Postoperative insulin requirements in surgical patients receiving fully automated insulin delivery in the hospital
Gabija Krutkyte, Clara Escorihuela-Altaba, Michael S. Hughes, Christos T. Nakas, David Herzig, Lia Bally

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
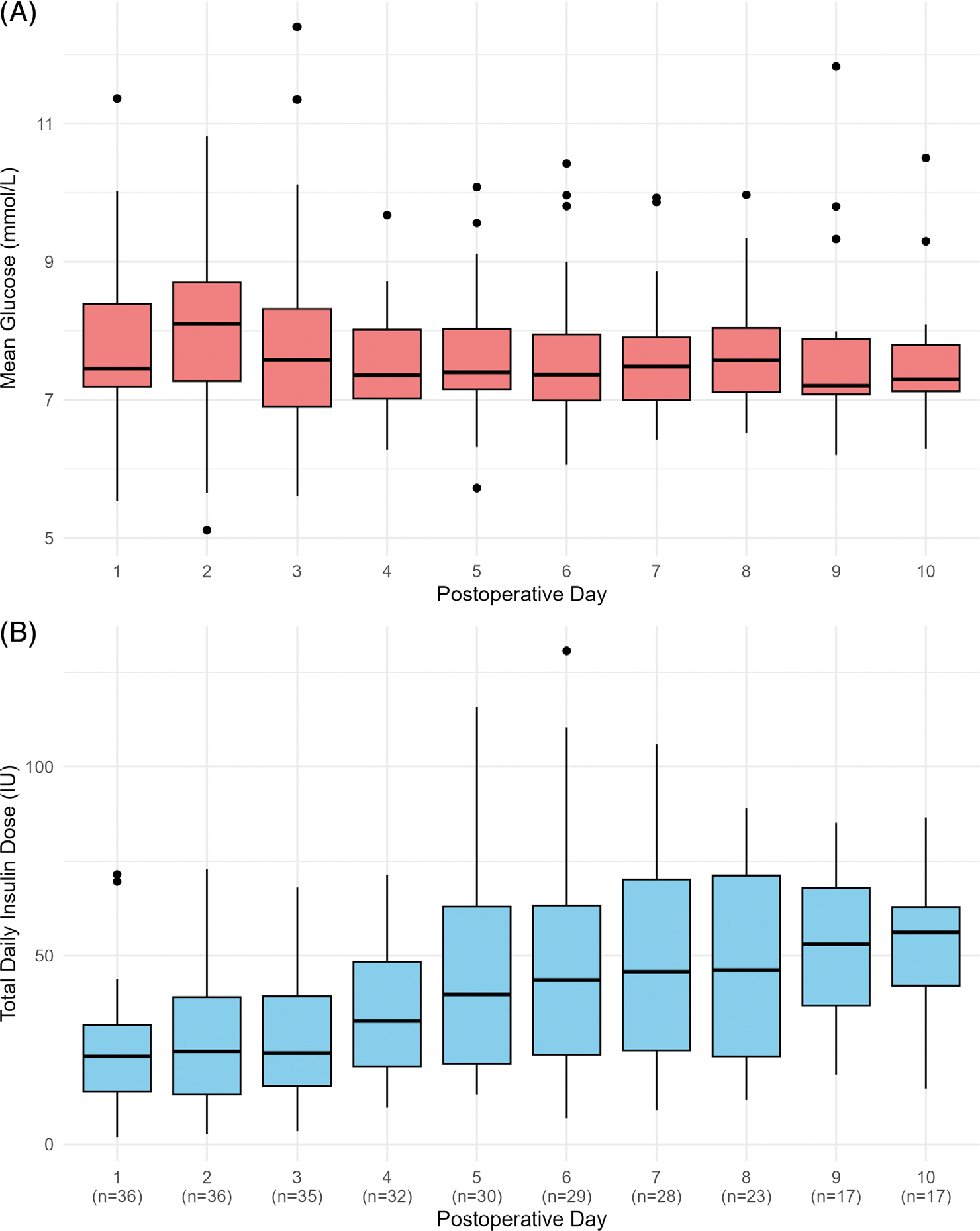 Figure 1
Figure 1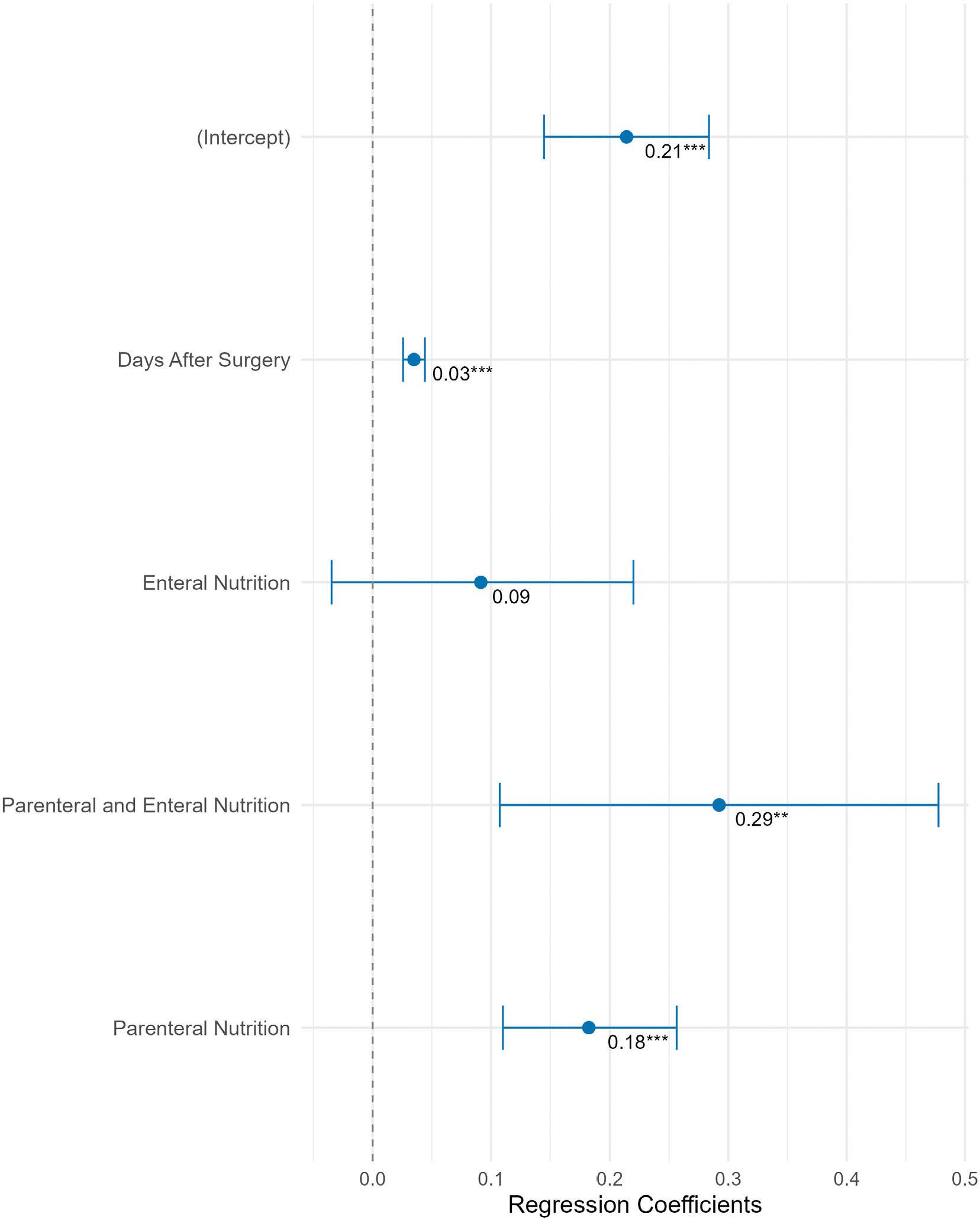 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHyperglycemia and glycemic control in critically ill and hospitalized patients · Diabetes Management and Research · Diabetes and associated disorders
BACKGROUND
1 |
Surgery-induced metabolic stress, immobilisation and adjunctive therapies (e.g., glucocorticoids, nutritional support) cause dynamic changes in insulin requirements.^1,2^ A mismatch between prescribed and actual insulin needs predisposes patients to dysglycaemia, which is associated with prolonged hospitalisation and adverse outcomes.^3–5^ Fully automated insulin delivery (AID) systems continuously titrate insulin to maintain target glucose levels, offering both effective perioperative support for complex patients^6,7^ and insights into insulin requirements. This study examined perioperative insulin delivery in patients with fully AID and identified determinants of insulin needs to inform postoperative glycaemic strategies.
