Pediatric eye movement-based perimetry: progress, pitfalls, and prospects
Anna Boethun, Sarah Linea von Holstein, René Mathiasen, Miriam Kolko, Frans W. Cornelissen, Jeroen Goossens, Barbara Johanne Thomas Nordhjem

TL;DR
Eye movement-based perimetry is a promising method for assessing vision in children, but faces challenges like poor ergonomics and calibration issues that need to be addressed for reliable clinical use.
Contribution
The paper identifies practical barriers in pediatric eye movement-based perimetry and proposes solutions based on clinical and technological insights.
Findings
Commercially available EMP systems often face poor ergonomic fit and inadequate calibration in children.
Attention management strategies are lacking, leading to incomplete tests and data loss.
Collaboration between clinicians, engineers, and scientists is needed to improve EMP for pediatric use.
Abstract
Eye movement-based perimetry (EMP) is a promising, non-invasive approach for visual field assessment, particularly in pediatric populations where standard automated perimetry often fails. However, completion rates in prior pediatric EMP studies have ranged from 41 to 81%, and reasons for unsuccessful testing are seldom reported. In this perspective article, we aim to highlight practical barriers and design gaps in EMP systems for children, with a focus on clinical use. From our clinical experience with testing two commercially available EMP systems in children (21 patients with brain tumors and 19 age-matched controls), we observed recurring challenges, including poor ergonomic fit, inadequate calibration of eye tracker, and insufficient attention management strategies. These issues frequently led to data loss and incomplete tests, underscoring the gap between current technology and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
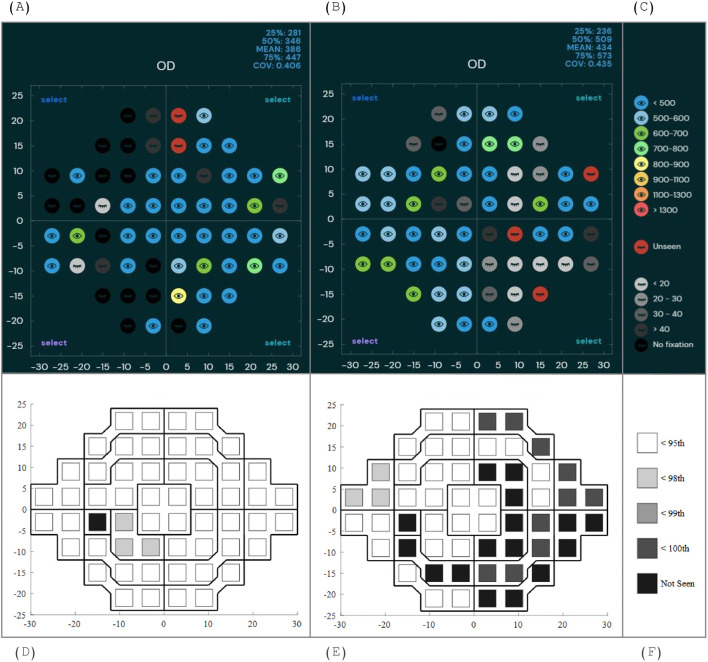 Figure 1
Figure 1| Info | BulbiCAM | SONDA |
|---|---|---|
| System Type | Haploscope with integrated eye tracker and +6 lenses placed between eye and virtual image; Software run via accompanying PC | Standardized oculomotor assessment platform (monitor, wearable tracker, companion device (smart phone) and accompanying PC) |
| Eye Tracker Specs | Glint based; 400 Hz (alternating 200 Hz bright pupil/200 Hz dark pupil glint); effective 200 Hz | Video-based; 120 Hz; head-mounted (Pupil Labs Pupil Invisible) |
| Monitor specs | 14.7 cm viewing distance, screen dimensions: 121x68 mm, 60 Hz monitor refresh rate | 60 cm viewing distance, screen dimensions: 598x336 mm, 60 Hz monitor refresh rate |
| Mounting Options | Ceiling or desk mount (desk-mounted used in study) | Monitor on height-adjustable table with chinrest |
| Calibration | None required (fixation assumed to align with target at start of each trial) | Calibration-free (deep learning-based analysis); uses screen detection for head movement correction |
| Fixation Target | Green, moves smoothly 4 times (center: all corners) to sample different field locations, present at all times | See “stimulus details” |
| Stimulus Details | White stimuli, Goldmann III4e equivalent, on gray (10 cd/m²) background; three intensity onsets (instant, logarithmic, linear; instant used) | Moving Gaussian blob (0.43°, Goldmann III, peak 42 cd/m²) on gray background (30 cd/m²) |
| Visual Field Protocol | 60 points per eye, covering central ±30° (standard protocol). | 56 points peer eye (24–2 standard pattern + two points) via smooth pursuit and step/jump to new locations. |
| Testing time | 2 to 4 minutes per eye (depending on performance). | 4x40 seconds per eye. |
| Participant Instructions | “Look at the green dot, when you see a white dot look at that and then look back at the green dot” | “Follow the white dot with your eyes” |
