Three-Year Outcomes of iStent Inject W Implantation Combined With Phacoemulsification in Japanese Eyes With Open-Angle Glaucoma: A Retrospective Study
Takahiro Usami, Takahiro Matsuoka, Masami Yamashita, Ryosuke Yamada, Ayano Tanaka, Hiroki Kaneko

TL;DR
This study shows that combining iStent inject W with cataract surgery effectively lowers eye pressure and reduces medication use in Japanese patients with glaucoma over three years.
Contribution
Provides three-year clinical data on iStent inject W in Japanese patients with normal-tension glaucoma, a population with limited prior long-term outcomes.
Findings
Intraocular pressure decreased by 24% at 36 months post-surgery.
83% of patients achieved at least a 20% reduction in eye pressure or were medication-free.
No additional glaucoma surgeries were needed, with minimal complications observed.
Abstract
Background Glaucoma is a leading cause of irreversible blindness. In Japan, most primary open-angle glaucoma (POAG) cases are normal-tension glaucoma (NTG). Micro-invasive glaucoma surgery (MIGS) such as the iStent inject W (Glaukos Corporation, San Clemente, CA) offers a less invasive option, but long-term outcomes in NTG-predominant populations are scarce. Objective The objective of this study is to evaluate three-year outcomes of combined phacoemulsification and iStent inject W implantation in Japanese eyes with POAG. Methods This retrospective study included 24 eyes from 14 Japanese patients undergoing combined surgery between February 2021 and May 2022 at Chutoen General Medical Center. Eyes with prior glaucoma surgery (except laser trabeculoplasty) or secondary glaucoma were excluded. Intraocular pressure (IOP) and medication scores were recorded up to 36 months…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
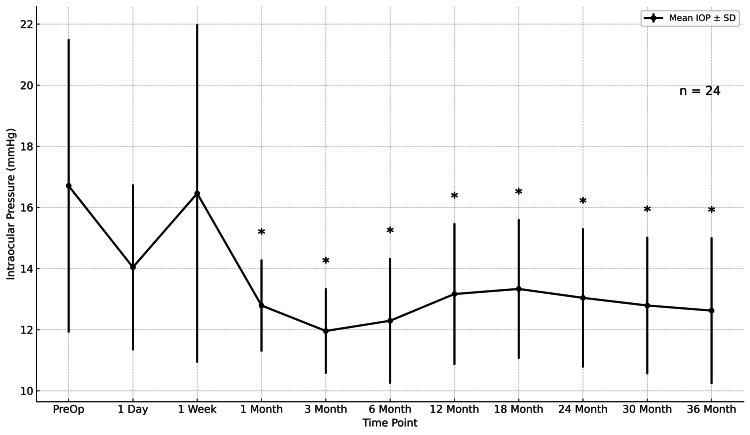 Figure 1
Figure 1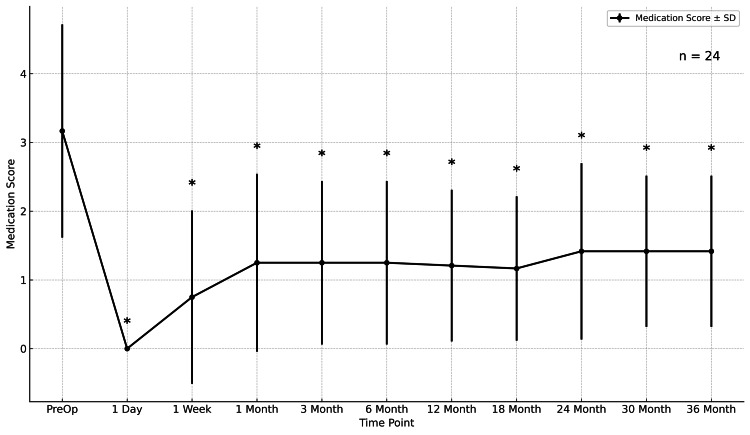 Figure 2
Figure 2| Characteristics | Value |
| Age (years), mean ± SD | 67.6 ± 9.7 |
| Gender, n (%) | |
| Male | 8 (57.1%) |
| Female | 6 (42.9%) |
| Race, n (%) | |
| Japanese | 14 (100%) |
| Laterality, n (%) | |
| OD | 13 (54.2%) |
| OS | 11 (45.8%) |
| Type of glaucoma, n (%) | |
| POAG | 11 (45.8%) |
| NTG | 13 (54.2%) |
| VFMD (dB), mean ± SD | -11.82 ± 7.59 |
| Axial length (mm), mean ± SD | 25.56 ± 1.30 |
| Outcome | Preoperative | 36 Months | Change (95% CI) | p-value | Effect size | Notes |
| IOP (mmHg), mean ± SD | 16.71 ± 4.54 | 12.63 ± 2.59 | -4.08 (-5.76 to -2.40) | <0.001 | r = 0.986 | Wilcoxon signed-rank |
| Medication score, mean ± SD | 3.17 ± 1.55 | 1.42 ± 1.10 | -1.75 (-2.15 to -1.35) | <0.001 | r = 0.967 | Wilcoxon signed-rank |
| VFMD (dB), mean ± SD | -11.82 ± 7.76 | -11.58 ± 8.75 | -0.81 (-2.21 to 0.59) | 0.483 | r = 0.15 | Wilcoxon signed-rank(paired n = 22) |
| Medication-free eyes, n (%) | - | 8 (33.3%) | - | - | - | 8/24 eyes |
| Eyes with ≥20% IOP reduction, n (%) | - | 14 (58.3%) | - | - | - | 14/24 eyes |