METHODS
2 |
Study design
2.1 |
Data from two randomised controlled trials (NCT05392452 and NCT04361799) investigating the glycaemic efficacy of fully AID in hospitalised surgical patients with insulin-requiring non-type 1 diabetes were pooled and retrospectively analysed. Both trials had ethics approval (2020–01024, 2022-D0034) and all participants provided written informed consent. Eligible adults underwent elective surgery, were expected to require insulin, and remained hospitalised ≥72 h postoperatively; type 1 diabetes was excluded. The AID system comprised the Dexcom G6 subcutaneous continuous glucose monitoring (Dexcom, USA), an android smartphone hosting the CamAPS HX application with a model predictive control algorithm (University of Cambridge, Cambridge, UK), and a subcutaneous insulin pump—either YpsoPump (Ypsomed AG, Burgdorf, Switzerland) or the DANA RS insulin pump (Diabecare, Sooil, Seoul, South Korea), delivering fast-acting insulin aspart (Fiasp, Novo Nordisk). AID was initialised using participants’ body weight and estimated total daily insulin dose (TDD), with a glucose target of 5.8 mmol/L.
Data collection
2.2 |
Continuous insulin delivery and glucose data were retrieved from a cloud-based diabetes management platform (Glooko, Inc., Palo Alto, California, USA). Clinical data, including nutrition support type (parenteral, enteral or both) and glucocorticoid use (documented daily as a binary variable), were extracted from electronic health records. For a subset of patients, daily carbohydrate (CHO) intake (oral plus nutritional support, calculated over 24-h periods [00:00 to 23:59]) was obtained from the hospital’s electronic meal management software.
Statistical analysis
2.3 |
TDD and weight-normalised TDD (TDD/kg) were calculated for each patient, from the first postoperative day (00:00) until the 10th postoperative day or discharge, excluding the day of surgery and discharge. Day-to-day variability was assessed by the coefficient of variation (CV) of TDD, calculated for each patient.
Changes in TDD were analysed with a linear mixed-effects model. Predictor significance was tested with Type III Wald chi-square tests, and model assumptions were verified graphically.
Linear mixed-effects models assessed effects of postoperative day, nutrition support (parenteral vs. enteral vs. concomitantly administered parenteral and enteral) and glucocorticoid therapy on TDD/kg, adjusted for surgery type, glycated haemoglobin (HbA1c), sex, age and body mass index (BMI). Postoperative day was included as a fixed effect and participant as a random intercept to account for within-subject correlation. Non-significant terms were removed to reduce model complexity and improve interpretability. For patients with CHO data, a quadratic term accounted for non-linear effects.
Results from the fixed-effects estimates are presented with 95% confidence intervals [95% CI], p-values, and using Forest plots, while non-linear effects of CHO supply on TDD/kg are visualised graphically. Descriptive statistics are presented as mean ± standard deviation (SD) for normally distributed variables or median [25th; 75th percentile] for non-normally distributed variables unless specified otherwise. Analyses were performed using R (4.4.1).