| Requirements to show stimulus | Gaze within a 5-pixel radius circle (eye coordinates) for ≥300 ms within 3 seconds prior to stimulus onset; if not met, stimulus not displayed and position marked as “no fixation” (black). | None |
| Definition ‘Seen’/’Unseen’ | “Seen” if gaze moves ±30° toward stimulus 120–1200 ms after onset and subsequent fixation detected (63 ms, gaze within 1.5 px radius circle); otherwise “unseen” (red in plot) or by distance measure (Euclidean distance from target-stimulus vector; gray scale in plot) | “Seen” if saccade (gaze velocity 30 deg/s or gaze acceleration 175 deg/s2) starts within 8° of pre-jump stimulus position and ends within 8° of post-jump stimulus position; otherwise “Unseen” |
| Response Time Mapping | Color coding based on latency (time to leave fixation area after stimulus onset) | Grayscale coding by SRT quartiles compared to adult, normative data |
| Retesting | Locations marked as “no fixation” or “unseen” retested once | None |
| Manual Review | Examiner review and exclude falsely categorized “seen” responses | None |
| Other Analysis | None | Machine learning based analysis of Spatiotemporal properties (not performed in current study due to small sample size) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Visual Impairment Studies · Gaze Tracking and Assistive Technology · Retinopathy of Prematurity Studies
Introduction
1
Visual field examination is a cornerstone of diagnosing and managing ophthalmological and neurological disorders. Visual field defects (VFDs) can indicate serious conditions such as retinal disorders, optic neuropathies, or brain tumors (1–3). Early detection and monitoring are essential for timely and appropriate intervention, especially in children (4), where preserving visual function is critical for development and quality of life.
In pediatric patients, reliable visual field assessment is especially important, as some serious conditions initially present through visual complaints (5). For instance, 10-20% of children with brain tumors exhibit VFDs (5, 6) and in some cases this is the only sign of disease. The true prevalence of VFDs in this population is likely higher, but due to limitations in current testing methods, many defects remain undetected (7). This underscores the need for more effective approaches to pediatric visual field assessment.
Traditional perimetric methods, such as Tangent Screen Campimetry, Goldmann Visual Fields (GVF), Frequency Doubling Technology (FDT) and Standard Automated Perimetry (SAP), provide detailed assessments of visual field sensitivity but rely on sustained fixation and manual responses. These cognitive and motor demands make them less suitable for young children. While SAP has been tested in children as young as 5 years old, results are typically unreliable under age 6-7 (8–12), with slightly better outcomes reported only in selected healthy cohorts (13). Notably, none of these studies included children with neurological impairment or visual field defects. Children with these conditions are likely to be at a further disadvantage. Reliability is even lower with other paradigms, with semi-automated kinetic perimetry (Octopus 900) reliable only from around age 11 (14), and FDT from age 8–9 in healthy children (15, 16). GVF, though lacking automated reliability indices, produces acceptable results from age 7–8 (17, 18) and is often preferred under age 9 when compared to SAP and Octopus paradigms (19). Simpler alternatives like confrontational testing are quick and easy to administer but lack sensitivity and rely on examiner skills, limiting their value for follow-up (20).