| Eyes with IOP increase, n (%) | - | 1 (4.2%) | - | - | - | Vs preoperative |
| Additional glaucoma surgery, n (%) | - | - | - | - | - | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlaucoma and retinal disorders · Ocular Surface and Contact Lens · Retinal Diseases and Treatments
Introduction
Glaucoma is a leading cause of irreversible blindness worldwide, with more than 70 million affected individuals, and its prevalence is projected to rise substantially as populations age [1,2]. In Japan, the Tajimi Study revealed that the majority of primary open-angle glaucoma (POAG) cases are normal-tension glaucoma (NTG), highlighting an epidemiological profile distinct from Western countries [3].
Randomized controlled trials, including the Early Manifest Glaucoma Trial, the Ocular Hypertension Treatment Study, and the Collaborative Normal-Tension Glaucoma Study, have established that lowering intraocular pressure (IOP) reduces the risk of disease progression, even in NTG patients [4-7]. However, achieving meaningful IOP reduction in NTG often requires long-term topical therapy or filtering surgery. Medical therapy is limited by adherence issues, ocular surface disease, and systemic side effects, while filtering surgery carries risks of hypotony, infection, and vision-threatening complications [8].
Micro-invasive glaucoma surgery (MIGS) has emerged as a less invasive option to improve aqueous outflow while maintaining a favorable safety profile [9]. Among MIGS devices, the iStent inject W (Glaukos Corporation, San Clemente, CA) places two trabecular micro-bypass stents into Schlemm’s canal to enhance conventional outflow. Previous studies have reported promising results, with sustained IOP and medication reduction after implantation combined with phacoemulsification [10-12]. However, many reports come from Western populations with predominantly high-tension glaucoma, and evidence in Asian populations, where NTG predominates, remains limited.
Therefore, the purpose of this study was to evaluate the three-year outcomes of combined phacoemulsification and iStent inject W implantation in Japanese eyes with POAG. We aimed to assess long-term changes in IOP, medication burden, and safety profile in a cohort characterized by advanced disease and a high prevalence of NTG.
Materials and methods
Study design and participants
This retrospective observational study was conducted at Chutoen General Medical Center, Shizuoka, Japan. Consecutive patients who underwent combined iStent inject W implantation and phacoemulsification with intraocular lens implantation between February 2021 and May 2022 were screened. Inclusion criteria were (1) diagnosis of open-angle glaucoma (including POAG and NTG) and (2) follow-up of at least 36 months after surgery at our institution. Eyes with prior glaucoma surgery other than laser trabeculoplasty, secondary glaucoma, or incomplete follow-up data were excluded.
