Adherence to denosumab therapy and fracture risk associated with drug withdrawal: a retrospective study
Hande Özdemir, Nur Kakilli, Filiz Tuna, Buket Yılmaz Bülbül, Mehmet Çelik, Selçuk Korkmaz, Derya Demirbağ Kabayel

TL;DR
This study examines how stopping denosumab treatment affects fracture risk and finds that fractures may occur due to osteoporosis progression, not just treatment discontinuation.
Contribution
The study provides new insights into fracture risk after denosumab discontinuation and treatment adherence factors in osteoporosis patients.
Findings
Adherent and non-adherent patients had similar fracture risks after denosumab discontinuation.
Fractures may result from osteoporosis progression rather than a rebound effect from drug withdrawal.
Unscheduled treatment discontinuation should be avoided to manage osteoporosis effectively.
Abstract
To assess the prevalence of fragility fractures after denosumab discontinuation and to identify the factors affecting treatment adherence. We retrospectively reviewed the medical records of 3876 osteoporosis patients who were treated with denosumab at Trakya University Osteoporosis Clinic between 2015 and 2021. A total of 210 patients who received at least two regular doses of denosumab were eligible for inclusion. Patients were categorized as denosumab-adherent and denosumab-non-adherent. Adherence was defined as receiving the six-month scheduled dose with a maximum delay of up to eight weeks. Overall, 124 (59.05%) patients were denosumab-adherent and 86 patients (40.95%) were denosumab-non-adherent. New fragility fractures were identified in 32 patients: 17 in the denosumab-adherent group and 15 in the denosumab-non-adherent group. The groups did not significantly differ in the risk…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
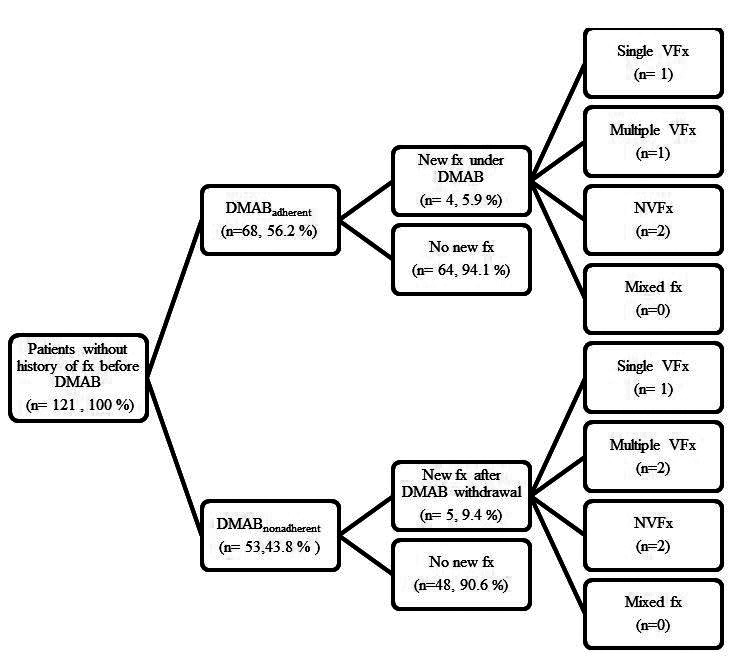 Figure 1
Figure 1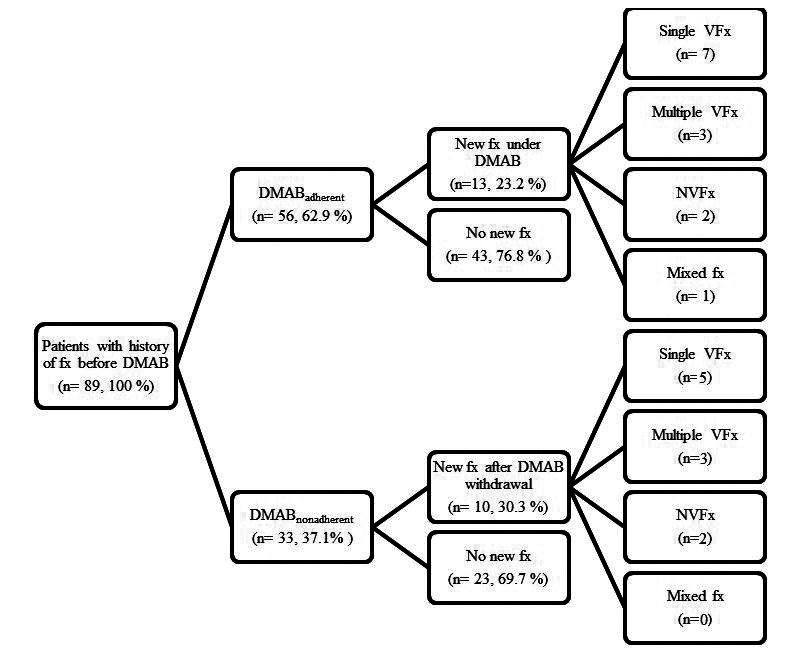 Figure 2
Figure 2| Total (n = 210) | DMAB-adherent (n = 124) | DMAB-non-adherent (n = 86) | ||
|---|---|---|---|---|
| Age (years), mean ± standard deviation (SD) | 69.44 ± 9.35 | 68.61 ± 9.49 | 70.63 ± 9.07 | 0.125 |
| Sex, n (%) |
|
|
| 1.000 |
| female | 207 (98.6) | 122 (98.4) | 85 (98.8) |
|
| male | 3 (1.4) | 2 (1.6) | 1 (1.2) |
|
| Age at menopause (years), mean ± SD | 45.81 ± 5.49 | 45.93 ± 5.61 | 45.64 ± 5.32 | 0.700 |
| Parity, median (min-max) | 2 (0-9) | 2 (0-6) | 2 (0-9) | 0.016 |
