Multiplex Polymerase Chain Reaction (PCR) and Conventional Methods for Diagnosing Ventilator-Associated Pneumonia in ICU Settings: A Systematic Review
Aalaa Salih Fadel Yosif, Gidaa Khalid Eltayeb Blado, Mohamed Awad Bashir Eltayeb, Nada Abdelrahman Shamina, Mohamed Abass Ahmed Abdalaziz, Amina Osman

TL;DR
This systematic review compares mPCR with conventional methods for diagnosing VAP in ICUs, highlighting mPCR's faster results and high accuracy in ruling out infection.
Contribution
The study provides a systematic comparison of mPCR and conventional methods for VAP diagnosis, emphasizing mPCR's clinical utility and antimicrobial stewardship benefits.
Findings
mPCR showed high pooled sensitivity and specificity with a near 100% negative predictive value.
mPCR significantly reduced turnaround time, enabling faster antibiotic adjustments in ICU patients.
Positive predictive value was variable, highlighting the need for clinical context in interpreting mPCR results.
Abstract
Ventilator-associated pneumonia (VAP) is a prevalent and serious infection in intensive care units (ICUs), with timely and accurate diagnosis being crucial for patient outcomes. Conventional diagnostic methods, primarily culture-based, are hampered by long turnaround times and limited sensitivity. Multiplex polymerase chain reaction (PCR) (mPCR) offers rapid detection of multiple pathogens and resistance genes, potentially revolutionizing VAP diagnosis and antimicrobial stewardship. This systematic review aims to compare the diagnostic performance and clinical impact of mPCR versus conventional methods for diagnosing VAP in ICU settings. This review was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. A comprehensive search of PubMed/MEDLINE, Embase, Web of Science, Scopus, and the Cochrane Library was performed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
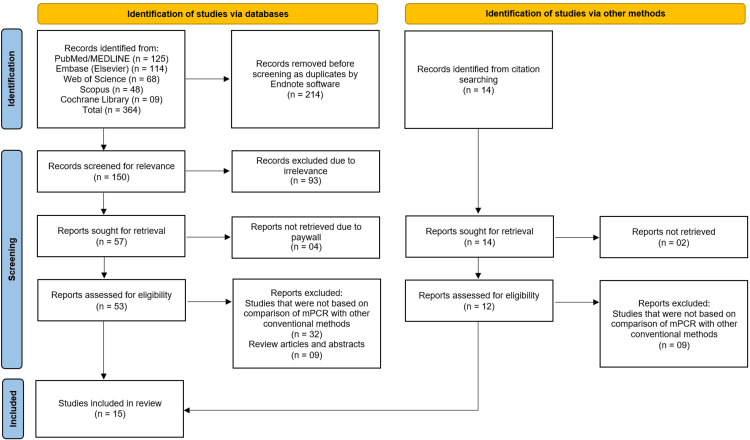 Figure 1
Figure 1| Author (Year) | Country | Study Design | Sample Size | Population (ICU type/patients) | Diagnostic Methods Compared | Reference Standard Used | Key Pathogens Detected |
| Contier et al., [ | France | Retrospective, single-center study | 114 | Critically ill immunocompromised patients with acute respiratory failure requiring invasive ventilation | BioFire FilmArray Pneumonia Panel multiplex PCR (BFPP mPCR) vs. conventional culture (CC) | CC | Enterobacteria (51%), multi-resistant bacteria; others of low pathogenicity not included in mPCR panel |
| Aissaoui et al., [ | Morocco | Multicenter observational study | 210 | Adult patients with pneumonia requiring invasive mechanical ventilation (CAP, HAP, VAP) | Multiplex PCR (mPCR) vs. conventional microbiological methods | Conventional microbiological methods | NR |
| Bay et al., [ | France | Prospective | 294 admitted; 168 mechanically ventilated; 41 episodes for diagnostic evaluation | ICU patients with ESBL-E carriage | BioFire® FilmArray® Pneumonia Plus Panel (mPCR) vs. CC | CC | ESBL-producing Enterobacterales (blaCTX-M), Carbapenem-resistant bacteria |
| Virk et al., [ | USA | Single-centre, open-label, pragmatic, randomized controlled trial | 1152 (modified intention-to-treat) | Hospitalized adults (≥18 years) with suspected pneumonia | BioFire FilmArray pneumonia panel vs. CC and antimicrobial susceptibility testing | CC and antimicrobial susceptibility testing | Gram-positive and Gram-negative bacteria |
| Pickens et al., [ | USA | Observational, single-center | 179 patients (386 BAL samples) | ICU patients with severe SARS-CoV-2 pneumonia requiring mechanical ventilation | Multiplex PCR panel vs. quantitative culture of BAL fluid | Quantitative culture of BAL fluid | Difficult-to-treat pathogens |
| Hou et al., [ | China (Zhongshan Hospital, Fudan University) | Prospective observational study | 12 patients (51 specimens) | ICU patients diagnosed with VAP after mechanical ventilation | PCR/ESI-MS vs. Routine Clinical Culture | Routine Clinical Culture | Common VAP pathogens (16 bacterial isolates confirmed, e.g., multiple bacterial species; 15 confirmed by paired culture, including typical VAP-causing bacteria) |