Diagnostic definitions
Diagnostic definitions followed the Japan Glaucoma Society Fifth Edition guidelines [9]. POAG was defined as open anterior chamber angles without secondary causes, together with glaucomatous optic neuropathy and corresponding visual-field loss on standard automated perimetry, accompanied by a documented, untreated IOP >21 mmHg at diagnosis or in historical records. NTG was defined by the same structural and functional criteria as untreated IOP, consistently ≤21 mmHg on repeated measurements (preferably including diurnal testing). For analytic consistency, eyes without a documented untreated IOP profile were conservatively classified as POAG.
Data collection and outcome measures
Baseline demographic and clinical data, including age, sex, glaucoma type, axial length, and baseline visual field mean deviation (VFMD), were obtained from medical records. The primary outcomes were changes in IOP, glaucoma medication score, and VFMD from baseline to each follow-up time point. IOP and medication score were recorded at baseline (preoperative) and at one day, one week, one, three, six, 12, 18, 24, 30, and 36 months postoperatively. VFMD was recorded at baseline (preoperative) and 12, 24, and 36 months postoperatively. The medication score was calculated by assigning one point per single-agent medication and two points for a fixed-combination drug. Medication tapering and reintroduction were at the surgeon's discretion based on individualized target IOP, ocular surface tolerance, and postoperative course.
Measurements
IOP was measured using Goldmann applanation tonometry (GAT) (Haag-Streit AG, Köniz, Switzerland). When reliable GAT was not feasible due to strong eyelid squeezing/blepharospasm, rebound tonometry (iCare, Icare Finland Oy, Vantaa, Finland) was used. For each eye, the same measurement modality (GAT or iCare) was maintained across all follow-up visits. No correction for central corneal thickness was applied. Readings were obtained during routine clinic hours, and the exact time of day was not standardized, which may introduce diurnal variation, particularly in NTG-predominant cohorts.
Visual fields were assessed with Humphrey Field Analyzer 3 (HFA3; Carl Zeiss Meditec, Jena, Germany) using the 30-2 program and SITA-Standard strategy. Only examinations deemed reliable per institutional criteria were included; VFMD was taken as the instrument-reported mean deviation.
Axial length was measured with IOLMaster 700 (Carl Zeiss Meditec, Jena, Germany) under dilated conditions; values were recorded according to the device’s automated averaging protocol.
Surgical procedure
All surgeries were performed by experienced glaucoma surgeons under topical anesthesia. Phacoemulsification (through a 2.4-mm temporal clear corneal incision) and IOL implantation were carried out first, followed by insertion of two iStent inject W devices into the nasal trabecular meshwork under gonioscopic view.
Safety definitions (intraoperative adverse events)
For this study, intraoperative adverse events were predefined as follows.
Stent-related: (1) inability to implant both iStent inject W devices as planned, (2) stent dislocation, (3) device occlusion by tissue or blood, and (4) iris injury attributable to device insertion.
Cataract-related: (1) posterior capsule rupture, (2) zonular weakness or dialysis, and (3) vitreous prolapse/loss.
Statistical analysis
Continuous variables are summarized as mean ± standard deviation (SD), and changes are presented as mean differences with 95% confidence intervals (CIs) for interpretability. Statistical significance was tested using the Wilcoxon signed-rank test. The effect size r was calculated as Z/√N (paired observations). Multiplicity arising from repeated time-point comparisons was treated as exploratory and unadjusted. Proportions are reported with Wilson 95% CIs. A two-sided p < 0.05 was considered statistically significant. Analyses were conducted using standard statistical software.
Ethical approval
This study was approved by the Institutional Review Board of Chutoen General Medical Center, Shizuoka, Japan (approval no. 1306250512). The study adhered to the tenets of the Declaration of Helsinki. Given the retrospective design, written informed consent was waived, and an opt-out process was adopted through institutional website disclosure.
