Herpes simplex virus type 2 implicated in a case of acute disseminated encephalomyelitis
Stuart Booth, Igor Starinskij, Stuart Gallacher, Peter Garmany

TL;DR
A rare case links herpes simplex virus type 2 to acute disseminated encephalomyelitis, a neurological disorder.
Contribution
This is the first reported case of ADEM associated with HSV-2, expanding the known viral triggers.
Findings
ADEM was diagnosed in a patient with HSV-2 confirmed via PCR.
The patient showed neurological improvement after treatment with aciclovir and dexamethasone.
Neurological sequelae remained despite rehabilitation.
Abstract
Introduction. Acute disseminated encephalomyelitis (ADEM) is a well-described neurological disorder that follows acute infection, vaccination and organ transplantation. It is characterized by sudden and widespread areas of inflammation in the central nervous system. Previous case reports have described ADEM with evidence of either recent or current herpes simplex virus type 1 infection. However, here, we report a rare, to our knowledge never before documented, case of ADEM associated with herpes simplex virus type 2 (HSV-2). Case report. A 20-year-old man presented with weakness and sensory disturbance to the lower limbs, which had gradually progressed over the preceding 7 days, with associated fever, urinary retention and bowel incontinence. Magnetic resonance imaging was in keeping with a diagnosis of ADEM with mainly spinal involvement. Lumbar puncture revealed lymphocytic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
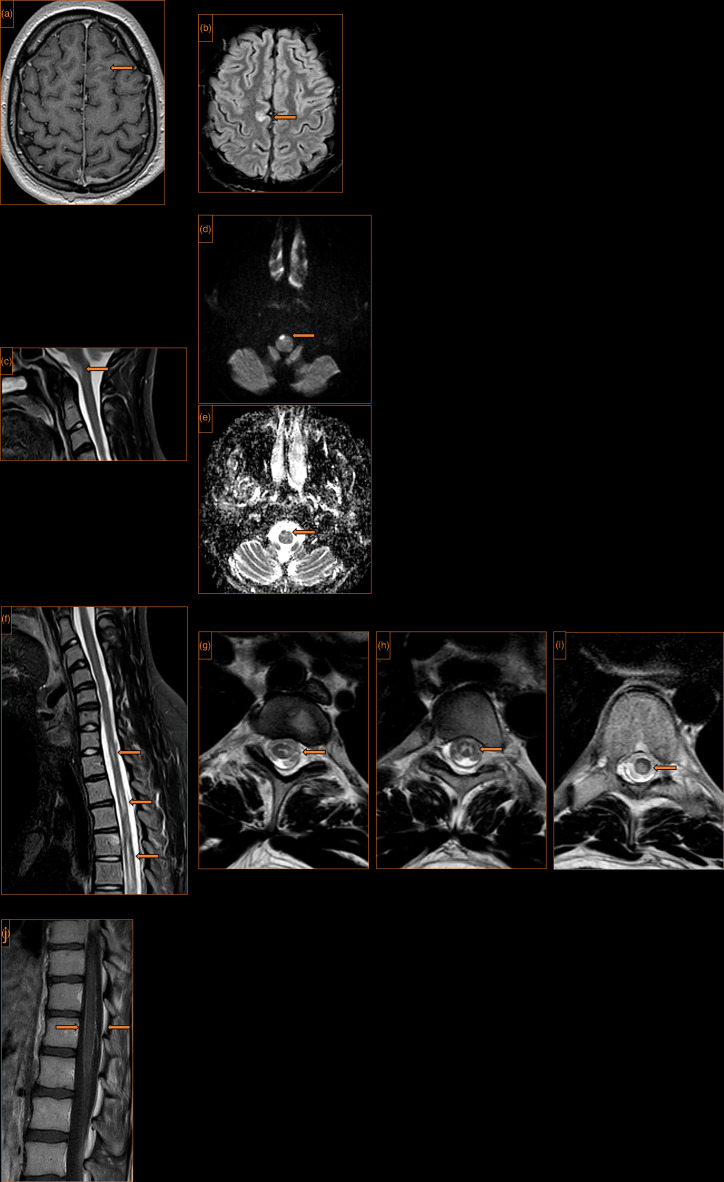 Fig. 1
Fig. 1| Parameter | Reference range | Day 1 of treatment | Day 12 of treatment | Day 26 of treatment |
|---|---|---|---|---|
| Opening pressure | 10–20 cmH2O | 20 cmH2O |
| 15 cmH2O |
| Appearance | Clear colourless fluid | Straw-coloured fluid | Straw-coloured fluid | Clear colourless fluid |
| Red cell count | <5/mm3 | 597/mm3 | 1,360/mm3 | <5/mm3 |
| White cell count | <5/mm3 | 425/mm3 | 41/mm3 | 10/mm3 |
| Polymorphs |
| 20% | 10% |
|
| Lymphocytes |
| 80% | 90% |
|
| Protein | 0.1–0.5 g l−1 | 3.3 g l−1 | 0.71 g l−1 | 0.46 g l−1 |
| Glucose | 2.5–4.5 mmol l−1 | 1.2 mmol l−1 | 1.7 mmol l−1 | 2.7 mmol l−1 |
| HSV-2 PCR (Ct value) |
| Detected (22.2) | Detected (33.5) | Not detected |
| HSV-1, VZV, enterovirus, parechovirus PCR |
| Not detected | Not detected | Not detected |
| Parameter | Sample type | Result (reference range, if applicable) |
|---|---|---|
| 16s rDNA real-time PCR | CSF | No rDNA detected |
| CSF | Negative | |
| CSF | Negative | |
| Oligoclonal bands | Paired CSF and serum | Normal |
| Antineutrophil cytoplasmic antibodies | Serum | Negative |
| Antinuclear antibodies | Serum | Negative |
| Anti-streptolysin O titre | Serum | 99 U ml−1 (<200 U ml−1) |
| Aquaporin4 antibodies | Serum | Negative |
| Serum | Negative | |
| Ganglioside screen* | Serum | Negative |
| Neuronal antibodies† | Serum | Negative |
| Myelin oligodendrocyte glycoprotein antibodies | Serum | Negative |
| Myeloperoxidase antibodies | Serum | <0.2 IU ml−1 (<3.5 IU ml−1) |
| Proteinase-3 antibodies | Serum | <0.2 IU ml−1 (<2.0 IU ml−1) |
| Hepatitis B surface antigen | Plasma | Negative |
| Hepatitis C antibodies | Plasma | Negative |
| HIV antibodies/antigen | Plasma | Negative |
| HSV total antibodies during admission | Plasma | Negative |
| HSV total IgM during admission | Plasma | Negative |
| HSV-1 IgG during admission | Plasma | Negative |
| HSV-1 IgG 7 months post-presentation | Serum | Negative |
| HSV-2 IgG during admission | Plasma | Negative |
| HSV-2 IgG 7 months post-presentation | Serum | Positive |
| Rapid plasma reagin | Plasma | Negative |
| Plasma | Negative | |
| Plasma | Negative |
| Analyte | No. of positive samples | Mean Ct (range) |
|---|---|---|
| HSV-1 | 20 | 31.1 (22.8–37.3) |
| HSV-2 | 13 | 30.6 (25.9–36.3) |
| Varicella zoster virus | 26 | 31.2 (27.0–36.9) |
| Enterovirus | 23 | 33.9 (29.9–39.5) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Multiple Sclerosis Research Studies · Viral Infections and Immunology Research
Data Summary