| Marital status, n (%) |
|
|
| 0.010 |
| married | 149 (71) | 95 (76.6) | 64 (62.8) |
|
| single | 14 (6.7) | 10 (8.1) | 4 (4.7) |
|
| widow | 47 (22.4) | 19 (15.3) | 28 (32.6) |
|
| Occupation, n (%) |
|
|
| 0.672 |
| housewife | 153 (72.9) | 88 (71) | 65 (75.6 |
|
| retired | 53 (25.2) | 33 (26.6) | 20 (23.3) |
|
| active working | 4 (1.9) | 3 (2.4) | 1 (1.2) |
|
| Height, mean ± SD | 155.77 ± 7.44 | 155.63 ± 7.37 | 155.97 ± 7.57 | 0.748 |
| Weight, mean ± SD | 67.05 ± 11.99 | 66.10 ± 11.78 | 68.41 ± 12.23 | 0.170 |
| BMI, mean ± SD | 27.90 ± 5.06 | 27.58 ± 4.97 | 28.51 ± 5.20 | 0.287 |
| Family history of fragility fracture, n (%) |
|
|
| 0.693 |
| yes | 46 (21.9) | 26 (21) | 20 (23.3) |
|
| no | 164 (78.1) | 98 (79) | 66 (76.7) |
|
| Fracture before DMAB, n (%) |
|
|
| 0.328 |
| yes | 89 (42.4) | 56 (45.2) | 33 (38.4) |
|
| no | 121 (57.6) | 68 (54.8) | 53 (61.6) |
|
| Comorbidities, n (%) |
|
|
|
|
| diabetes | 48 (22.9) | 29 (23.4) | 19 (22.1) | 0.826 |
| hypertension | 131 (62.4) | 76 (61.3) | 55 (64) | 0.695 |
| dyslipidemia | 26 (12.4) | 16 (12.9) | 10 (11.6) | 0.789 |
| hyperthyroidism | 4 (1.9) | 3 (2.4) | 1 (1.2) | 0.648 |
| hypothyroidism | 56 (26.7) | 35 (28.2) | 21 (24.4) | 0.540 |
| malignity | 62 (29.5) | 34 (27.4) | 28 (32.6) | 0.422 |
| Use of steroids, n (%) |
|
|
| 0.357 |
| yes | 22 (10.5) | 15 (12.1) | 7 (8.1) |
|
| no | 188 (89.5) | 109 (87.9) | 79 (91.9) |
|
| Smoking, n (%) |
|
|
| 0.533 |
| yes | 15 (7.1) | 10 (8.1) | 5 (5.8) |
|
| no | 195 (92.9) | 114 (91.9) | 81 (94.2) |
|
| Secondary osteoporosis, n (%) |
|
|
| 0.210 |
| yes | 111 (52.9) | 70 (56.5) | 41 (47.7) |
|
| no | 99 (47.1) | 54 (43.5) | 45 (52.3) |
|
| Tea consumption/d (cup), median (min-max) | 2 (0-20) | 2 (0-20) | 2 (0-10) | 0.501 |
| Coffee consumption/d (cup), median (min-max) | 1 (0-5) | 1 (0-5) | 1 (0-3) | 0.525 |
| Consumption of dairy products, n (%) |
|
|
| 0.144 |
| regular | 148 (70.5) | 81 (65.3) | 67 (77.9) |
|
| occasional | 59 (28.1) | 41 (33.1) | 18 (20.9) |
|
| never | 3 (1.4) | 2 (1.6) | 1 (1.2) |
| Total (n = 210) | DMAB-adherent (n = 124) | DMAB-non-adherent (n = 86) | ||
|---|---|---|---|---|
| Any therapy prior to DMAB, n (%) |
|
|
| 0.209 |
| yes | 135 (64.3) | 84 (67.7) | 51 (59.3) |
|
| no | 75 (35.7) | 40 (32.3) | 35 (40.7) |
|
| Treatment agent prior to DMAB, n (%) |
|
|
|
|
| oral bisphosphonate. | 107 (51) | 68 (54.8) | 39 (45.3) | 0.684 |
