Cutaneous anthrax outbreak associated with use of cattle hides and handling carcasses, Amudat District, Uganda, 2023–2024
Patrick Kwizera, Richard Migisha, Hannington Katumba, Esther Nabatta, Samuel Gidudu, Benon Kwesiga, Job Morukileng, Lilian Bulage, Alex Riolexus Ario, Chisoni Mumba, Chisoni Mumba, Chisoni Mumba, Chisoni Mumba

TL;DR
A cutaneous anthrax outbreak in Uganda was linked to handling cattle carcasses and using cattle hides as bedding, with recommendations for prevention.
Contribution
The study identifies specific risk factors for anthrax transmission in a community setting and provides actionable prevention strategies.
Findings
102 cutaneous anthrax cases were identified with a peak in March 2024.
Using cattle hides as bedding and butchering carcasses were strongly associated with anthrax infection.
No livestock had been vaccinated prior to the outbreak, highlighting a gap in preventive measures.
Abstract
Anthrax is a zoonotic disease that remains endemic in Uganda, particularly in cattle-keeping areas. On December 28, 2023, the first suspected human case of anthrax was detected in Amudat District. We investigated to determine the outbreak’s magnitude, identify risk factors, and recommend prevention and control measures. We defined a suspected cutaneous anthrax case as acute onset of ≥2 of the following: skin lesions (papule, vesicle, or eschar) on exposed areas such as the hands, forearms, shoulders, back, thighs or face, localized itching, redness, swelling, or regional lymphadenopathy, in Amudat residents from December 2023–June 2024. A confirmed case was a suspected case with PCR-positive test for Bacillus anthracis. In unmatched case-control study (1:3 ratio), we compared exposures among 40 cases and 120 controls. We identified cases through house-to-house search, medical record…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
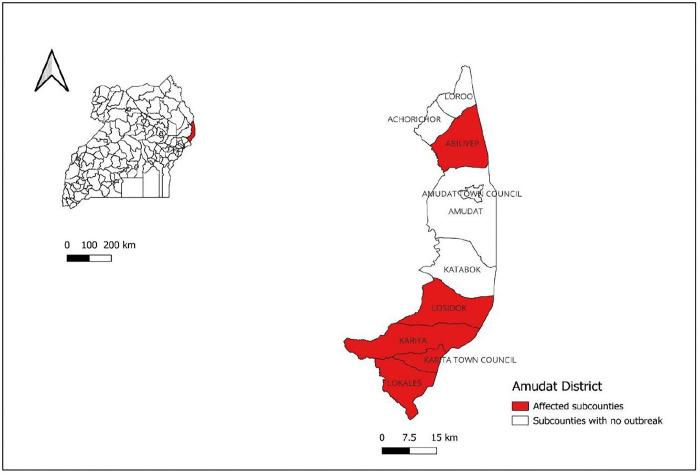 Fig 1
Fig 1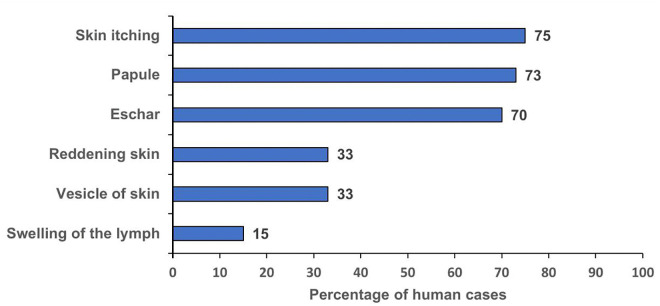 Fig 2
Fig 2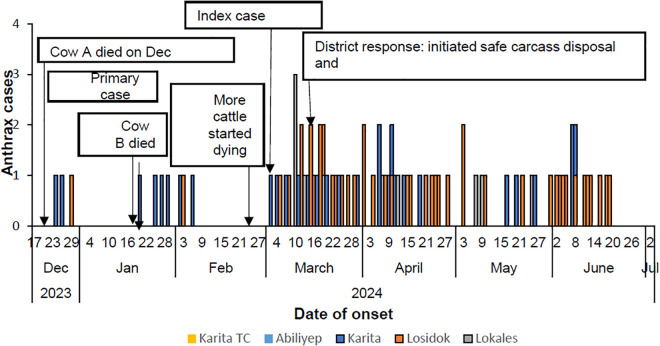 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacillus and Francisella bacterial research · Poxvirus research and outbreaks · Zoonotic diseases and public health
Background
Anthrax is a zoonotic disease caused by Bacillus anthracis, a gram-positive, aerobic, spore-forming bacterium that affects both animals and humans [1]. Globally, anthrax continues to pose a significant public health threat, especially in underserved rural regions across Africa and Asia, where an estimated 20,000–100,000 cases occur annually [2,3].The World Health Organization (WHO) recognizes anthrax as one of the neglected zoonotic diseases due to its persistent burden on health and livelihoods in marginalized communities [2].
