terms of quality of life. ^ 33 ^ In addition, Vancini and others revealed that Pilates and walking positively impact quality of life, depression, and anxiety; and the Pilates approach could be utilized as an option to alleviate mood problems in overweight/obese adults. ^ 34 ^
Only physical function scores and total quality of life ratings increased with exercise in this trial. The psychological impact of burn injuries may explain the lack of recovery in psychological scores. ^ 3 , 6 ^ Psychological assistance is equally important as rehabilitation in achieving psychological improvement, and advanced research should be conducted in this area.
Furthermore, Pilates improves kinaesthetic awareness, trunk muscle strength, core stability, and the capacity to rectify maladaptive movement patterns, all of which enhance limb motor coordination and, in turn, overall motor control and performance. ^ 25 , 35 ^ Additionally, it improves the sensitivity and proprioception of mechanoreceptors surrounding the knee joint, resulting in increased joint awareness, better movement control, restored normal position sense, and improved muscle contraction. ^ 36 ^
A few limitations should be addressed. The current investigation demonstrated the methodological difficulties associated with the subjective concepts. Because of the nature of the therapy technique, it was not possible to blind the participants to the intervention; hence, this effect cannot be ruled out. Furthermore, the current investigation was limited to youth aged 10 to 15 years. As a result, our findings cannot be applied to all child populations. Only short-term consequences have been investigated; there was no follow-up with the participants, as a result, it was unclear if the gains in lower limb muscular strength and functional capacity from this period of training would continue after our intervention ended. More research should be done on the mid- and long-term impacts. We also noticed that the benefits could be attributed to the combined therapy impact, so future research should control for overall intervention duration to isolate the unique effects of Pilates.
Conclusion
Children with burn injuries who participated in the Pilates program in addition to traditional physical therapy showed greater improvements in lower limb muscular strength, functional ability, and quality of life than those who received only the traditional physical therapy program. Pilates exercises could be considered as part of a rehabilitation program for children who have suffered burn injuries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organization WH [Internet]. Burns. Genova: WHO; c 2023 Available from: https://www.who.int/news-room/fact-sheets/detail/burns#:~:text=The%20problem,and%20South-East%20Asia%20Regions
- 2Nassar JY Al Qurashi AA Albalawi IA Nukaly HY Halawani IR Abumelha A Fetal Pediatric Burns: A Systematic Review and Meta-Analysis on Epidemiology, Gender Distribution, Risk Factors, Management, and Outcomes in Emergency Departments Cureus 202315 e 49012[ PMC Free Article ]10.7759/cureus.4901238111412 PMC 10726077 · doi ↗ · pubmed ↗
- 3Mc Aleavey AA Wyka K Peskin M Difede J Physical, functional, and psychosocial recovery from burn injury are related and their relationship changes over time: A Burn Model System study Burns 201844793910.1016/j.burns.2017.12.01129395409 · doi ↗ · pubmed ↗
- 4Stanojcic M Abdullahi A Rehou S Parousis A Jeschke MG Pathophysiological Response to Burn Injury in Adults Ann Surg 201826757684[ PMC Free Article ]10.1097/SLA.000000000000209729408836 PMC 8966302 · doi ↗ · pubmed ↗
- 5Ogunbileje JO Porter C Herndon DN Chao T Abdelrahman DR Papadimitriou Aetal Hypermetabolism and hypercatabolism of skeletal muscle accompany mitochondrial stress following severe burn trauma Am J Physiol Endocrinol Metab 2016311 E 43648[ PMC Free Article ]10.1152/ajpendo.00535.201527382037 PMC 5005969 · doi ↗ · pubmed ↗
- 6Cimino SR Rios JN Godleski M Hitzig SL A Scoping Review on the Long-Term Outcomes in Persons with Adult-Acquired Burn Injuries J Burn Care Res 20204147250210.1093/jbcr/irz 14631504597 · doi ↗ · pubmed ↗
- 7Polychronopoulou E Herndon DN Porter C The Long-Term Impact of Severe Burn Trauma on Musculoskeletal Health J Burn Care Res 20183986980[ PMC Free Article ]10.1093/jbcr/iry 03530010999 PMC 6198740 · doi ↗ · pubmed ↗
- 8Cambiaso-Daniel J Rivas E Carson JS Hundeshagen G Nunez Lopez O Glover S Qetal Cardiorespiratory Capacity and Strength Remain Attenuated in Children with Severe Burn Injuries at Over 3 Years Postburn J Pediatr 20181921528[ PMC Free Article ]10.1016/j.jpeds.2017.09.01529246338 PMC 5739078 · doi ↗ · pubmed ↗