| Peiffer-Smadja et al., [ | France | Prospective study | 95 clinical samples from 85 patients | ICU patients with ventilated HAP or VAP; conducted in three ICUs (medical and infectious diseases ICU, surgical ICU, cardio-surgical ICU) | mPCR (Unyvero Hospitalized Pneumonia test) vs. conventional microbiological methods (culture) | CC methods | Gram-negative bacilli, Gram-positive cocci, extended-spectrum beta-lactamase producers (CTX-M), carbapenemase producers (NDM, OXA-48), Legionella |
| van der Schalk et al., [ | Belgium | Diagnostic accuracy study | 80 endotracheal aspirates (40 | Mechanically ventilated ICU patients | Semi-quantitative culture, quantitative culture (ChromID | Extended gold standard (positive if detected by any of the four methods beyond semi-quantitative culture) | Pseudomonas aeruginosa |
| Luyt et al., [ | France | Prospective observational study (Jan 2016 – Jan 2019) | 93 BALF samples | ICU patients with suspected VAP undergoing bronchoscopy; BALF microscopy showing intracellular bacteria | Multiplex PCR (Unyvero pneumonia cartridge) vs. CC and antimicrobial susceptibility testing | Conventional microbiological culture (gold standard) |
|
| Enne et al., [ | UK | Prospective observational study | 652 samples | ICU patients receiving new or changed antibiotics for hospital-onset lower respiratory tract infections | BioFire FilmArray Pneumonia Panel, Unyvero Pneumonia Panel vs. Routine microbiology | Routine microbiology, Bayesian latent class analysis | Common HAP/VAP pathogens |
| Karolyi et al., [ | Austria | Retrospective observational study | 60 | Critically ill COVID-19 patients in ICU with suspected HAP/VAP | Multiplex PCR (BioFire® Pneumonia Panel) vs. Microbiological culture | Microbiological culture of respiratory specimens |
|
| Loughlin et al., [ | UK | Prospective cohort (2 studies) | 360 (194 tested) | Critically ill adults with suspected ventilator-associated pneumonia (non-neutropenic) | Mycological testing (BAL fluid culture, serum/BAL galactomannan, histology/microscopy) | Probable Aspergillus infection definition (clinical + radiological + mycological criteria) |
|
| Monard et al., [ | France | Retrospective multicenter study | 159 pneumonia episodes | Adult patients; mostly ICU (n = 129, 81%); HAP (n = 68), CAP (n = 54), VAP (n = 37) | Syndromic rapid multiplex PCR (rm-PCR) vs. conventional microbiological methods | CC (microbiologically documented episodes) | ≥1 bacteria per episode |
| Razazi et al., [ | France | Observational | 95 patients (125 samples) | Mechanically ventilated ARDS patients in two ICUs (including 73 COVID-19 patients, 28 on ECMO) | Multiplex PCR (FilmArray Pneumonia Plus Panel) vs. CC | CC | NR |
| Rouzé et al., [ | Europe | Multicenter retrospective cohort | 1576 | Adult ICU patients on invasive mechanical ventilation >48 hours; SARS-CoV-2, influenza, or no viral infection | NR | Clinical, radiological, and quantitative microbiological criteria | Gram-negative bacilli ( |
| Author (Year) | Multiplex PCR Platform Used | Conventional Method Used | Sensitivity (%) | Specificity (%) | Positive Predictive Value (%) | Negative Predictive Value (%) | Turnaround Time (Hours) |
|
Contier et al., [ | BioFire FilmArray Pneumonia Panel (BFPP mPCR) | CC | 89 | 83 | 52 | 98 | 2.5-4 |
|
Aissaoui et al., [ | NR | NR | 96.9 | 92 | NR | NR | NR |
|
Bay et al., [ | BioFire® FilmArray® Pneumonia Plus Panel | Culture on respiratory samples | NR | 85% concordance reported | 60% (for blaCTX-M detected ESBL-E pneumonia) | 100% (all blaCTX-M negative were culture negative) | NR |
|
Virk et al., [ | BioFire FilmArray Pneumonia Panel (bioMérieux, USA) | Standard culture + antimicrobial susceptibility testing | NR | NR | NR | NR | Median 20.4 (any antibiotic modification), 13.8 (antibiotic escalation), 20.7 (de-escalation for Gram-positive) |