Eye movement-based perimetry (EMP) offers a promising alternative, leveraging the reflexive saccade: a rapid, automatic eye movement towards a suddenly appearing stimulus in the peripheral visual field (also referred to as visual grasp reflex or exogenous saccade) (21, 22). This instinctive gaze shift is conceptually similar to the response observed in preferential looking paradigms, widely used to assess visual function in infants and toddlers. In some EMP systems, the saccadic movement simply substitutes the manual response (23), while others quantify saccadic reaction time (SRT) - the latency from stimulus onset to saccade initiation - as a proxy for visual field sensitivity (24, 25). In adult cohorts, EMP has demonstrated feasibility and diagnostic value in glaucoma as well as various neurological disorders (23, 26, 27). EMP has also been tested in both healthy and visually impaired children, with varying degrees of success (28–34). Across pediatric EMP studies, a consistently high proportion of children, ranging from 41% to 81%, remain partially tested or untested.
Numerous EMP devices are currently under development, most targeting glaucomatous visual field loss in adults. Prior studies have shown that these methods are more intuitive and easier for adults to perform than traditional SAP (23, 35). Our objective was to determine whether systems originally developed for adults (adult systems) can also be used to examine children. We selected two European eye-tracking systems for evaluation in 4-18-year-olds: BulbiCAM (36) (BulbiTech AS, Trondheim, Norway), which mimics SAP with a static-grid paradigm, and SONDA (37) (the Standardized Oculomotor Neuro-ophthalmic Disorders Assessment; Reyedar, Groningen, The Netherlands), which relies on continuous tracking of a moving target.
Translating EMP to pediatric use introduces unique challenges: children’s limited comprehension and attention, physical constraints, and immature visual and oculomotor systems complicate direct application of adult setups. In this perspective article, we describe pitfalls and usability issues when testing BulbiCAM and SONDA in a pediatric cohort. We present practical lessons and recommendations to support improved EMP implementation for children.
Description of two adult systems
2
The technical specifications and EMP paradigms for BulbiCAM and SONDA are provided in Table 1, including mounting options, calibration requirements, stimulus properties, and the criteria for visual field assessment. The standard output of BulbiCAM and SONDA is shown in Figure 1.
Visual field plots from one patient (9-year-old with temporal hemianopia) and one age-matched control. (A). healthy control tested with BulbiCAM, (B). patient tested with BulbiCAM, (C). labels, numbers ranging from 500 to 1300 indicate saccadic reaction time in ms, (D). healthy control (SONDA), (E). patient (SONDA), (F). labels, numbers indicate SRT-percentile.
Clinical experience and testing context
3
Our experience using BulbiCAM and SONDA is informed by EMP testing in 21 patients aged 4–18 years diagnosed with a brain tumor and 19 age-matched healthy controls. Patients were recruited from the Department of Ophthalmology, Rigshospitalet, Copenhagen, between March 15, 2023, and September 31, 2024, following referral by the treating pediatric ophthalmologist. Healthy controls were recruited through the authors’ personal networks and were excluded if they had a history of ophthalmic/neurologic disease or abnormal findings upon ophthalmic examination. The EMP testing was conducted in a dimly lit examination room at the Department of Ophthalmology, Rigshospitalet, Copenhagen. All examinations were conducted by staff experienced in pediatric ophthalmic testing.
The BulbiCAM was placed on a height-adjustable table and adapted to each child, allowing for either seated or standing testing. Bulbitech provided custom face pieces for smaller head sizes, along with a stable mounting base. These face pieces were secured to the child’s head using an elastic band and then magnetically attached to the haploscope to reduce head movements. The test was operated through a user-interface (BulbiHUB).
The SONDA setup comprised a monitor mounted on a height-adjustable table with an attached chinrest. If necessary, the child’s head was gently held in place by the examiner to minimize movement. Children were seated in a height-adjustable chair. The eye tracker was connected to a mobile device, which was linked to a laptop. The SONDA test was operated through the Ubuntu terminal.