Livestock typically become infected through ingestion of contaminated feeds or water, inhalation of spores while grazing on land harboring dormant spores, which then germinate into active bacteria within the host [4]. Humans primarily acquire the infection through contact with infected animals or their products, such as meat, hides, skin, and bones [5,6]. The disease manifests in three primary forms in humans: cutaneous, gastrointestinal and inhalational, each associated with a distinct route of exposure and varying incubation periods: cutaneous (2–7 days), inhalational (1–6 days), and gastrointestinal (1–6 days) [7]. Cutaneous anthrax is the most frequently reported form, accounting for approximately 95% of human cases and may lead to fatality rates as high as 20% if not treated [2,8]. Pastoralist and agro-pastoralist communities are particularly at risk due to frequent human-animal interactions and reliance on livestock for livelihood.
In Uganda, close human-animal interactions, particularly in pastoralist regions, increase the risk of zoonotic disease transmission [9]. Between January 2017 and April 2023, the country documented 19 anthrax outbreaks across various regions, predominantly within the cattle corridor that spans the north, east, and west [10–13]. According to 2018 surveillance data, there were186 human anthrax cases and 721 livestock deaths attributed to the disease [14,15].
On December 28, 2023, a 10-year-old child from Kakworobu Village, a rural community in Amudat District, sought medical attention at a local health facility with symptoms consistent with cutaneous anthrax: an itchy lesion on the shoulder that progressed to a black eschar, accompanied by generalized body weakness. This health facility was the first to identify suspected cases of anthrax, signaling the onset of a potential outbreak. Sporadic cases continued to appear into early March 2024, prompting health authorities to alert district officials on March 5, 2024. Laboratory tests confirmed anthrax in human samples on March 25, 2024.This marked the first documented anthrax outbreak in the district, highlighting the urgent need for a public health response. We investigated to assess the outbreak’s magnitude, identify associated risk factors, and recommend control and prevention measures.
Methods
Outbreak area
Amudat District is located in north-eastern Uganda, within the Karamoja sub-region. shares borders with Kenya to the east, Moroto District to the north, Nakapiripirit to the west, and Kween and Bukwo District to the south. The district has a population of approximately 157,800 according to Uganda Bureau of Statistics (UBOS) and people are predominantly nomadic pastoralists. Amudat District is administratively divided into 10 lower local government units, consisting of 2 urban town councils and 8 rural sub-counties. The town councils are: Amudat Town Council and Karita Town Council. The sub-counties are: Loroo, Abiliyep, Katabok, Kangorok, Lokales, Losidok, Achorichori, and Karita (Fig 1).
Location of Amudat District in Uganda (map drawn using QGIS browser 3.10.2).
Case definition and finding
We defined a suspected cutaneous anthrax case as acute onset of ≥2 of the following: skin lesions (papule, vesicle, or eschar) on exposed areas such as the hands, forearms, shoulders, back, thighs or face, localized itching, redness, swelling, or regional lymphadenopathy, in Amudat residents from December 2023–June 2024.