|
Pickens et al., [ | Multiplex PCR panel | Quantitative culture of BAL fluid | NR | NR | NR | NR | NR |
|
Hou et al., [ | Sequential PCR coupled to electrospray ionization mass spectrometry (PCR/ESI-MS) | Routine clinical culture | 14/16 VAP-confirmed isolates identified = ~87.5% | NR | NR | NR | ~6 |
|
Peiffer-Smadja et al., [ | Unyvero Hospitalized Pneumonia (HPN, Curetis) | Culture (BAL/PTC samples) | 80% overall (90% for Gram-negative; 62% for Gram-positive cocci) | 99% | NR | NR | Median 4.6 (IQR 4.4-5) |
|
van der Schalk et al., [ | GeneXpert PA PCR assay | Semi-quantitative culture | 97.6 | 100 | NR | NR | ~0.9 (≈55 min) |
|
Luyt et al., [ | Unyvero pneumonia cartridge | BALF cultures (gold standard) | 73 | NR | NR | NR | 4-5 |
|
Enne et al., [ | BioFire FilmArray (bioMérieux) and Unyvero (Curetis) | Routine microbiology | 50-100 | 87.5-99.5 | NR | NR | NR |
|
Karolyi et al., [ | BioFire® Pneumonia Panel (PP) | Microbiological culture | NR | NR | NR | NR | NR |
|
Loughlin et al., [ | NR | BAL fluid culture, serum/BAL galactomannan, histology/microscopy | NR | NR | NR | NR | NR |
|
Monard et al., [ | Syndromic rapid multiplex PCR (rm-PCR) | Standard culture | NR | NR | NR | NR | NR |
|
Razazi et al., [ | FilmArray Pneumonia Plus Panel (bioMérieux, France) | Standard culture | 93 (95% CI 84-100) | 99 (95% CI 99-100) | 68 (95% CI 54-83) | 100 (95% CI 100-100) | NR |
|
Rouzé et al., [ | NR | Clinical, radiological, quantitative microbiology | NR | NR | NR | NR | NR |
| Study (Year) | Risk of Bias | Applicability Concerns | |||||
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
|
Contier et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Aissaoui et al., [ | Low risk | Low risk | Low risk | High risk | Low concern | Low concern | Low concern |
|
Bay et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Virk et al., [ | Low risk | Unclear risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Pickens et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Hou et al., [ | Low risk | Low risk | Low risk | High risk | Low concern | Low concern | Low concern |
|
Peiffer-Smadja et al., [ | Low risk | Low risk | Low risk | High risk | Low concern | Low concern | Low concern |
|
van der Schalk et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Luyt et al., [ | Low risk | Low risk | Low risk | Unclear risk | Low concern | Unclear concern | Low concern |
|
Enne et al., [ | Low risk | Low risk | Low risk | High risk | Low concern | Unclear concern | Low concern |
|
Karolyi et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Loughlin et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Monard et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Razazi et al., [ | Low risk | Low risk | Low risk | Low risk | Low concern | Low concern | Low concern |
|
Rouzé et al., [ | Low risk | Unclear risk | Low risk | Low risk | Low concern | Unclear concern | Low concern |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial Identification and Susceptibility Testing · Nosocomial Infections in ICU · Pneumonia and Respiratory Infections
Introduction and background
Ventilator-associated pneumonia (VAP) remains one of the most prevalent and severe healthcare-associated infections in intensive care units (ICUs). It is clinically defined as pneumonia that develops 48 hours or more after endotracheal intubation and initiation of mechanical ventilation, characterized by new or progressive pulmonary infiltrates on chest imaging accompanied by clinical signs such as fever, purulent tracheal secretions, leukocytosis, and worsening oxygenation [1]. VAP is associated with prolonged mechanical ventilation, extended hospital stays, increased healthcare costs, and significant morbidity and mortality among critically ill patients. Timely and accurate diagnosis of VAP is therefore crucial to guide appropriate antimicrobial therapy, reduce complications, and improve patient outcomes [2].
