Image-Guided Thrombin Injection for Post-procedural Hematomas in Various Surgical Settings: A Case Series
Aws Alfahad, Dura Ibrahim, Basil Ibrahim, Rami Alfahad

TL;DR
This case series shows that image-guided thrombin injections can safely and effectively treat post-surgery hematomas when other options are not possible.
Contribution
The study introduces image-guided thrombin injection as a novel alternative for managing post-procedural hematomas.
Findings
Thrombin injection achieved hemostasis in five patients with post-procedural hematomas.
No thrombin-related complications occurred, and no surgical intervention was needed.
The technique was effective across various surgical settings.
Abstract
Post-procedural hematomas are uncommon but clinically significant complications that can lead to morbidity and mortality. Conventional management often requires surgical re-exploration or embolization, which may be technically unfeasible or high risk in patients with multiple comorbidities. Thrombin injection, although well established for pseudoaneurysm treatment, has been less frequently reported in the management of postsurgical hematomas. We describe five patients who developed post-procedural hematomas following different interventions: robotic hernia repair, ovarian cystectomy, percutaneous nephrostomy, endoscopy, and percutaneous endoscopic gastrostomy tube insertion. Each patient was treated with image-guided thrombin injection under computed tomography or ultrasound guidance. Hemostasis was successfully achieved in all cases without thrombin-related complications, and patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
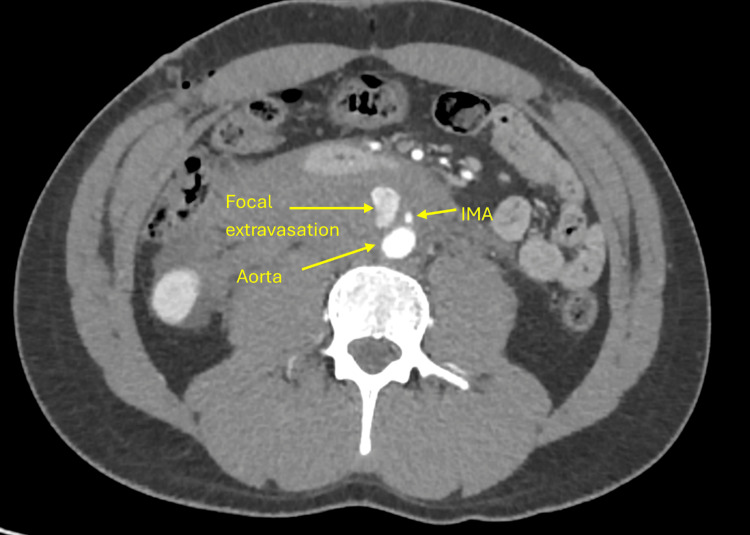 Figure 1
Figure 1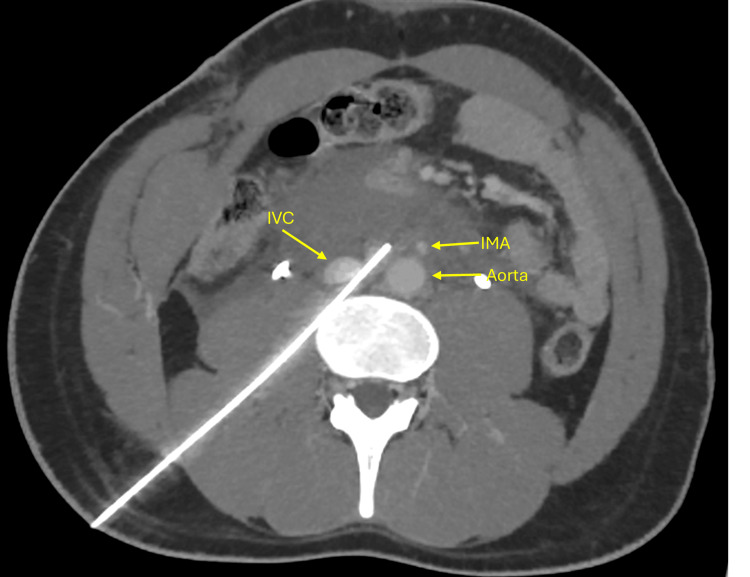 Figure 2
Figure 2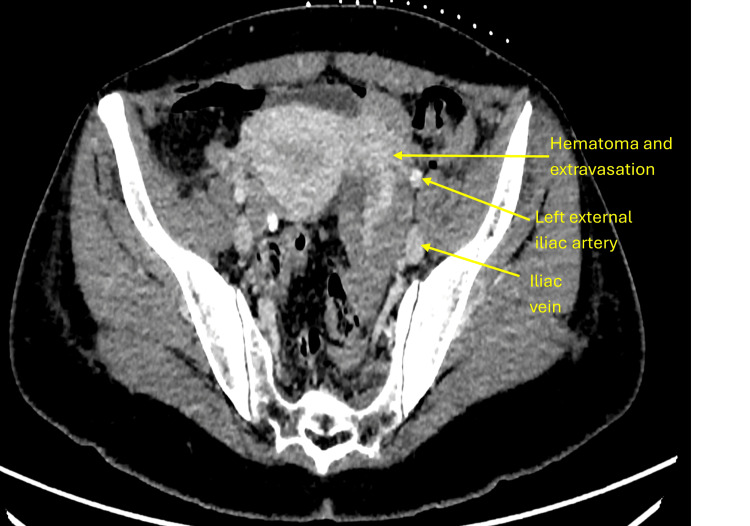 Figure 3
Figure 3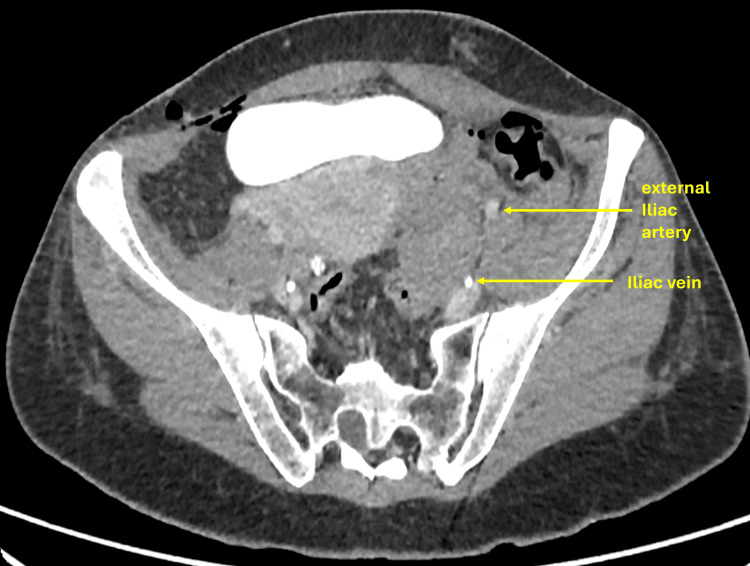 Figure 4
Figure 4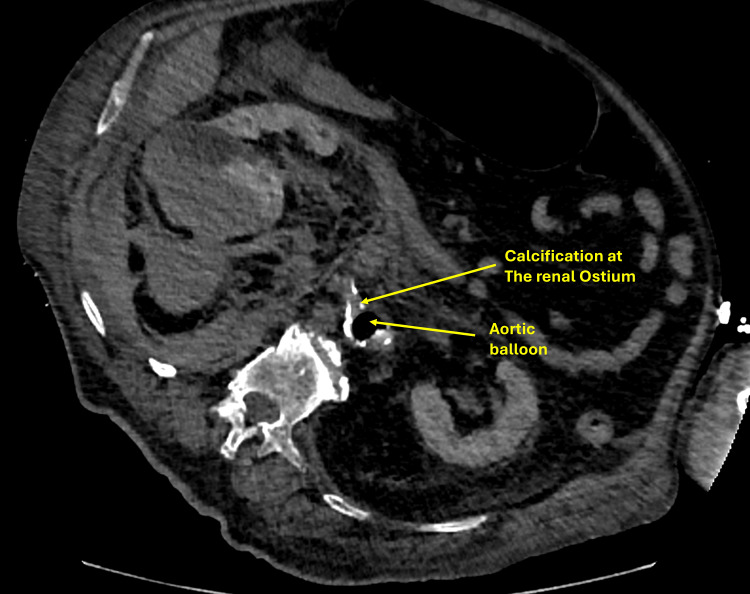 Figure 5
Figure 5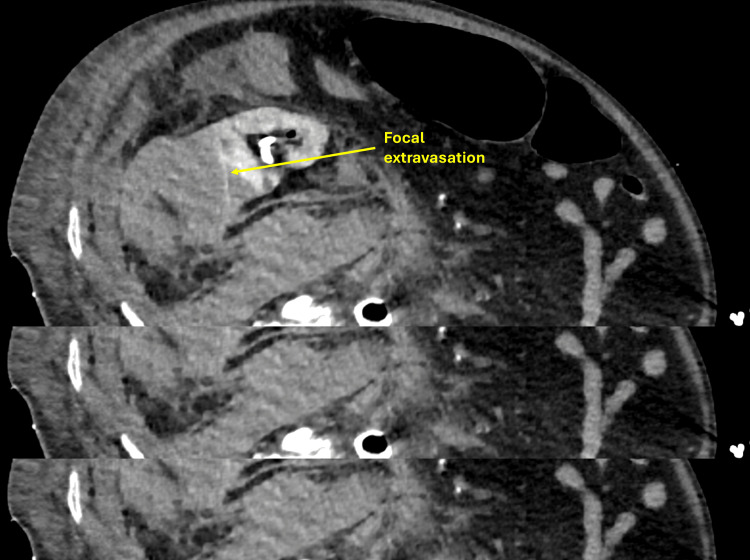 Figure 6
Figure 6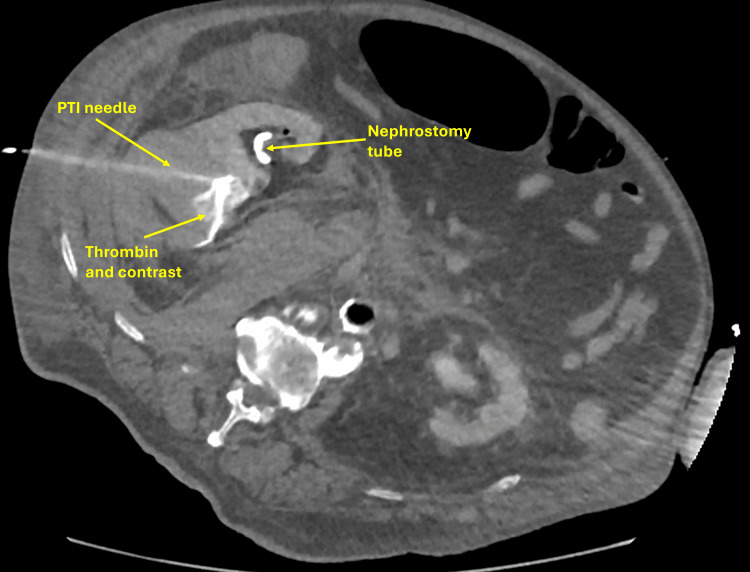 Figure 7
Figure 7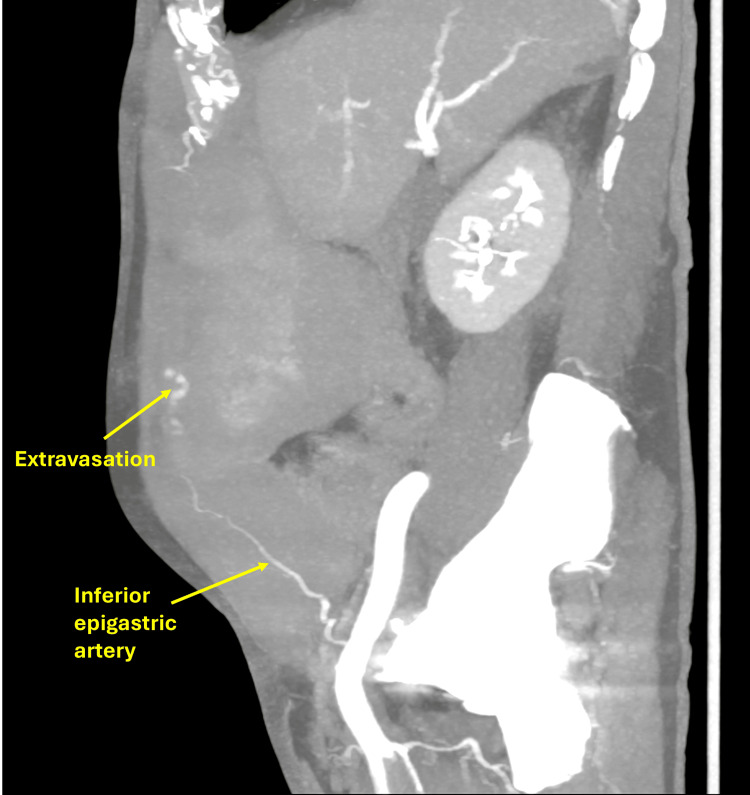 Figure 8
Figure 8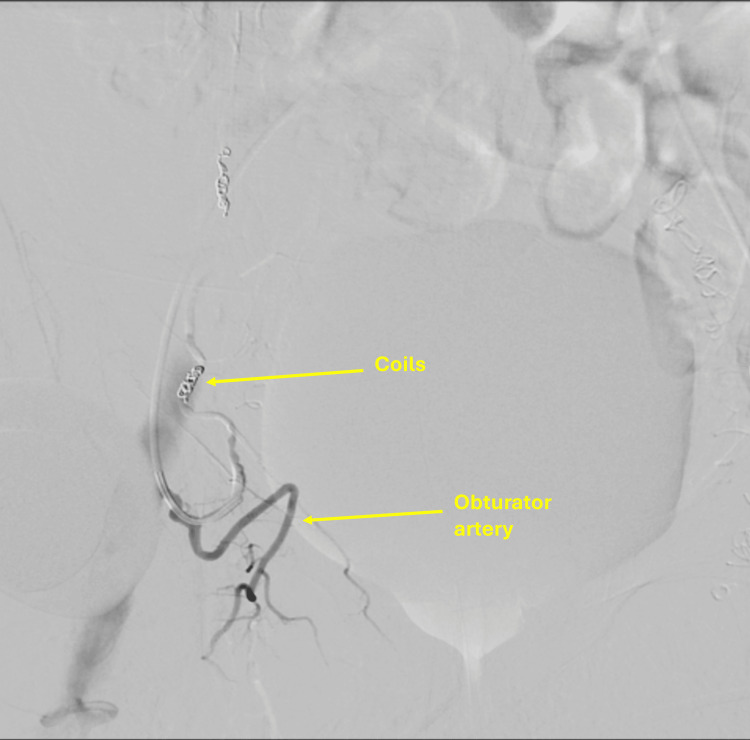 Figure 9
Figure 9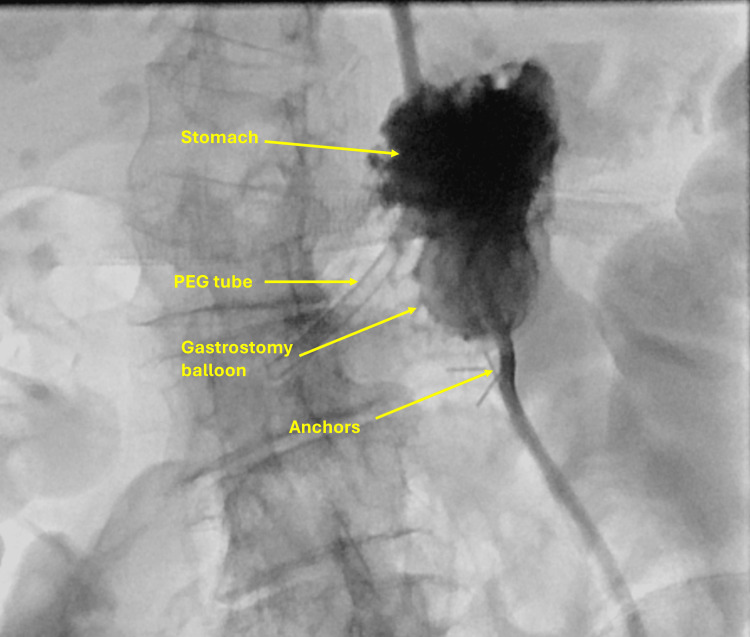 Figure 10
Figure 10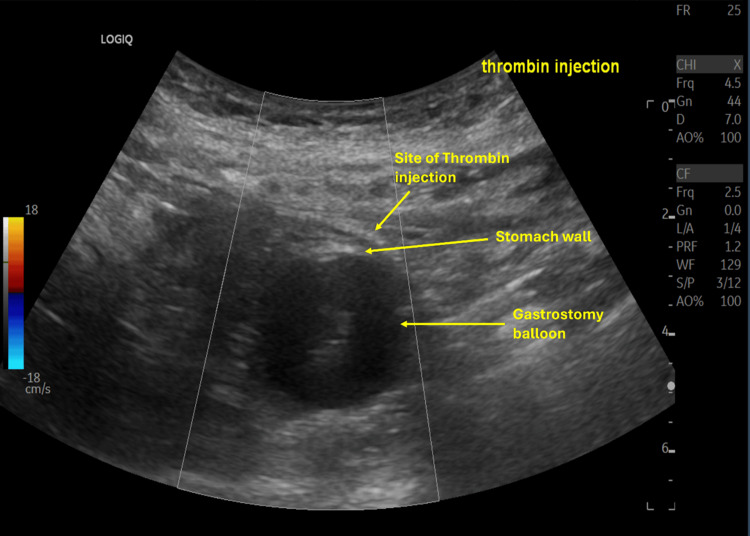 Figure 11