Main issues encountered
4
EMP in children presents age-specific challenges across hardware, testing procedures, and data interpretation. Below, we outline the main problem areas in four sections:
Hardware and ergonomics
4.1
Eye tracker hardware
4.1.1
Most eye-tracking equipment is designed with adult users in mind, which poses challenges in pediatric applications. The head-mounted eye tracker used with SONDA was only available in an adult-size at the time of testing, resulting in slippage, despite the use of two elastic bands for stabilization. Reyedar now offers a child-size wearable eye tracker (Pupil Labs GmbH Neon) for use with SONDA.
Similarly, BulbiCAM requires a head strap to minimize movement, but younger children found this setup distressing. As a result, testing in these cases was conducted without the head strap, which may have allowed minor head movements during data collection.
Seating and mobility
4.1.2
Room furnishings must accommodate all body sizes and mobility needs. The standard ophthalmic chin rest used with the SONDA setup was too tall for smaller children, increasing head movements due to poor headband reach. Similarly, tables and chairs are often too large and not easily adjustable or movable for wheelchair users. Ensuring that children feel comfortable and safe during testing is essential, which includes offering the choice to remain in their own wheelchair or sit on a parent’s lap. In one case, a wheelchair-using child was unable to get close enough to the screen for reliable eye tracking. Tschopp et al. (8) addressed these challenges by using a custom pediatric chair.
Tracking and calibration
4.2
Pupil detection
4.2.1
In our initial BulbiCAM trials, many children’s eyes were untrackable. Similar issues have previously been described in the literature and might be explained by watery eyes and large pupils that complicate glint and pupil detection, leading to intermittent data loss (38, 39). Tobii (another eye tracking manufacturer) even launched a specific illumination mode specifically designed for tracking infants’ gaze (40). We found that reducing the IR diode output solved the issue, although this is not a user-accessible setting.
Algorithmic bias
4.2.2
Video-oculography systems like the Pupil Labs Invisible used with SONDA rely on machine learning algorithms trained exclusively on healthy adult data (41, 42). This may introduce inaccuracies in pediatric as well as clinical populations. Although gaze estimates appeared broadly plausible, formal pediatric validation is needed. Retraining the algorithms on pediatric data could further improve accuracy.
Calibration trade-offs
4.2.3
Traditional multi-point calibration requires comprehension, cooperation, and sustained attention, which is often challenging in children (28, 32). Both SONDA and BulbiCAM sidestep this procedure: SONDA uses the calibration-free Pupil Invisible eye tracker, while BulbiCAM uses an uncalibrated eye tracker in combination with task adaptations and assumptions about fixation position. The benefit is speed - but at the cost of potentially imprecise or even inaccurate gaze estimations, limiting accurate localization of responses within the visual field.
Stimulus design and attention management
4.3
Test duration and breaks
4.3.1
Incomplete tests were common in our cohort and have also been reported in other pediatric visual field studies (8, 28), highlighting the need for pause options in this population. Both systems used in our study lack pause buttons to accommodate breaks, which is a limitation given children’s limited attention spans.
SONDA partially mitigates this issue by dividing the test into four trials, each lasting ~40 seconds, thereby allowing for three short breaks per eye. However, this structure has a critical limitation: interrupted trials or incomplete tests cannot be analyzed, which reduces its robustness in less cooperative or fatigued participants.
BulbiCAM requires a single uninterrupted session per eye. Although this increases the demand on the participant, unfinished tests can still be analyzed, providing greater flexibility. Additionally, Bulbitech offers shorter paradigms with 16 or 26 test points. However, the current design tests one quadrant in its entirety before proceeding to the next, which increases the risk of a quadrant being affected by temporary inattention. If a pause function was added, the sequential structure could potentially improve the reliability of defect detection by maintaining localized testing within manageable time blocks.
Engagement strategies, test and stimulus characteristics
4.3.2
Many children found the tests boring. Some even struggled to stay awake. The dynamic fixation target used in SONDA seemed to have a slight advantage in keeping children engaged. Nonetheless, active encouragement from the examiner was required to sustain attention throughout the test - especially when testing patients and younger children.