A confirmed case was a suspected case testing PCR-positive for Bacillus anthracis.
To identify cases, we reviewed health facility records at health facilities serving the affected community and conducted active community case searches in collaboration with the community health workers.
Descriptive epidemiology
We performed descriptive epidemiology on the line-listed case-patients. Case-patients were described by time, place, person characteristics. We constructed an epidemic curve to depict the distribution of cases over time. Attack rates were calculated as the number of new anthrax cases during the outbreak period divided by the total population at risk, multiplied by 100,000 using statistics based on district population estimates obtained from the District Biostatistician and stratified by age group, sex, and sub-county. Choropleth maps were developed to illustrate the geographic distribution of cases across sub-counties.
Laboratory investigations
Samples were collected from humans, animals, and the environment during the outbreak investigation. For human cases, swabs were obtained from the active edges of cutaneous lesions (eschars) using sterile swabs. From cattle carcasses, tissue samples (ear notch or muscle), and swabs of unclotted blood oozing from natural body orifices (nose, eyes, anus) were collected where available, following strict biosafety precautions. Soil samples were also obtained from sites where cattle had died suddenly. All samples were placed in sterile containers, properly labeled, and maintained on ice during transport.
Human samples were triple-packaged and transported through the national specimen hub system to the Uganda Virus Research Institute (UVRI) laboratory in Arua District, while animal and environmental samples were sent to the National Animal Disease Diagnostics and Epidemiology Centre (NADDEC) laboratory in Entebbe, Uganda. At both laboratories, samples were processed using standard real-time PCR protocols for the detection of Bacillus anthracis DNA, following WHO guidelines for anthrax confirmation. Positive and negative controls were included in all assays to ensure accuracy. Laboratory staff adhered to biosafety level 2 (BSL-2) procedures throughout sample handling and analysis.
Environmental investigations
We inspected grazing sites and areas where cattle had died suddenly, focusing on carcass disposal practices to identify potential contamination sources. Soil samples were collected specifically from these sites where cattle had died, as they were considered high-risk for environmental contamination with Bacillus anthracis spores and were taken to the laboratory for analysis.
Additionally, we assessed the livestock vaccination status within the affected sub-counties.
Hypothesis generation
To generate hypotheses, we conducted face-to-face, structured interviews with 40 case-patients using a pre-tested questionnaire to identify various exposures associated with contracting anthrax. These exposures included: butchering of carcasses, use of cattle hides as bedding, and digging up buried animal remains during farming.
Case-control study
We carried out an unmatched case-control study to identify risk factors for anthrax. A total of 40 case-patients, including all confirmed and suspected cases who could be located, were enrolled from the 102 cases identified during the outbreak.
For each enrolled case, three controls were selected randomly from the nearest households, resulting in a 1:3 case-to-control ratio. Controls were screened to ensure they had no clinical signs or symptoms of anthrax before enrolment. The remaining 62 case-patients were not included due to the nomadic nature of the Pokot population, which made it challenging to locate and follow up on some case-patients, especially those who had migrated or were unreachable during the study period. Using structured questionnaires, we collected demographic characteristics (age, sex, and sub-county) and potential exposures (butchering of carcasses from cattle that had died suddenly, skinning carcasses, carrying the meat of cattle that died suddenly, use of cattle hides as bedding from carcasses of cattle that died suddenly, and digging out animal remains).
Data were analyzed using Epi Info software. Crude odds ratios (OR) were computed at the bivariate analysis. Factors found significant at this level were included in a multivariable logistic regression model to calculate adjusted odds ratios (aOR), with significance set at p < 0.05. A common reference group analysis was also conducted to evaluate risk associated with multiple exposure combinations [16].