RESULTS
3 |
Clinical context and glucose control
3.1 |
Thirty-six patients (277 patient-days, mean age 67.8 ± 11 years, 39% female, HbA1c 7.2% [6.4; 8]) were analysed (Table S1). Abdominal surgery was most common (n = 27 (75%), including seven total pancreatectomies). Postoperatively, 36% received parenteral nutrition, 8% enteral and 14% parenteral and enteral nutrition concomitantly. Postoperative glucocorticoids were prescribed in 14% of patients. In a subset of 13 patients (99 patient-days) for whom detailed CHO data were available, the mean between-participant daily CHO supply was 163 ± 42 g (105 ± 68 g with solely oral nutrition; 123 g [81; 167] with enteral nutrition support [as a stand-alone or in combination with oral nutrition]; 187 g [170; 223] with parenteral nutrition [with or without accompanying oral nutrition]). The concomitant use of parenteral with enteral nutrition delivered the highest quantities of 286 [264; 302] g/day.
Postoperative mean daily glucose levels were maintained between 7.2 and 8.1 mmol/L, and time with glucose levels between 3.9 and 10.0 mmol/L was 89.1% [82.2; 93.2] (Figure 1A, Table S2).
Insulin requirements
3.2 |
Figure 1B illustrates the temporal evolution of postoperative insulin requirements, with daily doses normalised by body weight presented in Table S3. Insulin requirements were lowest on the first postoperative day and increased over time after surgery, peaking on Day 10 at 0.65 [0.47; 0.81] units/kg, representing a 2.41 [2.08; 3.36]-fold change. Between-day variability in insulin requirements during the 10 postoperative days was substantial (CV 42 ± 18.7%).
Determinants of insulin requirements
3.3 |
Parenteral nutrition, concomitant parenteral and enteral nutrition and days after surgery were significantly associated with higher daily insulin requirements when compared to days with oral nutrition only. TDD/kg was 0.18 IU/kg [0.1; 0.3] higher on days with parenteral nutrition and 0.03 IU/kg [0.02; 0.04] higher with each day after surgery (all p < 0.001). Preoperative HbA1c, BMI, age, sex, pancreatic surgery, postoperative enteral nutrition and glucocorticoid therapy were not significant predictors. Regression coefficients for daily insulin dose are presented in Figure 2.
In patients with CHO data, insulin requirements increased non-linearly with CHO intake, from 0.45 IU/kg (fasting) to 0.95 IU/kg at 300 g/day (p < 0.001; Figure S1).
CONCLUSIONS
4 |
This study characterised daily postoperative insulin delivery and its determinants in surgery patients using fully AID. Excellent glucose control (89.1% time in range) enabled robust insights into postoperative insulin needs, which varied substantially—lowest immediately after surgery and rising 2.4-fold by Day 10, with a day-to-day CV of 42%. Parenteral nutrition, with or without enteral supplementation, was a significant predictor of insulin needs, alongside postoperative day. CHO supply exhibited a non-linear positive association with insulin dose, although the dose–response may be influenced by unmeasured factors such as feeding schedule, nutrient composition and individual insulin sensitivity. Importantly, postoperative day independently predicted insulin requirements even after accounting for CHO intake, indicating additional physiological mechanisms.
Day-to-day insulin variability in this cohort (42 ± 18.7%) significantly exceeded that of non-surgical inpatients using identical AID algorithms (30 ± 16%),^8^ highlighting the unique challenges of the immediate postoperative period and the necessity for vigilant titration. Consistent with prior evidence,^8^ baseline characteristics (BMI, age, sex and HbA1c) were not predictive. These findings suggest that insulin therapy cannot rely on admission parameters alone, but rather must be dynamically adjusted to recovery and interventions, particularly nutrition. The lack of a statistically significant effect of glucocorticoid therapy may be attributable to both the limited sample size of treated patients and the binary categorisation of glucocorticoid use, which precluded dose-dependent analysis. This is a crucial area for future research in larger studies.
