Pulmonary Embolism in a Patient With Undifferentiated Dyspnoea
Yun Hung Chor

TL;DR
A 76-year-old man on blood thinners developed a severe lung blood clot despite medication, highlighting the need for careful diagnosis and possible benefits of newer anticoagulants.
Contribution
Demonstrates that pulmonary embolism can occur even with anticoagulant therapy, suggesting potential advantages of direct-acting oral anticoagulants over warfarin.
Findings
Pulmonary embolism occurred in a patient on warfarin and clopidogrel, indicating subtherapeutic anticoagulation.
Direct-acting oral anticoagulants may reduce progression to pulmonary embolism compared to warfarin.
Non-specific symptoms of pulmonary embolism can mimic acute heart failure, requiring high clinical suspicion for accurate diagnosis.
Abstract
Pulmonary embolism can cause right and left ventricular dysfunction and induce acute heart failure or shock. A 76-year-old gentleman with a history of ischaemic heart disease and atrial fibrillation, on oral warfarin and clopidogrel daily, presented with a three-day history of worsening shortness of breath associated with a dull ache over the right side of his chest. On examination, auscultation of his lungs revealed mild crepitations bilaterally at the bases and bilateral pitting oedema of legs up to his shins. His ECG showed ST-segment depression in lead 1, aVL, V2 to V6. His Chest X-ray showed cardiomegaly with minimal bilateral lower zone haziness. The initial provisional diagnosis was decompensated heart failure, and the patient was referred to acute medicine. His blood tests later showed a white cell count (WCC) of 15, CRP 298 and D-Dimer of 35317. This was followed by a computed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
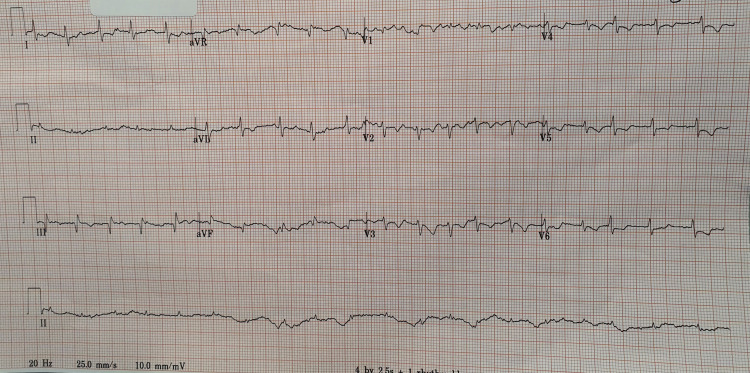 Figure 1
Figure 1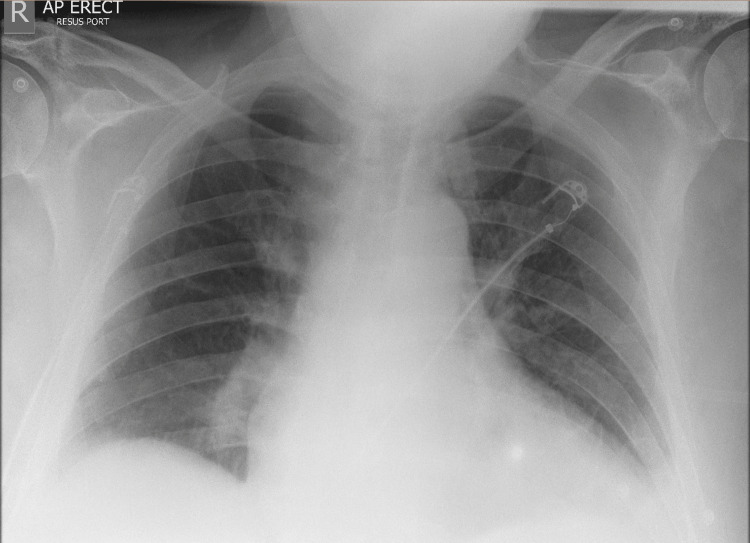 Figure 2
Figure 2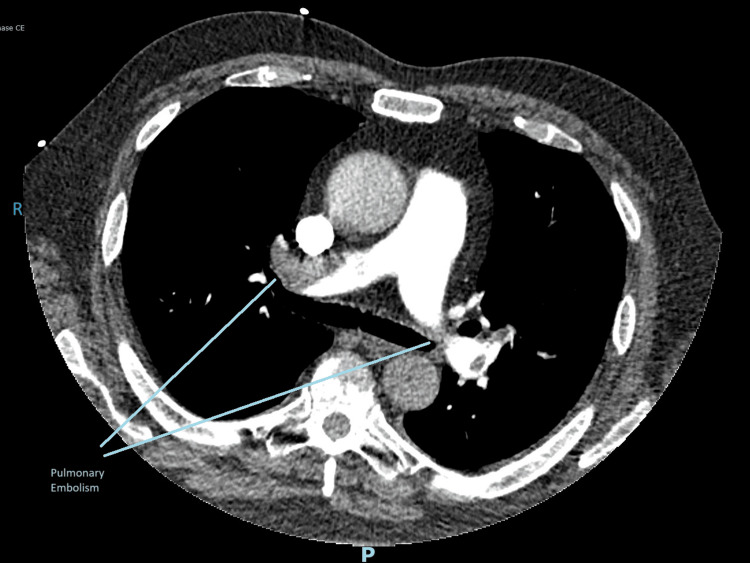 Figure 3
Figure 3| Parameter | Patient's values | Reference values |
| White cell count (WCC; x109 /L | 15 (neutrophils 12.19) | 4.0-11.0 |
| Haemoglobin (Hb; g/L) | 168 | 130-180 |
| Platelet (g/L) | 190 | 150-450 |
| D-dimer (ng/ml FEU) | 35317 | 0-500 |
| C-reactive protein (CRP; mg/L) | 298 | <5 |
| Bilirubin (μmol/L) | 44 | 0-21 |
| Alkaline phosphatase (ALP; U/L) | 263 | 30-130 |
| Total protein (g/L) | 73 | 60-80 |
| Alanine aminotransferase (ALT; U/L) | 53 | 10-50 |
| Troponin T (ng/L) | 39 | <14 |
| B-type natriuretic peptide (NT-pro BNP; pg/ml) | 5242 | <400 |
| International normalised ratio (INR) | 1.5 | 1.0-1.3 |
| Partial thromboplastin time ratio (PTR) | 0.8 | 0.9-1.1 |
| Urea (mmol/L) | 9.3 | 2.5-7.8 |