Results
Patient characteristics
A total of 24 eyes from 14 patients (eight men, six women) were included in the analysis. The mean age was 67.6 ± 9.7 years. All patients were Japanese. Out of 24 eyes, 13 eyes (54.2%) had NTG, and 11 eyes (45.8%) had POAG. The mean baseline VFMD was -11.82 ± 7.59 dB, and the mean axial length was 25.56 ± 1.30 mm (Table 1).
Intraoperative safety
No intraoperative adverse events occurred among the predefined categories: there were no instances of inability to implant both stents, stent dislocation, device occlusion by tissue/blood, or iris injury, and no posterior capsule rupture, zonular weakness/dialysis, or vitreous prolapse/loss.
Intraocular pressure
Mean IOP decreased from 16.71 ± 4.54 mmHg preoperatively to 12.63 ± 2.59 mmHg at 36 months (p < 0.001), representing a mean reduction of -4.08 mmHg (95% CI, -5.76 to -2.40). The IOP reduction was statistically significant at all postoperative time points compared with baseline (Figure 1).
*Mean IOPMean IOP over 36 months. Values are mean ± 95% CI; n = 24. p < 0.05 vs baseline (Wilcoxon signed-rank). IOP = intraocular pressure; CI = confidence interval.
Medication score
The mean glaucoma medication score decreased from 3.17 ± 1.55 preoperatively to 1.42 ± 1.10 at 36 months (p < 0.001), corresponding to a mean reduction of -1.75 (95% CI, -2.15 to -1.35). Significant reductions were observed at all follow-up visits (Figure 2).
*Medication scoreMean medication score over 36 months. Values are mean ± 95% CI; n = 24. Medication score assigns one point per single-agent medication and two points per fixed-combination medication.p < 0.05 vs baseline (Wilcoxon signed-rank). CI = confidence interval.
Visual field mean deviation
VFMD remained generally stable through 36 months. Mean ± SD VFMD was -11.82 ± 7.76 dB preoperatively (n = 24), -11.74 ± 8.56 dB at 12 months (n = 20), -12.23 ± 6.97 dB at 24 months (n = 15), and -11.58 ± 8.75 dB at 36 months (n = 22). In paired analyses vs baseline, the median change was +0.72 dB at 12 months (n = 20; Wilcoxon p = 0.2455), +0.08 dB at 24 months (n = 15; p = 0.9341), and +0.09 dB at 36 months (n = 22; p = 0.4826).
Main outcomes at 36 months
At the final follow-up, out of 24 eyes, eight eyes (33.3%) were medication-free, 14 eyes (58.3%) achieved ≥20% IOP reduction from baseline, and only one eye (4.2%) experienced an increase in IOP compared to preoperative levels. No eyes required additional glaucoma surgery during the follow-up period (Table 2).
Postoperative complications
No eyes required reoperation for glaucoma during the 36-month follow-up. Postoperative hyphema with niveau formation was observed in two (8.3%) out of 24 eyes. Elevated IOP ≥30 mmHg occurred in 0 eyes (0.0%) on postoperative day 1, in two eyes (8.3%) at postoperative week 1, and in 0 eyes (0.0%) at postoperative month 1.
Discussion
In the present study, combined phacoemulsification and iStent inject W implantation resulted in significant and sustained reductions in both IOP and medication burden over a 36-month follow-up period. Mean IOP decreased by over 4 mmHg (-24%) from baseline, and nearly 60% of eyes achieved ≥20% reduction. Furthermore, 13 eyes were medication-free at three years, despite a high baseline medication score of 3.2. No eyes required additional glaucoma surgery, underscoring the safety and durability of the procedure.
A notable observation at 36 months was that one eye (4.2%) showed a higher IOP than baseline, with an absolute change of +1 mmHg (14 to 15 mmHg), while its medication score decreased from 4 to 1. This pattern suggests that the modest IOP rise was more likely attributable to de-escalation of topical therapy rather than surgical failure. The increase was clinically mild and manageable by re-introducing or adjusting medications; no additional glaucoma surgery was required. Potential mechanisms include peri-stent fibrosis or stent obstruction [13] and segmental variability of distal outflow involving collector channels [14], as well as non-IOP-dependent processes relevant to NTG pathophysiology [15].