When tested with BulbiCAM, children quickly recognized the predictable sequence in which stimuli were presented (each eccentricity tested from top to bottom before progressing) which made the test easy to anticipate and, consequently, less engaging. For children with VFDs, locating the fixation target after a saccade was often challenging, leading to search behavior.
Developmental aspects
4.4
Normative/ground-truth
4.4.1
Children’s oculomotor and visual systems mature during the first years of life (43, 44). Therefore, pediatric normative datasets spanning a wide age range are crucial to capture this developmental change. However, such datasets for comparison and training purposes are currently missing. In addition, conventional methods such as SAP or GVF are unreliable in young children and cannot be easily used for comparison, highlighted by the fact that some EMP studies lack any comparative test altogether (30, 33).
Saccadic reaction time
4.4.2
Both BulbiCAM and SONDA use SRT as a proxy for visual field sensitivity, enabling rapid data collection. However, SRT is strongly influenced by factors such as stimulus contrast, cognitive load, and age (45, 46). Given these dependencies, its suitability as a reliable proxy is questionable, particularly in children with delayed cognitive development or neurological conditions affecting oculomotor control and attention.
Fixation behavior
4.4.3
The BulbiCAM paradigm requires stable fixation to present stimuli, but in younger children and those with VFDs, this often failed due to inattention or poor tracking. As a result, fewer stimuli were shown, reducing engagement further, and causing interruptions. Additionally, children’s fixation behavior differs from that of adults (47), making standard assumptions about gaze events less applicable in pediatric testing.
Data quality and noise management
4.4.4
Inspection of raw data from our trials revealed that gaze often did not follow the stimulus sequence or trajectory as expected. It was difficult to determine whether this was due to measurement noise, poor performance, or true visual field loss. Accurately distinguishing between these sources of error is essential for interpreting results and assessing the measurement reliability.
The way forward: towards child-centered EMP design
5
Building on our experience with BulbiCAM and SONDA, as well as insights from the broader literature, we offer recommendations to guide further development of EMP for children. We propose child-friendly solutions organized around the four previously mentioned problem areas:
Prioritize child-specific ergonomics and reliability
5.1
Our testing was marked by limited adaptability of setup and recurring hardware and software failures. Test setups must accommodate children while maintaining the robustness essential for clinical use:
Design with the child in mind
5.1.1
Hardware should accommodate children’s size and movement while reliably capturing raw data. Wearable options, such as virtual reality (VR) headsets, may improve stability and allow natural head movements, potentially making the test more comfortable and engaging. VR has shown promise for static perimetry in children as young as nine (48), though further research into usability in younger children and EMP specifically is needed. For non-wearable systems, test setups should be equipped with adjustable tables, seating and mounting solutions to optimize test conditions for all children, including wheelchair-users.
Robust systems
5.1.2
Unlike adult participants, who may tolerate occasional equipment malfunctions or repeated trials, children have minimal tolerance for such disruptions. Therefore, systems intended for clinical use should undergo especially rigorous testing for hardware and software reliability, as system robustness is critical even during early-stage trials in pediatric populations.
Refine tracking and calibration techniques for pediatric use
5.2
A major lesson from current systems is the necessity for adaptive, user-friendly tracking and calibration methods, explicitly validated in pediatric populations:
Illumination modes
5.2.1
Glint based eye tracking systems should offer automated and user-accessible IR level controls or illumination mode settings, allowing for tuning to each individual variations in pupil size and iris reflectivity commonly encountered in children.
Pediatric-trained algorithms
5.2.2
Future machine learning models for gaze and event detection, as well as data analysis, must be trained on data from children across multiple developmental stages. Age-stratified datasets are essential for capturing a full range of typical developmental variability, pupil characteristics, and oculomotor behaviors seen in the pediatric population.