Traditionally, the diagnosis of VAP has relied on conventional methods such as culture-based techniques and clinical criteria [3]. While microbiological cultures remain the gold standard, they are often limited by long turnaround times (TATs), reduced sensitivity due to prior antibiotic exposure, and challenges in differentiating colonization from true infection [4]. These limitations can lead to delays in treatment initiation, inappropriate antibiotic use, and the emergence of antimicrobial resistance, which poses a growing threat in ICU settings.
In recent years, Multiplex polymerase chain reaction (PCR) (mPCR) assays have emerged as promising molecular diagnostic tools for detecting respiratory pathogens directly from clinical samples [5]. mPCR offers the advantages of rapid TAT, high sensitivity, and the ability to simultaneously detect multiple bacterial and viral pathogens, as well as antimicrobial resistance genes [6]. These features may facilitate early, targeted therapy and antimicrobial stewardship in critically ill patients with suspected VAP. However, questions remain regarding the accuracy, cost-effectiveness, and clinical impact of mPCR compared with conventional diagnostic methods [7].
Several studies have compared mPCR platforms with standard microbiological cultures and clinical diagnostic criteria in the context of VAP [8,9]. While some have demonstrated superior diagnostic yield and faster results, others have raised concerns about specificity, detection of non-pathogenic colonizers, and integration into clinical decision-making. A systematic evaluation of the current evidence is therefore warranted to clarify the diagnostic performance and clinical utility of mPCR relative to conventional methods in ICU practice.
This systematic review aims to critically compare mPCR with conventional diagnostic methods for VAP in ICU settings. Specifically, it will examine diagnostic accuracy, TAT, detection of key pathogens and resistance markers, and potential implications for patient management and antimicrobial stewardship.
Review
Methodology
Study Design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [10].
Eligibility Criteria
This systematic review included original research studies that compared mPCR assays with conventional diagnostic methods, such as culture-based techniques, for diagnosing VAP in ICU patients. Only studies published within the last five years were considered, in order to focus on the most recent advances and ensure clinical relevance to current ICU practice. Eligible studies were those reporting diagnostic accuracy outcomes such as sensitivity, specificity, predictive values, or TAT. Reviews, conference abstracts, editorials, case reports, and studies not conducted in ICU populations were excluded.
Information Sources and Search Strategy
A comprehensive search of electronic databases was conducted, including PubMed/MEDLINE, Embase, Web of Science, Scopus, and the Cochrane Library. The search strategy was designed using a combination of controlled vocabulary and free-text terms related to “ventilator-associated pneumonia,” “multiplex PCR,” “molecular diagnostics,” and “conventional methods.” To ensure completeness, the reference lists of all included studies and relevant reviews were screened for additional eligible studies through citation searching.
Selection Process
All records retrieved from the databases were imported into EndNote (Clarivate, Philadelphia, PA) reference management software, where duplicates were identified and removed. The remaining articles were independently screened by two reviewers, first by title and abstract, and then by full text, to determine eligibility based on the inclusion and exclusion criteria. Disagreements at any stage were resolved through discussion and consensus.