| Sodium (mmol/L) | 138 | 133-146 |
| Potassium (mmol/L) | 4.7 | 3.5-5.3 |
| Creatinine (μmol/L) | 134 | 59-104 |
| COVID and Influenza polymerase chain reaction (PCR) | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Venous Thromboembolism Diagnosis and Management · Cardiovascular and Diving-Related Complications
Introduction
The epidemiology of pulmonary embolism (PE) can be difficult to predict, as the first presentation of a patient can be cardiac arrest. We present a case of undifferentiated dyspnoea with heart failure, which was caused by PE along with pre-existing cardiac disease. This patient developed a PE despite receiving dual therapy with warfarin and clopidogrel. We also highlight the importance of factors affecting the efficacy of vitamin K antagonists and the effectiveness of direct-acting oral anticoagulants (DOAC).
Acute heart failure and PE can clinically present in a similar way and often share similar risk factors. The diagnosis of dyspnoea can be difficult. Hypertension, dyslipidemia, diabetes, obesity, smoking, malnutrition, stress and estrogen therapy have significant effects on endothelial function, inflammation and hypercoagulable state. This results in the development of atherothrombosis, which leads to ischaemic heart disease, heart failure, and venous thrombosis. These factors can ultimately cause PE. Patients with cardiac disease, such as coronary artery disease and atrial fibrillation, also display a higher risk for PE. Many studies have shown that patients with previous myocardial infarction have a high risk of developing PE. Patients with heart failure have nearly double the risk of developing PE than those without it [1]. In addition, PE can cause right and left ventricular dysfunction and induce acute heart failure or shock. The diagnosis of massive PE is difficult because of its non-specific clinical presentation and the absence of definitive findings on non-invasive cardiac imaging. In around one third of patients, a massive PE presents with pleuritic chest pain with or without dyspnoea. The patient may present with retrosternal chest pain that mimics angina. Besides, cardiac syncope can be a hallmark of massive PE with ventricular failure and severe pulmonary hypertension. Even with the latest advanced therapies and anticoagulation therapies, mortality remains high [2]. This case illustrates a diagnostic challenge, describing a patient who presented with undifferentiated dyspnoea and was found to have a massive PE despite ongoing dual anticoagulation and antiplatelet therapy thereby highlighting the complex diagnostic and therapeutic challenges involved.