Ethical considerations
This outbreak investigation was in response to a public health emergency and was therefore determined to be non-research. The Ministry of Health (MoH) gave permission to investigate this outbreak. In agreement with the International Guidelines for Ethical Review of Epidemiological Studies by the Council for International Organizations of Medical Sciences (1991) and the Office of the Associate Director for Science, US CDC/Uganda, it was determined that this activity was not human subject research and that its primary intent was public health practice or disease control activity (specifically, epidemic or endemic disease control activity). This activity was reviewed by the US CDC and was conducted consistent with applicable federal law and CDC policy. §§See, e.g., 45 C.F.R. part 46, 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq. All experimental protocols were approved by the US CDC human subjects review board (The National Institute for Occupational Safety and Health Institutional Review Board) and the Uganda MoH and were performed in accordance with the Declaration of Helsinki. Permission to conduct the outbreak response was also granted by Amudat District Local Government. Prior to data collection, informed consent was obtained from all the participants who were aged 18 years or older (legal age in Uganda). For those below 18 years, consent was sought from their parents/guardians and assent was also obtained from them to participate in the study.
Results
Descriptive epidemiology
We identified a total of 102 case-patients during the outbreak. Forty were investigated and interviewed, of whom seven were confirmed by PCR as cutaneous anthrax and 33 were suspected cases. The overall attack rate was 169 per 100,000 population, with all cases presenting in the cutaneous form.
The mean age of the 40 cases was 24 years (range: 7 months–70 years), with the cases aged 40 years and above being the most affected (attack rate: 229/100,000), and the under 5 years group the least affected (attack rate: 88/100,000). Males had a higher attack rate (196/100,000) compared to females (138/100,000). Geographically, Losidok Sub-county recorded the highest attack rate (452/100,000), whereas Abiliyep Sub-county had the lowest (8/100,000) (Table 1).
Table 1: Attack rates by age, sex, sub-county among case-patients during a cutaneous anthrax outbreak, Amudat District, December 2023–June 2024.
Among 40 case-patients, skin itching (75%), skin swelling (73%) and eschar (70%) were the most common signs and symptoms of illness. (Fig 2).
Distribution of clinical symptoms of anthrax case-patients during an anthrax outbreak, Amudat District, December 2023–June 2024 (n = 40).
On December 22, 2023, cow A died in neighboring Kween District. Its carcass was then butchered, and its meat transported to Amudat; two days later, the first suspected human case emerged with signs and symptoms suggestive of cutaneous anthrax including skin itching on the shoulders, general body weakness, and eschars on the hands and visited Karita HCIV in Karita Sub-county on December 28, 2023. On January 20, 2024, cow B died in Karita Sub-county, and shortly thereafter, additional human cases emerged. Towards the end of February 2024, over 100 cattle died, this was the time cattle were returning from Kween District and it was followed by marked increase in human cases. On March 3, 2024, the index case was identified, prompting an alert to the district, on March 4, 2024, the Moroto Regional Emergency Operations Centre (REOC) was notified. On March 15, 2024, a joint team from the district and REOC verified the alerts at Karita HC4. It took 66 days to detect the outbreak, one day to be notified and 12 days for the district to initiate response.
The cases were initially confined to Karita Sub-county but later spread to Losidok and Lokales Sub-counties. We observed that during the outbreak, cattle frequently moved across sub-counties and district borders in search of pasture.
A noticeable surge that occurred in March 2024, prompted the district to respond on March 15,2024. The carcasses of infected cattle were safely disposed of to prevent further spread, and awareness campaigns were conducted in the affected sub-counties to help reduce transmission (Fig 3).
Distribution of cutaneous anthrax cases across sub-counties, Amudat District, December 2023–June 2024.
Laboratory findings
Among 16 human skin lesion swabs collected, seven (44%) tested positive for B. anthracis by PCR at UVRI. The remaining 9 samples were negative. All six samples from the cattle carcasses and two soil samples tested negative at NADDEC.