Our results compare favorably with previous reports. Salimi et al. demonstrated a 22% IOP reduction at 36 months in a single-center cohort from Canada [10]. Clement et al. reported significant short-term efficacy at 12 months in Australian patients [11]. A prospective seven-year cohort of iStent inject further supports long-term durability, reporting approximately 34-44% IOP and 58-76% medication reductions, no filtering surgeries over seven years, and clinically significant VFMD progression (≥2.5 dB) in 4.84%, albeit in a higher-IOP, predominantly non-Hispanic White population [16]. Importantly, Ang et al. recently reported outcomes specifically in Asian patients with NTG, showing modest IOP reduction but a marked decrease in medication burden, with over 80% of eyes medication-free at 12 months [12]. Despite including eyes with more advanced glaucoma (mean VFMD -11.8 dB in our study vs approximately -5 to -6 dB in other reports), our outcomes were comparable or better in terms of both IOP and medication reduction. Taken together with the findings of Ang et al. [12], our study reinforces the growing evidence that iStent inject W can provide meaningful long-term benefit even in NTG-predominant Asian populations, underscoring its clinical value in Japan, where NTG is the most common form of open-angle glaucoma.
The strengths of this study include its relatively long follow-up period, detailed outcome measures, and the focus on a Japanese cohort with advanced glaucoma and NTG predominance. These factors provide new insights into the applicability of iStent inject W in Asian populations. However, limitations include the retrospective, small, uncontrolled design, which limits generalizability. Because no standardized protocol governed postoperative medication tapering/re-initiation, decisions were made at the surgeon’s discretion, introducing management heterogeneity. Given the small cohort and few failure events, baseline-IOP-stratified analyses, modeling of within-patient correlation (when both eyes were included), and Kaplan-Meier survival analysis were not performed or would have been underpowered. Untreated IOP was unavailable for all eyes, so misclassification at the NTG/POAG boundary cannot be excluded. Larger multicenter prospective studies are needed to confirm long-term effectiveness in NTG-dominant populations.
Conclusions
In conclusion, this study demonstrates that combined phacoemulsification and iStent inject W implantation provides sustained reductions in IOP and medication burden over three years in Japanese eyes with open-angle glaucoma. Despite including more advanced cases with higher medication requirements than most prior reports, outcomes were favorable and comparable to international studies. These findings suggest that MIGS can be a safe and effective treatment option even in populations characterized by advanced disease and a high prevalence of NTG.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The number of people with glaucoma worldwide in 2010 and 2020 Br J Ophthalmol Quigley HA Broman AT 2622679020061648894010.1136/bjo.2005.081224 PMC 1856963 · doi ↗ · pubmed ↗
- 2Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis Ophthalmology Tham YC Li X Wong TY Quigley HA Aung T Cheng CY 2081209012120142497481510.1016/j.ophtha.2014.05.013 · doi ↗ · pubmed ↗
- 3The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study Ophthalmology Iwase A Suzuki Y Araie M 1641164811120041535031610.1016/j.ophtha.2004.03.029 · doi ↗ · pubmed ↗
- 4Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial Arch Ophthalmol Heijl A Leske MC Bengtsson B Hyman L Bengtsson B Hussein M 1268127912020021236590410.1001/archopht.120.10.1268 · doi ↗ · pubmed ↗
- 5The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma Arch Ophthalmol Kass MA Heuer DK Higginbotham EJ 70171312020021204957410.1001/archopht.120.6.701 · doi ↗ · pubmed ↗
- 6Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures Am J Ophthalmol Collaborative Normal-Tension Glaucoma Study Group 4874971261998978009310.1016/s 0002-9394(98)00223-2 · doi ↗ · pubmed ↗
- 7The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration Am J Ophthalmol The AGIS Investigators 42944013020001102441510.1016/s 0002-9394(00)00538-9 · doi ↗ · pubmed ↗
- 8The pathophysiology and treatment of glaucoma: a review JAMA Weinreb RN Aung T Medeiros FA 1901191131120142482564510.1001/jama.2014.3192 PMC 4523637 · doi ↗ · pubmed ↗