Data Collection Process
Data were extracted from each included study using a standardized data extraction form. Extracted information included study characteristics (country, year of publication, study design, and sample size), patient population (ICU type and clinical characteristics), diagnostic methods compared, reference standards used, key pathogens identified, diagnostic performance outcomes (sensitivity, specificity, positive predictive value (PPV), NPV), and TAT. To minimize errors, data extraction was performed by one reviewer and cross-checked by a second reviewer.
Study Risk of Bias Assessment
The quality and risk of bias of the included studies were evaluated using the QUADAS-2 tool [11], which is specifically designed for studies of diagnostic accuracy. The tool assesses risk across four domains: Patient Selection, Index Test, Reference Standard, and Flow and Timing. Each domain was judged as having a low, high, or unclear risk of bias. The results of the assessment are presented in tabular form.
Synthesis of Results
Given the heterogeneity in study designs, patient populations, mPCR platforms, and reference standards used across the included studies, conducting a quantitative meta-analysis was not appropriate. Pooling the results could have introduced significant bias and misrepresented the true diagnostic performance of mPCR in the clinical setting. Therefore, a qualitative synthesis was performed, with findings summarized narratively and presented in comparative tables to highlight similarities, differences, and key trends across studies.
Results
Study Selection and Characteristics
A comprehensive literature search across PubMed/MEDLINE, Embase, Web of Science, Scopus, and the Cochrane Library yielded a total of 364 records. An additional 14 records were identified through citation searching, bringing the total to 378 records. After removing 214 duplicates using EndNote software, 164 unique records remained for screening. Of these, 150 records were screened based on title and abstract, leading to the exclusion of 93 records due to irrelevance. The full texts of 57 articles were sought for retrieval; however, four reports could not be retrieved due to paywall restrictions, and two reports were not available. Consequently, 51 full-text articles were assessed for eligibility. Following full-text assessment, 41 reports were excluded: 32 did not compare mPCR with conventional methods, and nine were review articles or abstracts only (Figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart
A total of 15 studies [12-26] were included in this systematic review, published between 2020 and 2025. The characteristics of these studies are summarized in Table 1. The included studies were conducted across a diverse range of geographical locations, including France [12,14,18,20,24,26], the USA [15,16], the UK [21,23], Morocco [13], China [17], Belgium [19], Austria [22], and a multicenter European cohort [26]. Sample sizes varied considerably, ranging from 12 patients [17] to 1,576 patients [26], reflecting a mix of single-center and multicenter designs.
The study designs were predominantly observational, including prospective [14,17,18,20,21] and retrospective [12,22,24,26] cohorts, with one randomized controlled trial [15]. The patient population consistently focused on critically ill adults in ICUs requiring invasive mechanical ventilation. The studies investigated various forms of pneumonia, including VAP, hospital-acquired pneumonia (HAP), and community-acquired pneumonia (CAP) in intubated patients, and pneumonia in specific subpopulations such as immunocompromised patients [12], those with ARDS [25], and patients with severe COVID-19 [16,22,26].
A variety of mPCR platforms were evaluated against conventional microbiological culture (CC) as the reference standard. The most commonly used platforms were the BioFire FilmArray Pneumonia Panel (BFPP) or its extended version (Pneumonia Plus Panel) [12,14,15,21,22,25] and the Unyvero Hospitalized Pneumonia (HPN) cartridge [18,20,21]. Other platforms included syndromic rapid mPCR tests [24], PCR/electrospray ionization mass spectrometry (PCR/ESI-MS) [17], and specific assays like the GeneXpert PA for Pseudomonas aeruginosa [19]. The key pathogens detected across studies included Gram-negative bacilli (e.g., Pseudomonas aeruginosa, Klebsiella spp., Enterobacter spp., ESBL-producing Enterobacterales) and Gram-positive cocci (e.g., Staphylococcus aureus), with some panels also detecting resistance markers and fungal pathogens [18,20,23].
Diagnostic Performance of Multiplex PCR
The diagnostic performance metrics of mPCR compared to conventional methods are detailed in Table 2. The reported sensitivity and specificity of mPCR were generally high, though variable across studies.