Environmental assessment findings
In Losidok Sub-county, we observed scattered cattle bones, suggesting prior improper disposal of animal carcasses. In Karita, we noted discarded hides that respondents reported had been used as bedding. In one family with two affected children, the hide used as bedding had been recently obtained (approximately two months prior) from a donor returning from Kween District, an area with prior anthrax outbreaks. Additionally, none of the respondents reported vaccinating their livestock against anthrax before the outbreak.
Hypothesis generation findings
Of the 40 participants interviewed during hypothesis generation, 33(83%) reported butchering of carcasses from cattle that had died suddenly. Additionally, 33% respondents indicated they were involved in digging up animal remains (bones) during cultivation and 30% admitted use of cattle hides as bedding. We therefore considered that the use of cattle hides as bedding, digging out animal remains and the butchering of carcasses from cattle that died suddenly could be associated with the anthrax outbreak in Amudat District. (Table 2).
Table 2: Hypothesis generation among case-patients during a cutaneous anthrax outbreak, Amudat District, December 2023–June 2024 (n-40).
Case control study findings
Use of cattle hides from cattle that had died suddenly as bedding was associated with a substantially higher likelihood of cutaneous anthrax (aOR = 12, 95% CI: 2.7–52). Furthermore, individuals who butchered carcasses from cattle that died suddenly were 6 times more likely to develop cutaneous anthrax compared to those who did not (aOR = 6, 95% CI: 1.84–19) (****Table 3).
Table 3: Exposure factors associated with an anthrax outbreak, Amudat District, Uganda, December 2023–June 2024.
Compared to the unexposed group (those with no contact with the dead cattle), individuals who engaged in more exposure activities had higher odds of contracting anthrax. Those who only butchered had an odds ratio (OR) of 6.9 (95% CI: 2.6–18). The odds were higher for those who butchered and carried cattle parts (OR=11, 95% CI: 1.2–96), butchered and skinned (OR=14, 95% CI: 3.5–56), and for those who performed all three activities butchering, carrying cattle parts, and skinning (OR=17, 95% CI: 1.6–219) (****Table 4).
Table 4: Common reference analysis of risk factors associated with cutaneous anthrax, Amudat, December 2023–June 2024.
Discussion
This outbreak represents the first documented case of anthrax in Amudat District. Our investigation identified key risk factors, including direct exposure to cattle hides and involvement in butchering activities, with a synergistic effect of these exposures amplifying the cumulative risk. Additionally, there was a lack of prior vaccination among livestock in the district. The outbreak affected five sub-counties and no human death was reported, although livestock deaths occurred in several affected areas. While the outbreak response faced significant delays in detection and response, the one-day notification requirement for the 7-1-7 metrics was met.
Using cattle hides as bedding emerged as a major risk factor for cutaneous anthrax in Amudat District, with exposed individuals more likely to develop the disease. Contaminated hides provide a plausible route for Bacillus anthracis transmission, consistent with previous studies from other countries [17]. To our knowledge, this is the first outbreak investigation in Uganda to suggest that using cattle hides from suddenly deceased cattle as bedding may increase the risk of cutaneous anthrax. However, the relatively small number of participants and the wide confidence intervals limit the precision of these estimates and the strength of the evidence. Future studies with larger sample sizes are needed to confirm this association and better quantify the risk. Nonetheless, these findings highlight the need for increased community awareness and the promotion of safer alternatives, with involvement of cultural and community leaders to ensure effective communication of preventive measures.
Butchering of carcasses of cattle suspected to have anthrax was also a key factor in the transmission of anthrax to humans. These findings are consistent with previous studies that have identified exposure like butchering of infected animals as a significant risk factor for human anthrax [14,18–20]. Given the risk of recurrent outbreaks in Uganda, ongoing community education on safe carcass disposal is essential to prevent future outbreaks.