Parenteral nutrition emerged as a strong predictor of insulin requirements. This observation is physiologically consistent, as intravenous glucose administration bypasses the incretin effect that normally potentiates glucose-stimulated insulin secretion during oral or enteral nutrient absorption.^9^ Combined parenteral-enteral nutrition generated the highest insulin requirements, as its CHO load often exceeded 200 g/day—the recommended threshold for hospitalised patients with diabetes.^10^ These findings suggest that careful moderation of carbohydrate intake is a practical way to support postoperative glycaemic control, especially where automated titration is unavailable.
Limitations include a small sample size (36 patients), a post hoc approach, potential underestimation of endogenous insulin and that carbohydrate data were available for only a subset of patients, restricting the scope of the dose–response relationship between nutrition and insulin needs. Data provision from a single hospital may limit external validity. Findings may not generalise beyond surgical populations or less invasive procedures.
In conclusion, fully AID provides valuable insights into metabolic dynamics. The highly variable postoperative insulin requirements, driven by nutrition support and carbohydrate provision, underscore the need for adaptive glucose management. While our hypothesis-generating study robustly characterises this phenomenon, larger prospective trials are needed to validate these predictors and develop adaptive AID-dosing algorithms that account for nutritional variability and other challenges to optimise postoperative care.
Supplementary Material
1
SUPPORTING INFORMATION
Additional supporting information can be found online in the Supporting Information section at the end of this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thorell A, Efendic S, Gutniak M, Häggmark T, Ljungqvist O. Insulin resistance after abdominal surgery. Br J Surg. 1994;81(1):59–63.8313123 10.1002/bjs.1800810120 · doi ↗ · pubmed ↗
- 2Teshigawara S, Tone A, Katayama A, Time course change of the insulin requirements during the perioperative period in hepatectomy and pancreatectomy by using an artificial pancreas STG-55. Diabetol Int. 2023;14(3):262–270.37397907 10.1007/s 13340-023-00623-3PMC 10307749 · doi ↗ · pubmed ↗
- 3Frisch A, Chandra P, Smiley D, Prevalence and clinical outcome of hyperglycemia in the perioperative period in noncardiac surgery. Diabetes Care. 2010;33(8):1783–1788.20435798 10.2337/dc 10-0304 PMC 2909062 · doi ↗ · pubmed ↗
- 4Long CA, Fang ZB, Hu FY, Poor glycemic control is a strong predictor of postoperative morbidity and mortality in patients undergoing vascular surgery. J Vasc Surg. 2019;69(4):1219–1226.30459015 10.1016/j.jvs.2018.06.212 · doi ↗ · pubmed ↗
- 5de Vries FEE, Gans SL, Solomkin JS, Meta-analysis of lower perioperative blood glucose target levels for reduction of surgical-site infection. Br J Surg. 2017;104(2):e 95–e 105.27901264 10.1002/bjs.10424 · doi ↗ · pubmed ↗
- 6Herzig D, Suhner S, Roos J, Perioperative fully closed-loop insulin delivery in patients undergoing elective surgery: an open-label, randomized controlled trial. Diabetes Care. 2022;45(9):2076–2083.35880252 10.2337/dc 22-0438 · doi ↗ · pubmed ↗
- 7Krutkyte G, Goerg AMC, Grob CA, Perioperative fully closed-loop versus usual care glucose management in adults undergoing major abdominal surgery: a two-centre randomized controlled trial. Ann Surg. 2025;281(5):732–740. doi:10.1097/SLA.000000000000654939348314 PMC 11974617 · doi ↗ · pubmed ↗
- 8Lakshman R, Daly AB, Nwokolo M, Variability of insulin requirements in adults with type 2 diabetes during fully closed-loop insulin delivery. Diabetes Technol Ther. 2023;25(6):442–444.36971607 10.1089/dia.2023.0073 · doi ↗ · pubmed ↗