Sensitivity values ranged from 50% to 100% for detecting pathogens included in the respective panels [21]. Several studies reported high sensitivity; for instance, Aissaoui et al. reported a sensitivity of 96.9% [13], while van der Schalk et al. reported 97.6% for the specific detection of Pseudomonas aeruginosa using the GeneXpert PA assay [19]. Similarly, Razazi et al. reported a sensitivity of 93% (95% CI 84-100) for the FilmArray Pneumonia Plus Panel [25]. Specificity was consistently very high, often exceeding 90% and reaching 100% in some evaluations [19,25]. For example, Contier et al. reported a specificity of 83% and a notably high NPV of 98%, suggesting a strong ability to rule out infection when the test result is negative [12].
The PPV was more variable and often lower, reflecting the impact of colonization and the high sensitivity of mPCR. Contier et al. reported a PPV of 52% [12], and Razazi et al. reported a PPV of 68% (95% CI 54-83) [25], indicating that a positive mPCR result requires careful clinical correlation to distinguish true infection from colonization. Conversely, the NPV was consistently high, often approaching 100% [12,14,25], underscoring the utility of mPCR for discontinuing unnecessary antibiotics when results are negative.
A key advantage consistently demonstrated by mPCR was its significantly reduced TAT compared to conventional culture. TAT for mPCR results ranged from approximately 55 minutes [19] to six hours [17], with most platforms providing results within 2.5 to five hours [12,18,20]. In contrast, conventional culture and antimicrobial susceptibility testing typically require 48 to 72 hours, a delay that impacts timely clinical decision-making.
Impact on Antimicrobial Management
While not the primary focus of all studies, several investigations highlighted the potential impact of rapid mPCR results on antimicrobial stewardship. The drastically shortened TAT facilitated earlier adaptation of antibiotic therapy. Virk et al., in a randomized controlled trial, reported median times to any antibiotic modification of 20.4 hours, with escalation occurring at a median of 13.8 hours and de-escalation for Gram-positive organisms at 20.7 hours based on mPCR results [15].
Bay et al. focused on patients with ESBL-E carriage and found that while the PPV for ESBL-E pneumonia was 60%, the NPV was 100%; all patients with a negative mPCR for the blaCTX-M gene were culture-negative, potentially allowing for the avoidance of unnecessary carbapenem therapy [14]. Other studies similarly suggested that rapid negative results could support the early discontinuation of antibiotics, while positive results could guide earlier targeted or appropriate therapy, especially in cases where empiric coverage was inadequate [18,20,24,25].
Risk of Bias Findings
The overall risk of bias across the included studies was predominantly low, though some key concerns were noted in specific domains. The Patient Selection domain was judged as low risk for all 15 studies [12-26], indicating that the methods for selecting participants were appropriate. Similarly, the Reference Standard domain was rated low risk for all studies [12-26], confirming that conventional culture methods were applied correctly. For the Index Test, the risk of bias was low for most studies [12-14, 16-19, 22-25], though it was unclear for Virk et al. [15], Luyt et al. [20], and Rouzé et al. [26] due to insufficient information on whether the mPCR interpretation was blinded to culture results, resulting in an unclear risk in the Index Test domain. The Flow and Timing domain presented the most variability, with a high risk of bias identified in Aissaoui et al. [13], Hou et al. [17], Peiffer-Smadja et al. [18], and Enne et al. [21], often relating to inappropriate exclusions or timing issues between index and reference tests, while the risk was unclear for Luyt et al. [20] and low for the remaining studies [12,14-16,19,22-26]. Regarding applicability concerns, the Patient Selection and Reference Standard domains were of low concern for all studies [12-26]. Concerns regarding the Index Test were low for the majority [12-19,22-26], but were unclear for Luyt et al. [20], Enne et al. [21], and Rouzé et al. [26], typically because the test's application or representativeness for the review question was not fully detailed (Table 3).
Discussion
This systematic review evaluated the diagnostic performance and clinical utility of mPCR platforms compared to conventional culture-based methods for diagnosing VAP in ICUs. The analysis of 15 studies reveals that mPCR technology offers transformative potential through dramatically reduced TATs (often under six hours compared to 48-72 hours for conventional methods) and excellent NPV, though its clinical implementation requires careful interpretation due to challenges in distinguishing colonization from true infection [12,15,17-20].