| IV bisphosphonate. | 34 (16.2) | 24 (19.4) | 10 (11.6) | 0.097 |
| strontium | 22 (10.5) | 14 (11.3) | 8 (9.3) | 0.742 |
| teriparatide | 5 (2.4) | 2 (1.6) | 3 (3.5) | 0.381 |
| Number of DMAB injections (median, min-max) | 4 (2-13) | 6 (2-13) | 4 (2-10) | <0.001 |
| Duration of DMAB discontinuation, (months; median, min-max) | - | - | 23 (2-70) | - |
| Reason for DMAB discontinuation, n (%) | - | - |
| - |
| COVID pandemic |
|
| 61 (70.9) |
|
| comorbidities |
|
| 3 (3.5) |
|
| side effects |
|
| 0 (0) |
|
| other | 22 (25.6) |
| Patient | Age | BMI | Sex | Site of new fracture after DMAB withdrawal | Family history of hip fracture | Comorbidities | Prior therapy | Number of DMAB injections | Duration of DMAB withdrawal (months) at evaluation | Reason of DMAB withdrawal | Pre-DMAB fracture | Pre-DMAB DXA T-score | Pre- DMAB DXA BMD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1† | 85 | 28.9 | F | L4 | - | diabetes
hypertension
breast cancer
Alzheimer | - | 2 | 44 | pandemic | major: 18
hip: 6.2 | L1-L4: −0.1
DF:-2.7 | L1-L4: 1.03
DF: 0.42 |
| 2 | 75 | 36.4 | F | calcaneus | + | diabetes
hypertension
dyslipidemia
breast cancer (use of letrozole) | - | 2 | 45 | pandemic | major: 19
hip: 5.5 | L1-L4: −1.6
FN: −2.34 | L1-L4: 0.869
FN: 0.586 |
| 3 | 62 | 27.1 | F | distal radius | - | diabetes
thyroid papilary cancer (hypothyroidism) | 10 y of Aledronate | 3 | 14 | pandemic | major: 3.6
hip: 0 | L1-L4: −3.5
FN: 1.3 | L1-L4: 0.654
FN: 1.051 |
| 4 | 60 | 24.6 | F | T12, L2, L4 | - | rheumatoid arthritis
(use of methotrexate and prednisolone) | - | 4 | 10 | pandemic | major: 13
hip: 2.8 | L1-L4: −3.7
FN: −2.0 | L1-L4: 0.644
FN: 0. 630 |
| 5 | 82 | 20.4 | F | T9, T12 | - | hypertension CML (use of imatinib) | - | 4 | 36 | pandemic | major: 11 hip: 5.4 | L1-L4: −4.5 FN: −2.6 | L1-L4: 0.550 FN: 0.556 |
| Patient | Age | BMI | Sex | Site of previous fracture | Any fracture under DMAB | Site of new fracture after DMAB withdrawal | Family history of hip fracture | Comorbidities | Prior therapy | Number of DMAB injections | Duration of DMAB withdrawal (months) at evaluation | Reason of DMAB withdrawal | Pre-DMAB fracture | Pre-DMAB DXA T-score | Pre-DMAB DXA BMD |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 86 | 21.4 | F | T12, L2 | T7, T8, T9, T10 | T6 | - | hypertension | - | 6 | 7 | pandemic | major: 44
hip: 28 | L1-L4: −3.1
FN: −4.4 | L1-L4: 0.707