Practical calibration methods
5.2.3
Calibration procedures should balance ease-of-use with spatial accuracy. Promising approaches include calibration-free eye trackers (e.g., Pupil Labs Neon), smooth pursuit calibration, single-point systems (Tobii Pro Glasses 3), and stereoscopic setups using two cameras per eye (49). However, combining uncalibrated eye trackers with test compliance requirements (e.g., fixation requirements) should be avoided, as this results in poor spatial resolution and likely increases overall testing time in the children.
Attention through stimulus and engagement design
5.3
Maintaining attention and ensuring accessibility for all children, regardless of impairment, requires thoughtful stimulus and paradigm design. Several promising strategies include:
Easy pause-and-resume
5.3.1
Tests must include simple, pause and resume functions, allowing children breaks without losing data or the need for restarting entire test segments.
Dynamic fixation and stimuli
5.3.2
Based on our experience, children find it more natural to follow a moving target with their gaze, which in turn enhances engagement. We therefore suggest that future paradigms prioritize dynamic over static stimuli. BulbiCAM offers an optional “green dot animation” feature (a red circle contracting towards the fixation point) to help guide gaze. This feature may be useful but was not employed in order to maximize comparability to other tests and studies.
Color and contrast accessibility
5.3.3
Stimuli should be standardized in terms of luminance contrast, while additional gaze-guiding features - such as the green dot animation used in BulbiCAM - may incorporate color. However, such elements should be designed with common forms of color vision deficiency in mind to ensure visibility and usability for all children, regardless of their color perception.
Gamification and natural viewing
5.3.4
Simple gamification is feasible in certain pediatric age groups (4–12 years) (50). However, the cognitive demands of such designs must be carefully considered to avoid excluding younger or cognitively impaired children. A more universally accessible approach may involve attention-capturing stimuli, such as movie clips, as demonstrated by Allen et al. (51). Additionally, gaze-contingent paradigms and free-viewing of naturalistic scenes, which have been explored in adult populations (52, 53), may offer promising directions for developing more child-friendly EMP tests in the future.
Toward reliable and interpretable pediatric EMP data
5.4
Age-stratified normative databases
5.4.1
The absence of comprehensive normative pediatric datasets poses a major limitation for both clinical interpretation and research. Such reference data describe what is typical at different developmental stages, including age-related changes in eye movement patterns, fixation stability, and saccadic reaction time. These norms are essential not only for identifying deviations that may signal pathology, but also for guiding model development and validation.
Thresholding and saccadic reaction time analysis
5.4.2
The suitability of SRT as a proxy for visual field sensitivity requires further investigation - particularly in children - before it can be considered reliable. An alternative approach may lie in the gradual-onset stimulus mode available in BulbiCAM, where the stimulus progressively increases in luminance. In such cases, SRT becomes less meaningful, and the luminance level that triggers the saccade should be recorded instead. However, this method would likely increase both testing and waiting time, which may limit its feasibility in pediatric populations.
Novel reliability indices for EMP in children
5.4.3
Standard automated perimetry (SAP) provides easy-to-interpret reliability indices based on fixation losses, false positives, and false negatives. Comparable metrics are currently lacking in EMP, but should be developed. These could reflect the number of incorrectly presented stimuli, missing raw data, and saccade characteristics such as accuracy and precision. Age-adjusted scoring would be essential to account for the immaturity of the oculomotor system in younger children.
Discussion
6
This perspective paper, based on experience evaluating two commercial EMP systems in a diverse pediatric sample, highlights multifaceted challenges related to hardware ergonomics, eye tracking and calibration, stimulus engagement, and developmental considerations. To our knowledge, pediatric testing experiences with EMP systems have not been systematically described in the literature.
Research on EMP in children is limited, with only three systems tested: SVOP (28–32), EMPP (34), and “Field Bubbles” (33). All incorporated child-friendly features but relied on calibration, which failed in 5–25% of cases - except “Field Bubbles”, which successfully used a one-point calibration procedure. Overall, successful completion rates in pediatric EMP studies are low (41–81%) (28–34). Direct comparison between studies is limited by differences in methodology, reporting, study populations, and the absence of normative data or reference standards. Together with our observations, this underscores the need for coordinated progress in pediatric EMP development.