The consistently high sensitivity and specificity observed across studies, ranging from 87.5% to 100% for specific pathogens [13,19,25], confirms the technical reliability of mPCR systems for detecting target nucleic acids. The exceptional NPV, frequently approaching 100% [12,14,25], represents perhaps the most clinically significant advantage. This high NPV provides clinicians with confidence to discontinue unnecessary broad-spectrum antibiotics when mPCR results are negative, potentially reducing antimicrobial selective pressure in ICUs. However, the variable PPVs (52-68% in some studies [12, 25]) reflect the persistent challenge of differentiating true infection from respiratory colonization, a limitation also noted in previous meta-analyses by High et al. [27] and Webber et al. [28]. This diagnostic ambiguity necessitates careful correlation of mPCR results with clinical signs, biomarkers, and radiological findings, echoing recommendations from Klompas et al. [29] regarding VAP diagnosis generally.
The impact on antimicrobial stewardship emerges as a particularly promising aspect of mPCR implementation. The randomized controlled trial by Virk et al. [15] demonstrated that mPCR-guided therapy led to antibiotic modifications within a median of 20.4 hours, substantially faster than conventional methods. This finding aligns with research by Burillo et al. [30], who showed that rapid diagnostic methods can reduce time to appropriate antibiotic therapy by approximately 24 hours. The study by Bay et al. [14] provided particularly valuable insights for managing patients with ESBL-E carriage, showing that negative mPCR for blaCTX-M genes had 100% NPV for excluding ESBL-E pneumonia, potentially enabling avoidance of unnecessary carbapenem therapy. This application addresses a specific concern raised by Bassetti et al. [31] regarding carbapenem overuse in ICUs.
When contextualized within the broader literature, our findings both confirm and extend previous knowledge. The diagnostic accuracy metrics we observed are consistent with those reported in the study by Wang et al. [32], who found pooled sensitivity and specificity exceeding 90% for mPCR systems. However, our review provides several important advancements: inclusion of more recent studies through 2025, evaluation of diverse platforms (BioFire, Unyvero, PCR/ESI-MS, GeneXpert), and focus on specific challenging subpopulations, including immunocompromised hosts [12], COVID-19 patients [16,22,26], and ESBL-E carriers [14]. The detection of resistance markers directly from samples, as demonstrated by Peiffer-Smadja et al. [18] and Luyt et al. [20], represents a particular advantage over conventional methods, providing early warning of resistance mechanisms that can inform therapy days before traditional susceptibility results are available, addressing a critical need identified by Timbrook et al. [33] in their review of rapid diagnostic technologies.
Despite these advantages, several implementation challenges persist. The fixed pathogen menus of mPCR panels mean they cannot detect novel or uncommon pathogens outside their predetermined scope, as noted by Contier et al. [12], requiring continued use of conventional culture as a complementary method. The substantial upfront costs of equipment and test cartridges present economic barriers to widespread adoption, a concern also raised by Messacar et al. [34] regarding molecular diagnostic platforms generally. Furthermore, the clinical utility of mPCR depends heavily on effective antimicrobial stewardship programs to ensure rapid clinical response to diagnostic results, supporting the implementation model proposed by Banerjee et al. [35] that integrates rapid diagnostics with stewardship initiatives.
The findings from studies of specific populations offer particularly valuable insights. In immunocompromised patients [12], where infectious complications carry high mortality risks, the rapid exclusion of bacterial pneumonia through mPCR's high NPV could prevent unnecessary antibiotic exposure during vulnerable periods. For COVID-19 patients [16,22,26], who frequently experience bacterial superinfections but also receive empiric antibiotics, mPCR might help distinguish viral from bacterial pathology, addressing the diagnostic challenges described by Hughes et al. [36] during the pandemic.