Figure 11| Case | Age/sex | Surgical procedure | Hematoma location | Imaging modality used | Thrombin dose (IU) | Additional intervention | Outcome/follow-up |
| 1 | 28, M | Robotic inguinal hernia repair | Retroperitoneum (aortic extravasation) | CT-guided | 10,000 | None | Complete hemostasis; stable on follow-up |
| 2 | 45, F | Cystectomy (gynecologic) | Pelvic/inferior epigastric artery | CT-guided | 5,000 | None | Hemostasis confirmed; hematoma decreased on 48-hour CT |
| 3 | 74, M | Percutaneous nephrostomy | Perirenal space | CT-guided | 8,000 | None | Stable post-procedure; hematoma resolved |
| 4 | 77, M | On enoxaparin for atrial fibrillation | Abdominal wall/inferior epigastric artery | CT + US | 7,500 | Adjunct coil embolization | Complete hemostasis; no complications |
| 5 | 86, F | PEG insertion | Abdominal wall | US-guided | 4,000 | None | Stable; full recovery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Procedures and Complications · Case Reports on Hematomas · Venous Thromboembolism Diagnosis and Management
Introduction
Post-procedural bleeding is a common complication following various surgical and interventional procedures, particularly among patients with significant comorbidities. Inguinal hernia