Case presentation
A 76-year-old gentleman with a history of ischaemic heart disease and atrial fibrillation, and on oral warfarin 5 mg and clopidogrel 75 mg daily, presented with a three-day history of worsening shortness of breath associated with a dull ache over the right side of his chest. He had also developed bilateral leg swelling and orthopnoea. He had reduced mobility for two days due to shortness of breath and claimed that he had been compliant with his medication. He had last taken his dose of clopidogrel and warfarin the evening before he came to the hospital. There were no symptoms of fever or coughing. Prior to this presentation, he was fully independent in his activities of daily living and did not use mobility aids. He denied any recent medication or dietary change. We were unable to retrieve his recent INR readings from the anticoagulation clinic prior to admission; however, he claimed the recent reading was optimal.
On arrival, his oxygen saturation on room air was 90%, blood pressure was 85/60 mmHg, temperature was 37.5 °C, heart rate was between 90-120 bpm, and Glasgow coma score was 15/15. On examination, auscultation of his lungs revealed mild crepitations bilaterally at the bases and bilateral pitting oedema of legs up to his shins. His ECG showed an ST-segment depression in lead 1, aVL, V2 to V6 (Figure 1).
ECG of the patient
His arterial blood gas showed type 1 respiratory failure, and his chest X-ray showed cardiomegaly with minimal bilateral lower zone haziness (Figure 2).
Chest X-ray of the patient
He had a Wells' score [2] for PE of 1.5. The Initial provisional diagnosis was decompensated heart failure, and the patient was referred to acute medicine. There was ongoing concern that this could be related to an acute coronary syndrome, and Cardiology was also involved. He was given a total of 1 litre of intravenous fluid, in incremental boluses of 250ml; however, his blood pressure did not improve. His blood tests (Table 1) showed high values of D-dimer, white cell count (WCC), and C-reactive protein (CRP).
Following the D-dimer result, patient underwent a computed tomography (CT) pulmonary angiogram. It showed multiple bilateral proximal pulmonary emboli with right heart strain. The pulmonary infarcts in the middle lobe and right lower lobe may explain the right upper quadrant pain (Figure 3).
CT pulmonary angiogram
He was referred to the respiratory and intensive care teams and underwent thrombolysis in critical care setting. He was discharged home with DOAC after five days of hospital admission. No echocardiogram was performed during admission.
Discussion
Nearly 45% of patients with PE will have a right ventricular compromise. There is a reported mortality of up to 25% in a normotensive patient and up to 65% in hypotensive patients with PE.. Massive PE occurs in about 5% of patients with PE and carries a mortality rate of 18-65% [3]. PE can present with non-specific signs and symptoms, making it a challenge to diagnose clinically. It can overlap with heart failure symptoms, especially in patients with underlying ischaemic heart disease.
A key learning point in this case was the development of PE despite the patient being on both warfarin (anticoagulation) and clopidogrel (antiplatelet) treatment. Patients who have received a DOAC will have significantly lower rates of progression to PE and a lower incidence of major bleeding compared with patients receiving warfarin. DOAC also has more predictable anticoagulation. This suggests that DOACs are superior to warfarin for the treatment of deep vein thrombosis [4].
However, it is important to note that DOACs have a relatively short duration of action; therefore, missing even a single dose can result in a rapid loss of anticoagulant effect. This makes the patient's compliance with the medication especially important compared to warfarin, especially after 12 to 24 hours. With warfarin, some benefit is retained for 48 to 72 hours after missing a dose, as it has a longer duration of action [5].
This case also highlights the real-world limitations of vitamin K antagonists, particularly when INR is subtherapeutic. Warfarin can also be affected by other factors. For instance, eating an increased amount of foods rich in vitamin K can lower the prothrombin time (PT) and INR, making warfarin less effective and potentially increasing the risk of blood clots [6]. Some medications can affect warfarin efficacy. An enzyme CYP P450 inducer can lead to a reduction in INR. Some drugs, such as rifampicin and phenytoin, that are enzyme inducers may lower the INR. Chronic alcohol consumption can also have an impact [7].
A D-dimer test is a sensitive but poorly specific diagnostic tool for a patient suspected with a PE (sensitivity 100%, specificity 8.8%). It should, therefore, always be used in conjunction with clinical suspicion [8]. The effect of DOACs and vitamin K antagonists such as warfarin on D-dimer levels was studied previously in patients with atrial fibrillation with inconsistent results. One of the studies showed that D-dimer levels in patients with atrial fibrillation on apixaban were increased in comparison to warfarin users [9].