Limitations
This systematic review has several limitations that should be acknowledged. The heterogeneity in study designs, patient populations, and mPCR platforms prevented quantitative meta-analysis. The QUADAS-2 assessment identified recurring methodological challenges in the "Flow and Timing" domain, reflecting the inherent difficulty of using culture, an imperfect reference standard with limited sensitivity, to validate a more sensitive molecular test. This fundamental mismatch may lead to an underestimation of mPCR's true performance characteristics. Additionally, publication bias may favor studies with positive results, and the generalizability of findings may be limited for some platforms or specific patient subgroups. Furthermore, most mPCR panels are fixed pathogen panels and cannot detect unusual or novel organisms, and they cannot reliably distinguish colonization from true infection. Economic considerations, including the high cost of mPCR and the need for integration with antimicrobial stewardship programs, may limit widespread implementation. Other limitations include exclusion of non-English studies and studies behind paywalls, variability in reported clinical outcomes, and potential biases in the included studies. Finally, most studies were conducted in high-resource ICU settings, which may reduce the applicability of findings to low-resource or diverse healthcare environments.
Conclusions
Multiplex PCR represents a significant advancement in the rapid microbiological diagnosis of ventilator-associated pneumonia. Its dramatically reduced turnaround time and high negative predictive value offer powerful tools for enhancing antimicrobial stewardship in ICUs, though positive results should be interpreted cautiously as mPCR may detect dead bacteria, leading to false positives. However, the technology requires thoughtful implementation within a framework that acknowledges its limitations, particularly regarding differentiation between colonization and infection. mPCR should be viewed as a complementary diagnostic tool rather than a replacement for conventional methods, with its full potential realized through integration with antimicrobial stewardship programs and clinical correlation. Future research should focus on randomized trials measuring clinically important outcomes including mortality, ICU length of stay, and antimicrobial resistance rates, complemented by formal economic evaluations to establish the cost-effectiveness of these technologies in diverse healthcare settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ventilator associated pneumonia in intensive care unit patients: a systematic review Ann Med Surg (Lond) Mumtaz H Saqib M Khan W Ismail SM Sohail H Muneeb M Sheikh SS 293229398520233736347010.1097/MS 9.0000000000000836 PMC 10289715 · doi ↗ · pubmed ↗
- 2Hospital-acquired pneumonia and ventilator-associated pneumonia: a literature review Microorganisms Miron M Blaj M Ristescu AI 312202410.3390/microorganisms 12010213 PMC 1082046538276198 · doi ↗ · pubmed ↗
- 3Metagenomics for the microbiological diagnosis of hospital-acquired pneumonia and ventilator-associated pneumonia (HAP/VAP) in intensive care unit (ICU): a proof-of-concept study Respir Res Heitz M Levrat A Lazarevic V 2852420233796863610.1186/s 12931-023-02597-x PMC 10648381 · doi ↗ · pubmed ↗
- 4Emerging strategies for the noninvasive diagnosis of nosocomial pneumonia Expert Rev Anti Infect Ther Liapikou A Cillóniz C Torres A 5235331720193123746210.1080/14787210.2019.1635010 PMC 7103721 · doi ↗ · pubmed ↗
- 5Advances in the application of molecular diagnostic techniques for the detection of infectious disease pathogens (review)Mol Med Rep Liu Q Jin X Cheng J Zhou H Zhang Y Dai Y 12720233702650510.3892/mmr.2023.12991 PMC 10086565 · doi ↗ · pubmed ↗
- 6Bacterial multiplex polymerase chain reaction tests for the diagnosis and management of pneumonia: ready for prime time?Thorax Ling L Lai CK Rhee C 72202510.1136/thorax-2024-22229740473414 · doi ↗ · pubmed ↗
- 7Design, optimization, and application of multiplex r RT-PCR in the detection of respiratory viruses Crit Rev Clin Lab Sci Yang J Li D Wang J Zhang R Li J 5555725920223555971110.1080/10408363.2022.2072467 · doi ↗ · pubmed ↗
- 8Potential impact of rapid multiplex PCR on antimicrobial therapy guidance for ventilated hospital-acquired pneumonia in critically ill patients, a prospective observational clinical and economic study Front Cell Infect Microbiol Guillotin F Poulain C Gaborit B 8046111220223549373010.3389/fcimb.2022.804611 PMC 9043525 · doi ↗ · pubmed ↗