repair, pelvic operations, and nephrostomy procedures are especially prone to such vascular injuries and subsequent hematoma formation. Traditionally, management of post-procedural hematomas required surgical exploration or other invasive interventions. However, advances in interventional radiology have introduced image-guided thrombin injection as a minimally invasive and highly effective option for achieving hemostasis in such cases. Compared with conventional surgical or endovascular methods, thrombin injection offers shorter recovery, reduced procedural morbidity, and a lower risk of complications.
Multiple studies have demonstrated the safety and high success rate of thrombin injection, particularly in treating iatrogenic pseudoaneurysms and soft-tissue hematomas [1-3]. While ultrasound (US)-guided thrombin injection is well established for femoral pseudoaneurysms, its CT- or image-guided application in other postoperative or non-vascular hematomas remains relatively limited and less well documented [4-6].
Thrombin injection promotes clot formation by converting fibrinogen to fibrin, resulting in rapid and stable hemostasis. This case series presents five patients who developed post-procedural hematomas following different surgical interventions. Thrombin injection was selected as the management approach because each patient had localized, well-defined collections accessible to image-guided injection, and all were considered poor candidates for open surgical evacuation due to comorbidities or elevated bleeding risk. Traditional surgical or conservative approaches were associated with higher morbidity, prolonged recovery, or incomplete resolution in such cases. Therefore, image-guided thrombin injection provided a minimally invasive, targeted, and safe alternative that achieved rapid hemostasis and symptom relief.
Case presentation
Case 1
A 28-year-old male with a history of recurrent inguinal hernia underwent robotic hernia repair. Postoperatively, he developed increasing abdominal pain and mild tachycardia, raising concern for concealed hemorrhage. Given his clinical instability, a contrast-enhanced computed tomography (CT) of the abdomen was performed (Figure 1).
CT of the abdomen with contrast showing extravasation from the aorta with expanding hematoma at the level of the inferior mesenteric artery (IMA).