Dual therapy (oral anticoagulant plus a single antiplatelet agent) has been shown to be effective in reducing thrombotic risks for one year in patients with cardiovascular conditions, including coronary artery disease, atrial fibrillation, and venous thromboembolism. This is particularly noticed when DOACs are combined with the antiplatelet, clopidogrel. Aspirin also reduces risk of cardiovascular death, myocardial infarction, stroke and stent thrombosis particularly in the first 30 days but the benefit does not extend beyond that time point [10].
This case shows the importance of maintaining a high clinical suspicion for PE, even in patients whose presentation mimics heart failure or acute coronary syndrome. Early diagnosis and treatment are the key to survival for such patients, especially when they present with a massive PE, as in our case. This case also supports the clinical transition of warfarin to DOAC especially in patients with complicated ischaemic heart disease and those with subtherapeutic INR.
Conclusions
PE presents with many symptoms and risk factors, which are often similar to other acute coronary conditions and acute heart failure, making early diagnosis very difficult. Clinicians will need to have a high level of suspicion even when the patient is on anticoagulation, or as in this case, where the patient was on both anticoagulation and antiplatelet therapy. PE can still happen, particularly when therapy is subtherapeutic or even when anticoagulation is combined with an antiplatelet agent. Additionally, DOACs may provide more reliable anticoagulation than warfarin in selected patients requiring both anticoagulant and antiplatelet therapy, as warfarin can interact with other medications and food. We need to have individualised anticoagulation strategies for different patients, including consideration of DOACs, which may improve outcomes and reduce the risk of thromboembolism in patients with complex cardiovascular conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pulmonary embolism and heart failure: a reappraisal Card Fail Rev 9 2023 Arrigo M Huber LC 072020 https://doi.org/10.15420/cfr.2020.2610.15420/cfr.2020.26PMC 792647733708418 · doi ↗ · pubmed ↗
- 2Massive pulmonary embolism heart failure: a review of clinical status and meta-analyses of clinical scoring system and D-dimer, and thrombolytic and anticoagulation therapies Int Med Care 9 2023 Albakri A 11422018 https://www.oatext.com/pdf/IMC-2-122.pdf
- 3Pathophysiology of right ventricular failure in acute pulmonary embolism and chronic thromboembolic pulmonary hypertension: a pictorial essay for the interventional radiologist Insights Imaging Bryce YC Perez-Johnston R Bryce EB Homayoon B Santos-Martin EG 18102019 https://doi.org/10.1186/s 13244-019-0695-93075868710.1186/s 13244-019-0695-9PMC 6375098 · doi ↗ · pubmed ↗
- 4Warfarin versus direct oral anticoagulants for patients needing distal deep vein thrombosis treatment J Vasc Surg Venous Lymphat Disord Pham A Heib A Goodman E Cotto R Jafari P Lipsitz E Indes J 826831102022 https://doi.org/10.1016/j.jvsv.2022.01.0063512424310.1016/j.jvsv.2022.01.006 · doi ↗ · pubmed ↗
- 5Management of patients treated with direct oral anticoagulants in clinical practice and challenging scenarios J Clin Med LucàF Oliva F Abrignani MG 5955122023 https://cks.nice.org.uk/topics/atrial-fibrillation/prescribing-information/anticoagulants/3776289710.3390/jcm 12185955 PMC 10531873 · doi ↗ · pubmed ↗
- 6Prevention and Treatment of Arrhythmia 8 2025 420232023 https://www.heart.org/en/health-topics/arrhythmia/prevention--treatment-of-arrhythmia/
- 7Warfarin drug interactions Stat Pearls [Internet] Crader MF Johns T Arnold JK Treasure Island (FL)Stat Pearls Publishinghttps://www.ncbi.nlm.nih.gov/books/NBK 441964/28722993 · pubmed ↗
- 8D-dimer testing for the exclusion of pulmonary embolism among hospitalized patients with COVID-19JAMA Netw Open Logothetis CN Weppelmann TA Jordan A Hanna C Zhang S Charkowick S Oxner A 042021 https://doi.org/10.1001/jamanetworkopen.2021.2880210.1001/jamanetworkopen.2021.28802 PMC 850139634623411 · doi ↗ · pubmed ↗