FN: 0.364 |
| 2 | 86 | 27.3 | F | metacarpal,
distal radius | - | T12, L1, L4, L5 | + | hypertension
hyperthyroidism | - | 3 | 15 | pandemic | major: 74
hip: 69 | L1-L4: −4.0
FN: −4.5 | L1-L4: 0.607
FN: 0.346 |
| 3 | 52 | 30 | F | L1 | - | T8 | + | diabetes
hypertension
dyslipidemia
hypothyroidism | 1 y
zoledronate | 3 | 16 | pandemic | major: 13
hip: 0.6 | L1-L4: −2.6
FN: −1.2 | L1-L4: 0.75
FN: 0.71 |
| 4 | 83 | 18.2 | F | T8,T9 | - | T7 | - | diabetes | 1.5 y
teriparatide | 3 | 19 | pandemic | major: 14
hip: 3.8 | L1-L4: −4.1
FN: −1.8 | L1-L4: 0.599
FN: 0.648 |
| 5 | 66 | 28.1 | F | distal radius | - | distal radius | - | endometrium
cancer | 1 y
aledronate | 5 | 15 | personal preference | major: 21
hip: 8.3 | L1-L4: −3.6
FN: −3.1 | L1-L4: 0.65
FN: 0.50 |
| 6 | 62 | 33.3 | F | femoral neck, T11, T12 | - | L1,L2,L3,L4,L5 | - | hypertension
hypothyroidism | 5 y
aledronate | 4 | 22 | pandemic | major: 20
hip: 7.7 | L1-L4: −1.9
FN: −3.1 | L1-L4: 0.983
FN: 0.613 |
| 7 | 70 | 24.1 | F | metatarsal,
distal radius | - | T6 | + | - | - | 3 | 23 | pandemic | major: 12
hip: 0.9 | L1-L4: −2.5
FN: −0.8 | L1-L4: 0.768
FN: 0.759 |
| 8 | 71 | 27.6 | F | T10, T11, T12,
L1, L2, L3,
L4, L5 | - | T8, T9 | - | hypertension
SLE (long term steroid use)
>30 packs/y of cigarettes
bypass surgery | - | 2 | 24 | pandemic | major: 56
hip: 39 | L1-L4: −0.9
FN: −3.6 | L1-L4: 0.951
FN: 0.447 |
| 9 | 79 | 26.7 | F | L1 | - | T8 | - | diabetes
hypertension
hypothyroidism
atrial fibrillation
heart failure | 8 y
aledronate | 2 | 32 | pandemic | major: 30
hip: 12 | L1-L4: −3.6
FN: −3.2 | L1-L4: 0.654
FN: 0.497 |
| 10 | 69 | 31.2 | F | T7, L3, L4, L5 | T5 | ankle | - | hypertension breast cancer (use of tamoxifen) heart failure renal failure hepatitis B carrier | 3 y aldronate, 1 y zoledronate | 8 | 10 | pandemic | major: 14 hip: 2.3 | L1-L4: −1.3 FN: −1.9 | L1-L4: 0.90 FN: 0.63 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and osteoporosis research · Bone health and treatments · Pharmacological Effects and Toxicity Studies
Denosumab is a novel anti-resorptive agent associated with a low incidence of fractures and a low rate of adverse events. It produces a continued increase in bone mineral density (BMD) that does not plateau for up to 10 years (1). However, its potent anti-resorptive effects reverse rapidly upon treatment cessation, a phenomenon referred to as the “rebound effect” (2,3).