The patient developed new-onset abdominal and back pain after robotic hernia repair. A CT scan performed for evaluation revealed a retroperitoneal hematoma with active extravasation from the abdominal aorta, likely due to Veress needle injury during trocar insertion. Although the patient was young, surgical re-exploration was considered high risk because the source of bleeding was a direct extravasation from the aortic wall below the level of the inferior mesenteric artery. Re-entry into the operative field after recent robotic mesh repair would have required extensive dissection through adhesions with a substantial risk of catastrophic aortic hemorrhage. Endovascular stenting was also deemed unsuitable due to the proximity of the lesion to the inferior mesenteric artery and the danger of branch occlusion. Therefore, a multidisciplinary team concluded that CT-guided thrombin injection offered the safest and most targeted means of achieving hemostasis. CT-guided thrombin injection was performed via a retroperitoneal approach and was successful in managing the bleeding (Figure 2). The patient was monitored in the intensive care unit for 48 hours following the procedure, during which he remained hemodynamically stable and had no signs of rebleeding. He was subsequently discharged in good condition and continued to recover without complications.
CT of the abdomen showing resolution of the hematoma with patent inferior vena cava (IVC) and inferior mesenteric artery (IMA).
Case 2
A 45-year-old female underwent robotic-assisted ovarian cystectomy with extensive adhesiolysis. On postoperative day one, she developed new abdominal pain, tenderness, and 370 mL of dark blood in the pelvic drain, raising concern for ongoing bleeding. Contrast-enhanced CT of the abdomen demonstrated a large left pelvic sidewall hematoma measuring 43 × 82 × 63 mm, with an arterial blush and progressive venous pooling (Figure 3).
Porto-venous CT scan showing hematoma and active extravasation over the left ovarian area.
Although the patient was stable, surgical re-exploration was considered high risk because the hematoma was located deep within the pelvis, adjacent to major vessels and the urinary bladder, in a recently operated field. Re-entry into the surgical site would have carried a substantial risk of hemorrhage, infection, and tissue disruption. Endovascular embolization was also deemed unsuitable due to anatomical challenges: targeting the ovarian branch of the uterine artery risked compromising uterine perfusion, while accessing the left ovarian artery, arising directly from the aorta, was technically difficult. Consequently, a minimally invasive image-guided thrombin injection was selected as the safest and most targeted alternative for achieving hemostasis. Follow-up CT confirmed resolution of bleeding with a reduction in hematoma size (Figure 4). The patient recovered uneventfully. Post-procedure CT angiography performed immediately after thrombin injection demonstrated cessation of active extravasation, confirming technical success. A follow-up CT scan obtained 48 hours later showed interval reduction in the hematoma size, consistent with effective thrombin-induced hemostasis rather than spontaneous resolution.
CT of the abdomen showing complete resolution of the hematoma and patent iliac arteries and veins.
Case 3
A 74-year-old patient presented with respiratory distress, septic and cardiogenic shock, and non-ST-segment elevation myocardial infarction (NSTEMI), with echocardiography showing left ventricular ejection fraction (LVEF) of 35% and severe mitral regurgitation. He also had acute kidney injury and urinary retention. Due to bladder outlet obstruction from stricture and prostate enlargement, retrograde access was not possible, and a percutaneous nephrostomy was planned (Figure 5).
CT of the abdomen showing a calcified renal artery ostium and an intra-aortic balloon pump in place.
The patient developed flank pain and a drop in hemoglobin following percutaneous nephrostomy. Post-procedure imaging revealed a large subcapsular and perinephric hematoma (8.1 × 6 cm) with active hemorrhage arising from the lower pole region of the right kidney (Figure 6). Catheter angiography was unsuitable due to the presence of an intra-aortic balloon pump and severe renal artery calcification.
CT image showing right perinephric extravasation at the nephrostomy site.
CT-guided thrombin injection using a retroperitoneal approach was performed under aseptic conditions, injecting 10 mL of thrombin into the bleeding site, successfully controlling the hemorrhage (Figure 7). The patient recovered with improved renal function and was discharged in stable condition.
CT-guided thrombin injection into the right perinephric hematoma at the nephrostomy site.PTI: percutaneous thrombin injection.
Case 4
A 77-year-old male on anticoagulation with subcutaneous enoxaparin 40 mg daily for atrial fibrillation developed acute abdominal pain and distension shortly after diagnostic endoscopy. Examination revealed a firm abdominal wall mass, and CT imaging demonstrated a large right rectus sheath hematoma with active extravasation from the inferior epigastric artery (Figure 8).