Several additional EMP systems are currently under development and being tested in adults (23, 52, 54, 55). It is likely that these systems will soon be tested in children as well, especially given that a recent systematic review identified EMP as a promising emerging technology for pediatric visual field testing (56). To avoid repeating earlier pitfalls in system development, set-up, and study design, we believe that our observations can provide valuable guidance for future pediatric EMP research and development.
Limitations
7
Our perspective is grounded in hands-on clinical experience with two adult EMP systems adapted for use in children. To our knowledge, this is the first report directly comparing multiple systems in a pediatric setting, but it does not capture the full diversity of emerging EMP approaches. The population tested ranged from 4–18 years of age, which limits our ability to comment specifically on the feasibility of EMP in very young children. Our recommendations are intentionally broad and not system-specific, reflecting the early stage of EMP development in children and the absence of established standards. While principles such as ergonomic flexibility, attention-capturing stimuli, and simplified calibration may appear self-evident, these aspects have not yet been formalized into design guidelines and are not consistently addressed in existing systems.
Conclusion
8
Incorporating pediatric testing experience into EMP design is essential to ensure accessibility, reliability, and clinical value. Our observations underscore the importance of interdisciplinary collaboration - particularly between clinicians, engineers, and vision scientists - to adapt these tools for pediatric use. While our focus is on children, such innovations may also inform adaptations for adult populations with comparable cognitive or physical challenges.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Harwerth RS Quigley HA . Visual field defects and retinal ganglion cell losses in patients with glaucoma. Arch Ophthalmology. (2006) 124:853–9. doi: 10.1001/archopht.124.6.853, PMID: 16769839 PMC 2265071 · doi ↗ · pubmed ↗
- 2Grover S Fishman GA Anderson RJ Alexander KR Derlacki DJ . Rate of visual field loss in retinitis pigmentosa. Ophthalmology. (1997) 104:460–5. doi: 10.1016/S 0161-6420(97)30291-7, PMID: 9082273 · doi ↗ · pubmed ↗
- 3Peragallo JH . Effects of brain tumors on vision in children. Int Ophthalmol Clinics. (2018) 58:83–95. doi: 10.1097/IIO.0000000000000237, PMID: 30239365 PMC 6152840 · doi ↗ · pubmed ↗
- 4Azizi AA Walker DA Liu JF Sehested A Jaspan T Pemp B . NF 1 optic pathway glioma: analyzing risk factors for visual outcome and indications to treat. Neuro-Oncology. (2021) 23:100–11. doi: 10.1093/neuonc/noaa 153, PMID: 32628746 PMC 7850076 · doi ↗ · pubmed ↗
- 5Nuijts MA Stegeman I Porro GL Duvekot JC van Egmond-Ebbeling MB van der Linden DCP . Ophthalmological evaluation in children presenting with a primary brain tumor. J Neuroophthalmol. (2022) 42:e 99–108. doi: 10.1097/WNO.0000000000001421, PMID: 34812765 PMC 8834141 · doi ↗ · pubmed ↗
- 6Nuijts MA Stegeman I van Seeters T Borst MD Bennebroek CAM Buis DR . Ophthalmological findings in youths with a newly diagnosed brain tumor. JAMA Ophthalmology. (2022) 140:982–93. doi: 10.1001/jamaophthalmol.2022.3628, PMID: 36107418 PMC 9478881 · doi ↗ · pubmed ↗
- 7Harbert MJ Yeh-Nayre LA O’Halloran HS Levy ML Crawford JR . Unrecognized visual field deficits in children with primary central nervous system brain tumors. J Neurooncol. (2012) 107:545–9. doi: 10.1007/s 11060-011-0774-3, PMID: 22139448 · doi ↗ · pubmed ↗
- 8Tschopp C Safran AB Viviani P Bullinger A Reicherts M Mermoud C . Automated visual field examination in children aged 5–8 years: Part I: Experimental validation of a testing procedure. Vision Res. (1998) 38:2203–10. doi: 10.1016/S 0042-6989(97)00368-4, PMID: 9797979 · doi ↗ · pubmed ↗