Besides the rebound effect following denosumab discontinuation, fragility fractures may also arise as a result of the natural progression of osteoporosis, particularly in patients at high risk for fractures. Research on this topic remains limited, and the reports show conflicting results regarding the timing, number, and location of rebound fractures. This study aimed to assess the prevalence of fragility fractures in patients who discontinued denosumab therapy for any reason and to identify the factors influencing treatment adherence.
PATIENTS AND METHODS
Study design and patient population
This retrospective study was conducted at the Department of Physical Medicine and Rehabilitation and the Department of Endocrinology of Trakya University between December 2022 and April 2023. The study protocol was approved by the Science Research Ethics Committee of Trakya University Faculty of Medicine. Patient consent was waived due to the retrospective design of the study. The study was registered at ClinicalTrials.gov (ID: NCT06414616) and adhered to the principles of the World Medical Association Declaration of Helsinki.
The electronic medical records of patients who started denosumab (Prolia®) therapy between 2015 and 2021 were retrospectively evaluated. The inclusion criteria were as follows: 1) having received at least two consecutive doses (60 mg subcutaneously) of denosumab, with an interval of fewer than 8 months between the doses (as it is a minimum dosage to observe the anti-fracture effects of the medication) (4); 2) having had at least one radiological image of the lumbar and thoracic spine taken before the initiation of denosumab 3) having BMD and T-score assessed using dual-energy x-ray absorptiometry, and having fracture risk assessment tool scores calculated before the initiation of denosumab. Exclusion criteria were 1) fractures due to cancer, trauma, or Paget’s disease; 2) monthly denosumab injections to prevent bone metastasis; 3) age under 18 years, pregnancy, and premenopause.
We recorded data on age, sex, age at menopause, parity, marital status, occupation, height, weight, body mass index (BMI), family history of fragility fractures, the presence of baseline fragility fractures, comorbidities, use of steroids, smoking status, the presence of secondary osteoporosis, tea/coffee/alcohol consumption, the intake of dairy products, any previous osteoporosis therapy, the treatment agent used before denosumab, the number of denosumab injections received, the duration of denosumab withdrawal, and the reason for denosumab discontinuation.
Radiological images were examined to determine whether any fractures were present before, during, or after denosumab treatment. The number and location of the fractures were recorded. The number of denosumab doses administered was determined by reviewing the hospital’s electronic prescription and medical records.
Patients who missed the injections for more than two months were classified as denosumab-non-adherent, while those who received their injections regularly were classified as denosumab-adherent. An increased risk of vertebral fractures (VFx) has been reported as early as 4-8 weeks after a missed injection (5,6). In the current study, adherence was defined as receiving a scheduled six-month dose with a maximum delay of up to eight weeks, consistent with previous studies (7,8). This definition is based on the observation that multiple VFx are often reported 2-10 months after a delay in the dosing schedule (9).
The duration of the off-treatment period after denosumab discontinuation was calculated as the interval between six months after the last injection and the patient’s admission date. Patients in the denosumab-non-adherent group did not receive any alternative osteoporosis treatment during the off-treatment period. We also determined the differences in clinical features between patients with and without a history of fractures before starting denosumab.
Study outcomes
The primary outcome was the prevalence of new fragility fractures, including single or multiple VFx and non-vertebral fractures (NVFx) (any fragility fractures such as hip fractures), as defined radiologically. Hip fractures were classified as those occurring in the femoral neck, intertrochanteric region, or subtrochanteric region (4). Vertebral compression fractures were defined according to the Genant classification as at least a 20% reduction in the height of any of the anterior, middle, or posterior aspects of a vertebra compared with the height of the nearest normal vertebra. Multiple VFx were defined as two or more VFx (10). The secondary outcome was the exploration of factors that may influence denosumab adherence or non-adherence.
Statistical analysis
Continuous variables were summarized as means and standard deviations (SD), and categorical variables as frequencies and percentages. The normality of distribution was tested with a Shapiro-Wilk test. Differences between the groups in continuous variables were assessed with a t test, while differences in categorical variables were assessed with a Pearson χ^2^ test. Two-tailed P values lower than 0.05 were considered significant. Statistical analysis was performed with SPSS Statistics 23.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Participant characteristics
The medical records of 3876 patients who started denosumab therapy between 2015 and 2021 were reviewed. A total of 210 patients were eligible for inclusion: 207 postmenopausal women (98.6%) and 3 men (1.4%). The mean age was 69.44 ± 9.35 years. The most commonly observed comorbidities were hypertension (62.4%) and malignancy (29.5%). Baseline fragility fractures before the initiation of denosumab therapy were present in 89/210 patients (42.4%). A total of 135/210 patients (64.3%) had a history of osteoporosis medication use, with 107/210 (51%) having a history of oral bisphosphonate use. Participants received a median of 4 denosumab injections (range 2-13).