CT of the abdomen showing extravasation in the region of the right inferior epigastric artery.
Although active extravasation from the inferior epigastric artery was evident on initial imaging, thrombin injection was selected as the first-line intervention due to both anatomical and clinical considerations. The bleeding vessel was small, superficial, and tortuous, making selective catheterization technically challenging and increasing the risk of non-target embolization. In addition, the patient’s advanced age and ongoing anticoagulation with enoxaparin for atrial fibrillation increased the risk of endovascular access complications. Initial thrombin injection (7,500 IU) under combined CT and ultrasound guidance significantly reduced bleeding, but mild residual vascularity persisted. Therefore, adjunct selective coil embolization was performed, and final angiography confirmed complete hemostasis with preservation of collateral flow (Figure 9). The patient remained hemodynamically stable with no procedure-related complications.
Selective embolization of the right inferior epigastric artery using 2 mm and 3 mm coils.
Case 5
An 86-year-old female with advanced heart failure, severe aortic stenosis, chronic kidney disease, and recurrent aspiration was admitted to the intensive care unit (ICU) for circulatory shock secondary to gastrointestinal (GI) bleeding. After stabilization, a percutaneous endoscopic gastrostomy (PEG) tube was inserted.
Shortly after transfer from the endoscopy suite, she developed active bleeding from the gastrostomy site with a hemoglobin drop requiring transfusion. Bedside US confirmed active bleeding at the access tract (Figure 10).
Fluoroscopy showing active bleeding from the gastrostomy tract.PEG: percutaneous endoscopic gastrostomy.
Given her frailty and comorbidities, bedside US-guided thrombin injection (5,000 IU) was performed, achieving immediate hemostasis (Figure 11). The patient’s hemoglobin stabilized, and she tolerated PEG feeding without further bleeding complications.
Bedside ultrasound-guided thrombin injection at the gastrostomy site demonstrating hemostasis.
A summary of the clinical and procedural details for all five cases, including imaging modality, thrombin dose, and outcomes, is presented in Table 1.
Discussion
Our series demonstrates that image-guided thrombin injection is a safe and effective alternative to embolization or surgical intervention for selected postprocedural hematomas. It is particularly useful when conventional options are technically unfeasible or contraindicated. The first reported case of CT-guided thrombin injection for retroperitoneal hematoma from aortic injury during hernia repair underscores its potential value in complex scenarios. Wider adoption and standardization of techniques and dosing protocols could further optimize safety and outcomes in interventional radiology practice.
Overall, perioperative bleeding occurs in approximately one out of every 65 non-cardiac surgical procedures, with rates being higher in individuals who have increased cardiovascular risk. Among hospitalized postsurgical patients experiencing perioperative bleeding, one-third either die during their admission or require readmission within six months [4].
Cystectomy, the surgical excision of one or both ovaries along with any related cystic structures, is commonly performed in women of reproductive age. It is typically indicated for a range of ovarian pathologies, such as benign cysts, endometriosis, and ovarian malignancies [5,6]. As with many surgical procedures, cystectomy carries a risk of postoperative complications, including bleeding.
Literature reports suggest that percutaneous nephrostomy carries an incidence of serious vascular injury of approximately 1%-2% [7-10]. However, this figure may underestimate the true rate [11]. Renal arteriovenous fistulas and pseudoaneurysms are frequently undetected at first because they are often asymptomatic and may only become apparent months or even years later [12-14]. Although uncommon, severe renal vascular injury from needle puncture can result in fatality, nephrectomy, surgical exploration, large perirenal hematomas, septicemia, transfusion diseases, and other systemic complications.
Pharmacologic agents such as aprotinin, tranexamic acid, desmopressin, and recombinant factor VIIa are utilized both prophylactically and therapeutically to control bleeding. When these medications are insufficient, alternative non-surgical techniques, including thrombin injection, may be required [15].
The application and results of percutaneous thrombin injection have been documented for various indications. Hoegger et al. reported thrombin injection following renal and hepatic biopsies, with hemostasis achieved in 94% of patients [16]. Alfahad and Alhalabi reported thrombin injection as safe and effective for PEG stoma-site bleeding [17]. Ultrasound-guided thrombin injection into visceral pseudoaneurysms has also been reported as a valuable alternative when angiographic therapy is not feasible, with low recurrence and embolization rates [18]. Additional reports describe successful treatment of hepatic artery pseudoaneurysms when embolization failed [19,20].