The 7-1-7 metrics revealed a two-month delay in detecting and responding to the outbreak, illustrating challenges in early recognition of anthrax in previously unaffected district. Delays were likely exacerbated by limited awareness of the disease among health care providers. This delay mirrors challenges faced globally in managing public health threats [21,22]. To improve global health security, it is essential to strengthen early detection systems, enhance surveillance, train local health workers, and ensure better communication and coordination among stakeholders for faster, more effective responses to future outbreaks.
These findings have important public health implications. Targeted interventions in nomadic pastoral communities should address behaviors that increase risk, including using cattle hides as bedding and butchering of cattle carcasses. Health education campaigns should engage community and cultural leaders to promote behavioral change and safer practices. To reduce livestock-to-human transmission, routine vaccination of animals should be prioritized, as none of the livestock in the affected district had received prior vaccination. Integrated human-animal surveillance under a One Health framework is essential to ensure early detection and rapid response to future zoonotic threats.
One key limitation of this study is the likely underreporting of gastrointestinal (GI) anthrax cases, as symptoms may mimic other common GI conditions, leading to misdiagnosis. This, combined with the unfamiliarity of local healthcare providers with anthrax, given its novelty in the district likely delayed recognition and reporting, resulting in an underestimation of the outbreak’s true magnitude. Additionally, some exposures were self-reported and involved a small number of cases, which may introduce recall bias. Nevertheless, these findings provide important insight into key risk factors for cutaneous anthrax in this population.
Conclusion
This outbreak of cutaneous anthrax was primarily associated to use of cattle hides as bedding and butchering of carcasses from cattle that had died suddenly. The response was hindered by delayed outbreak detection. Prevention strategies should focus on community education, routine livestock vaccination, and safe handling and disposal of carcasses. Strengthening integrated surveillance systems across human and animal health sectors, in line with the One Health framework, could improve early detection and response to future outbreaks.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alam ME, Kamal MM, Rahman M, Kabir A, Islam MS, Hassan J. Review of anthrax: A disease of farm animals. J Adv Vet Anim Res. 2022;9(2):323–34. doi: 10.5455/javar.2022.i 599 35891653 PMC 9298093 · doi ↗ · pubmed ↗
- 2Kasradze A, Echeverria D, Zakhashvili K, Bautista C, Heyer N, Imnadze P, et al. Rates and risk factors for human cutaneous anthrax in the country of Georgia: National surveillance data, 2008-2015. P Lo S One. 2018;13(2):e 0192031. doi: 10.1371/journal.pone.0192031 29415029 PMC 5802846 · doi ↗ · pubmed ↗
- 3Badri R, Uwishema O, Wellington J, Thambi VD, Pradhan AU, Adanur I, et al. Anthrax outbreak amidst the COVID-19 pandemic in Africa: Challenges and possible solutions. Ann Med Surg (Lond). 2022;81:104418. doi: 10.1016/j.amsu.2022.104418 36000069 PMC 9389518 · doi ↗ · pubmed ↗
- 4CDC. Anthrax. 2025 [cited 2025 Aug 26]. About Anthrax. Available from: https://www.cdc.gov/anthrax/about/index.html
- 5Anthrax – Thailand. https://www.who.int/emergencies/disease-outbreak-news/item/2025-DON 573. Accessed 2025 August 26.
- 6Xin W, Yue N, Wang J. A review of epidemiological characteristics, risk factors, and prevention strategies of human anthrax in China. Decoding Infection and Transmission. 2024;2:100024. doi: 10.1016/j.dcit.2024.100024 · doi ↗
- 7Zasada A. Injectional anthrax in human: A new face of the old disease. Adv Clin Exp Med. 2018;27(4).10.17219/acem/6838029533547 · doi ↗ · pubmed ↗
- 8Nayak P, Sodha SV, Laserson KF, Padhi AK, Swain BK, Hossain SS, et al. A cutaneous Anthrax outbreak in Koraput District of Odisha-India 2015. BMC Public Health. 2019;19(Suppl 3):470. doi: 10.1186/s 12889-019-6787-0 32326927 PMC 6696704 · doi ↗ · pubmed ↗