Adherence to denosumab therapy
Out of 210 patients, 124 (59.05%) were adherent and 86 (40.95%) were non-adherent to denosumab. Most of the baseline demographic and clinical characteristics were similar between the groups (Table 1), but the denosumab-non-adherent group had significantly higher parity (P = 0.016) and widowhood rates (P = 0.010). The denosumab-adherent group had significantly more administered denosumab doses (P < 0.001). None of the patients reported alcohol consumption.
The most common reason for denosumab discontinuation (61/86 non-adherent patients; 70.9%) was the COVID-19 pandemic. No adverse events were reported. Twenty-two out of the 86 patients (25.6%) reported other reasons for discontinuation, such as forgetting the appointment (n = 4) or preferring not to attend (n = 18) (Table 2).
Vertebral and non-vertebral fractures
New fragility fractures were detected in 32 patients. Among these, 17 patients in the denosumab-adherent group developed new fractures while on denosumab treatment, and 15 patients in the denosumab-non-adherent group developed new fractures during the off-treatment period (22 VFx in 11 patients and 4 NVFx in 4 patients).
In patients without a history of fractures before initiating denosumab (n = 121), the prevalence of new fragility fractures was 5.9% (n = 4) in the denosumab-adherent group and 9.4% (n = 5) in the denosumab-non-adherent group (Figure 1). In this subset of patients, the denosumab-adherent and denosumab-non-adherent groups did not significantly differ in the risk of new fracture development (risk ratio [RR] = 0.624; 95% confidence interval [CI] 0.176-2.209, P = 0.464). They also did not significantly differ in the risk of single VFx (RR = 1.327, 95% CI 0.085-20.687, P = 0.840), multiple VFx (RR = 2.600, 95% CI 0.243-27.869, P = 0.4298), or NVFx (RR = 1.320, 95% CI 0.193-9.051, P = 0.777).
Compliance rates and fracture prevalence in patients without a history of fracture before the initiation of denosumab (DMAB). Fx – fracture, VFx – vertebral fracture, NVFx – non-vertebral fracture, mixed fx – a combination of VFx and NVFx.
In patients with a history of fractures before initiating denosumab (n = 89), the prevalence of new fragility fractures was 23.2% (n = 13) in the denosumab-adherent group and 30.3% (n = 10) in the denosumab-non-adherent group (Figure 2). In this subset of patients, the denosumab-adherent and denosumab-non-adherent groups did not significantly differ in the risk of new fracture development (RR = 0.766, 95% CI 0.379-1.548, P = 0.458). They also did not significantly differ in the risk of single VFx (RR = 1.276, 95% CI 0.446-3.646, P = 0.650), multiple VFx (RR = 1.769, 95% CI 0.385-8.141, P = 0.464), NVFx (RR = 1.800, 95% CI 0.270-12.011, P = 0.544), or mixed fractures (RR = 0.625, 95% CI 0.026-14.763, P = 0.770). No significant difference was observed in the prevalence of new fragility fractures in patients without a fracture history (RR = 0.624) and those with a previous fracture history (RR = 0.766; P = 0.780).
Compliance rates and fracture prevalence in patients with a history of fracture before the initiation of denosumab (DMAB). Fx – fracture, VFx – vertebral fracture, NVFx – non-vertebral fracture, mixed fx – a combination of VFx and NVFx.
The characteristics of patients who sustained fractures after denosumab withdrawal
Five patients without a history of fractures before denosumab treatment developed new fractures after discontinuation. All were postmenopausal women. The most common fracture site was the vertebra, with multiple VFx observed in 2 patients. No cases of mixed fractures (both VFx and NVFx) were reported. Among the 5 patients, 4 had a history of malignancy and 1 had rheumatoid arthritis with long-term corticosteroid use. Only 1 patient had a family history of hip fracture, and 1 patient had a history of bisphosphonate use. No fractures occurred during denosumab treatment. The number of denosumab administered doses ranged from 2 to 4 (Table 3).