CT-guided thrombin injection represents a reliable and effective approach for managing post-procedural hematomas across various surgical settings. Its minimally invasive nature, combined with its ability to provide targeted hemostasis, makes it an appealing option, particularly for patients at high risk of complications. Compared with conventional surgical re-exploration, image-guided thrombin injection offers markedly reduced procedural morbidity, faster recovery, and avoidance of general anesthesia. When compared with endovascular embolization, it eliminates the risks of contrast-induced nephropathy, non-target embolization, and vascular access complications, while achieving comparable rates of hemostatic success in appropriately selected, localized hematomas. Several studies have also reported low recurrence rates and minimal adverse events, supporting its role as a safe and effective alternative to traditional methods [16-20].
Conclusions
Our series demonstrates that image-guided thrombin injection is a safe and effective alternative to embolization or surgical intervention for selected post-procedural hematomas. It is particularly useful when conventional options are technically unfeasible or contraindicated. Although the safety and efficacy of thrombin injection have been well established in treating femoral pseudoaneurysms, its application for managing postoperative or non-pseudo-aneurysmal hematomas remains relatively uncommon and less well documented. Therefore, it is presented here as an alternative approach in complex surgical cases where conventional methods are not ideal or carry higher procedural risks. The first reported case of CT-guided thrombin injection for retroperitoneal hematoma from aortic injury during hernia repair underscores its potential value in complex scenarios. Wider adoption and standardization of techniques and dosing protocols could further optimize safety and outcomes in interventional radiology practice. Our review of the literature identified consistently high technical success rates across multiple reports, with very low recurrence and complication rates. Most published cases describe successful use of thrombin injection for femoral pseudoaneurysms, while a smaller number document its expanding role in managing visceral, parietal, and postoperative hematomas under ultrasound or CT guidance. Complications such as distal thrombosis or embolization were exceedingly rare when the technique was performed under imaging control and with appropriate dosing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Treatment of iatrogenic femoral artery pseudoaneurysm with percutaneous thrombin injection J Vasc Surg Liau CS Ho FM Chen MF Lee YT 1823261997924031610.1016/s 0741-5214(97)70141-1 · doi ↗ · pubmed ↗
- 2Percutaneous ultrasound-guided thrombin injection for the treatment of iatrogenic femoral artery pseudoaneurysms Eur J Radiol Vlachou PA Karkos CD Bains S Mc Carthy MJ Fishwick G Bolia A 172174772011 https://pubmed.ncbi.nlm.nih.gov/19660885/1966088510.1016/j.ejrad.2009.06.032 · doi ↗ · pubmed ↗
- 3Intranodal lipiodol injection for the treatment of chyle leak in children - a preliminary experience Br J Radiol Gupta A Naranje P Vora Z 20211270952022 https://pubmed.ncbi.nlm.nih.gov/35856789/3585678910.1259/bjr.20211270 PMC 10996956 · doi ↗ · pubmed ↗
- 4Perioperative major adverse cardiovascular and cerebrovascular events associated with noncardiac surgery JAMA Cardiol Smilowitz NR Gupta N Ramakrishna H Guo Y Berger JS Bangalore S 181187220172803066310.1001/jamacardio.2016.4792 PMC 5563847 · doi ↗ · pubmed ↗
- 5Ovarian cyst Stat Pearls Mobeen S Apostol R Treasure Island, FL Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 560541/32809376 · pubmed ↗
- 6Overview: Ovarian cysts Cologne (DE): Informed Health.org 2006 https://www.ncbi.nlm.nih.gov/books/NBK 539572/
- 7Percutaneous catheterization of the kidney and perinephric space: trocar technique Urol Radiol Newhouse JH Pfister RC 15716421981 https://pubmed.ncbi.nlm.nih.gov/7020206/702020610.1007/BF 02926718 · doi ↗ · pubmed ↗
- 8Percutaneous nephrostomy: a series and review of the literature AJR Am J Roentgenol Stables DP Ginsberg NJ Johnson ML 75821301978 https://doi.org/10.2214/ajr.130.1.7541342210.2214/ajr.130.1.75 · doi ↗ · pubmed ↗