Ten patients with a history of fractures before initiating denosumab developed new fractures after denosumab discontinuation. All were postmenopausal women. The most common site of fracture was the vertebra, with multiple VFx observed in 3 patients. No cases of mixed fractures were reported. Among 10 patients, 2 had a history of malignancy and 1 had systemic lupus erythematosus with long-term corticosteroid use. Three patients had a family history of hip fracture. Five patients had previously used bisphosphonate, and 1 had used teriparatide. Additionally, 2 patients had developed fractures during denosumab treatment. The number of administered denosumab doses ranged from 2 to 8 (Table 4).
DISCUSSION
In this study, the prevalence and type of new fractures were similar between denosumab-adherent and non-adherent patients, regardless of their history of fragility fractures. Additionally, nearly 41% of osteoporosis patients discontinued denosumab for over two months due to various reasons, primarily the COVID-19 pandemic. These patients were more likely to have higher parity or be widowed.
Contrary to expectations, the history of fractures did not significantly affect the risk of new fractures following denosumab discontinuation. Similar to our findings, Miller et al (11) did not observe an increased fracture incidence among the small number of patients who discontinued denosumab in their study. In a study by Bone et al (2), the incidence of clinical fractures 24 months after denosumab discontinuation was similar to that in the placebo group. Brown et al (12) also found no excess of fractures after denosumab discontinuation compared with placebo during the off-treatment period for up to 24 months.
Although several reports indicated an increased risk of VFx in non-persistent denosumab users (5,13-16), the risk of rebound fractures after denosumab discontinuation remains unclear. Many studies have shown that the risk of VFx significantly increases following denosumab discontinuation. These findings can be explained by the hypothesis that trabecular bone, being more rapidly affected by increased bone turnover, is more vulnerable than cortical bone (9,13,17). Conversely, a recent study found that any fractures, including hip fractures and multiple VFx, occurred more frequently in patients who discontinued denosumab compared with persistent users (18). The precise contribution of rebound phenomenon vs the natural progression of osteoporosis in high fracture-risk patients remains uncertain, which suggests that the return to the pretreatment fracture risk cannot be attributed solely to the rebound phenomenon (19). The risk factors for VFx after denosumab discontinuation include a history of VFx (12,20), longer duration of denosumab treatment (9,21), greater BMD loss (20), and the use of aromatase inhibitors (9,22). The rebound effect is not induced by a single denosumab dose (12,23), but it becomes more pronounced with an increased number of doses (24). Greater BMD gain during treatment corresponds to greater BMD loss upon discontinuation (25). Conversely, other studies reported that BMD response (26) and VFx incidence (20) were not related to the duration of denosumab treatment. Everts-Graber et al (27) associated greater BMD loss after denosumab withdrawal with younger age, lower BMI, longer denosumab therapy, and a lack of prior antiresorptive treatment, while Tripto-Shkolnik et al (18) found no association between prior bisphosphonate use and a reduced fracture risk following denosumab discontinuation. In our study, the risk of developing any type of fracture was not significantly increased following denosumab discontinuation. Furthermore, patients who experienced new fractures after denosumab discontinuation frequently used glucocorticoids and had an inflammatory disease and/or malignancy.
Modi et al reported that 48.8% and 64.3% of patients discontinued denosumab at 12 and 24 months, respectively (28). In our study, the discontinuation rate was 41%. However, since the primary reason for non-adherence was the COVID-19 pandemic, this rate may not represent non-pandemic circumstances. Although, in Turkey, hospital access was officially permitted during the pandemic, the government-imposed curfew for individuals over the age of 65, who represent the majority of patients receiving denosumab, may have prevented some patients from attending follow-up visits. A recent study from Japan has also reported a significant increase in postponed denosumab treatment during the pandemic (29).
Patients with multiple comorbidities are commonly believed to have lower medication compliance. However, in our study, the level of comorbidity was similar between the groups, consistent with previous findings (30). Additionally, adherence to denosumab was not influenced by age, BMI, the age at menopause, or occupation. The most significant factors affecting treatment compliance were high parity and widowhood. This may be attributed to the increased social and economic burdens associated with multiple childbirths. Additionally, the loss of a spouse may lead to the absence of reminder mechanisms for medication intake and a declined motivation for managing one’s health. Although previous studies suggested that patients with prior osteoporosis treatment were more adherent than treatment-naive patients (31), we did not find a significant difference in adherence rates between these groups.
The strengths of the study include reliable data collection due to our center’s extensive archive, including a fracture liaison service (FLS). FLS allows electronical recording of denosumab injections administered by an FLS nurse at the outpatient clinic, which eliminates any doubt regarding whether the patient withdrew medication from the pharmacy. Additionally, analyzing multiple VFx as a separate entity adds strength to the study. However, certain limitations should be considered. First, this study was a small, retrospective, and single-center analysis, which inherently limits the generalizability of the findings and may introduce selection bias or unmeasured confounding. Although we attempted to minimize selection bias by systematically reviewing all patient records for eligibility, we might not have been able to comprehensively control for all potential confounding factors. Second, since the study population primarily consisted of postmenopausal osteoporosis patients, the results may not be generalizable to all osteoporosis patients. Third, we were not able to reliably establish the exact timing of fractures due to missed follow-up visits during the pandemic, which precluded us from performing a detailed time-to-event analysis. Fourth, we did not assess BMD as a measure of therapeutic effect. Finally, as the data largely reflect the early post-pandemic period, our findings may underestimate denosumab adherence rates compared with regular health care periods. However, it is unlikely that the risk of new fracture development following denosumab discontinuation was significantly over- or underestimated.
In conclusion, our results indicate that although fractures after denosumab discontinuation may be attributed to the rebound effect, some may occur due to the inherent nature of osteoporosis. Nonetheless, our findings do not imply that discontinuing denosumab without subsequent therapy is safe, and unscheduled treatment discontinuation must be prevented.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bone HG Wagman RB Brandi ML Brown JP Chapurlat R Cummings SR 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol 2017 5 513 23 10.1016/S 2213-8587(17)30138-9 28546097 · doi ↗ · pubmed ↗
- 2Bone HG Bolognese MA Yuen CK Kendler DL Miller PD Yang YC Effects of denosumab treatment and discontinuation on bone mineral density and bone turnover markers in postmenopausal women with low bone mass. J Clin Endocrinol Metab 2011 96 972 80 10.1210/jc.2010-1502 21289258 · doi ↗ · pubmed ↗
- 3Tsourdi E Zillikens MC Certainties and uncertainties about denosumab discontinuation. Calcif Tissue Int 2018 103 1 4 10.1007/s 00223-018-0436-y 29926143 · doi ↗ · pubmed ↗
- 4Cummings SR San Martin J Mc Clung MR Siris ES Eastell R Reid IR Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 2009 361 756 65 10.1056/NEJ Moa 0809493 19671655 · doi ↗ · pubmed ↗
- 5Anastasilakis AD Evangelatos G Makras P Iliopoulos A Rebound-associated vertebral fractures may occur in sequential time points following denosumab discontinuation: need for prompt treatment re-initiation. Bone Rep 2020 12 100267 10.1016/j.bonr.2020.100267 32373677 PMC 7191536 · doi ↗ · pubmed ↗
- 6Sosa-Henriquez M Torregrosa O Deniz A Saavedra P Ortego N Turrion A Multiple vertebral fractures after suspension of denosumab. A series of 56 cases. Int J Clin Pract 2021 75 e 14550 10.1111/ijcp.14550 34145944 · doi ↗ · pubmed ↗
- 7Silverman SL Siris E Belazi D Recknor C Papaioannou A Brown JP Persistence at 24 months with denosumab among postmenopausal women with osteoporosis: results of a prospective cohort study. Arch Osteoporos 2018 13 85 10.1007/s 11657-018-0491-z 30088189 PMC 6096691 · doi ↗ · pubmed ↗
- 8Karlsson L Lundkvist J Psachoulia E Intorcia M Strom O Persistence with denosumab and persistence with oral bisphosphonates for the treatment of postmenopausal osteoporosis: a retrospective, observational study, and a meta-analysis. Osteoporos Int 2015 26 2401 11 10.1007/s 00198-015-3253-4 26282229 PMC 4575381 · doi ↗ · pubmed ↗