Data for cerebrospinal fluid multiplex PCR result comparison were extracted from the laboratory information management system using Dedalus Telepath version 1.9 by a data manager independent from the project. The following parameters were retrieved: patient demographic information, location at time of request, sample collection date, result authorization date, sample type, test interpretation results and cycle threshold values. The data were exported in XLSX format for processing and analysis. Samples obtained from the specific patient described in the report, as well as samples that did not complete testing, were excluded. The final dataset comprised 3,270 samples collected between 27 February 2019 and 30 October 2021. All information except for specimen type, collection date and testing results was removed to preserve patient confidentiality.
Introduction
Acute disseminated encephalomyelitis (ADEM) is a well-described neurological disorder that can complicate acute infection, vaccination and organ transplantation and often leads to acute urinary retention [17]. Preceding infection is not part of a formal definition of ADEM, which is considered an immune-mediated condition, although it is almost certainly one of the major triggers [8].
There are case reports of ADEM with evidence of recent or current herpes simplex virus (HSV) type 1 (HSV-1) infection as well as a survey reporting HSV genome detection in cerebrospinal fluid (CSF) in one out of three ADEM cases [912]. In contrast, there is no literature, to the best of the authors’ knowledge, describing an association between herpes simplex virus type 2 (HSV-2) and presentations of ADEM.
Case presentation
A 20-year-old man presented to the emergency department of a large inner city teaching hospital complaining of weakness and sensory disturbance affecting his lower limbs which had gradually progressed over the preceding 7 days.
The patient described initial altered sensation in his left foot with associated limp which, over a period of 4 days, developed to painful paraesthesia of his entire left leg. On the morning of attending hospital, he reported a complete loss of sensation to both legs and an inability to stand or walk. At this time, there was associated urinary incontinence. He required being carried into the emergency department due to bilateral limb weakness.
He was fit and well prior to this, except for a single episode of pharyngitis and tonsillar exudate 14 days preceding initial neurological symptoms, which fully resolved with 7 days of oral phenoxymethylpenicillin (500 mg four times daily).
There was no history of recent travel or unwell contacts. He had been immunized fully in line with the standard UK vaccination schedule including coronavirus disease 2019 vaccination. There was no family history of inherited conditions including no previous familial neurological condition.
He had one female sexual partner of around 2 months, was heterosexual and reported no unprotected sex. There was no evidence of genital blistering or ulceration, and he did not report any genitourinary symptoms.
On examination, he was noted to have Medical Research Council (MRC) grade 0/5 power in both lower limbs, with complete sensory loss (pin prick, light touch, vibration and proprioception) from the T10 through S5 dermatomes. Both legs were areflexic with flaccid muscle tone. He was found to be in urinary retention, requiring urinary catheterization and was incontinent of faeces. He was febrile with a temperature of 38.8 °C, and observations were otherwise within normal parameters.
Computed tomography head scanning was performed with intravenous contrast and was unremarkable. Blood laboratory results, including full blood count, C-reactive protein, liver function and renal function, were essentially within normal limits, while CSF results can be found in Table 1, although viral PCR results were not available at this point.
Empirical treatment was started (once daily unless stated otherwise):
intravenous ceftriaxone 2 g twice daily,intravenous aciclovir 10 mg kg^−1^ three times daily,oral dexamethasone 10 mg twice daily,oral rifampicin 720 mg,oral isoniazid 300 mg,oral pyrazinamide 1,800 mg,oral ethambutol 1,200 mg,oral pyridoxine 10 mg.
At this point, the working diagnosis was a central nervous system (CNS) infection, such as CNS tuberculosis, but other common bacterial and viral pathogens were also covered with the empirical regimen.
At day 10 of admission, he reported new paraesthesia to both feet which progressed over the following 2 days to involve his entire lower limbs. On day 12, he was noted to have light touch and pinprick sensation to the soles of both feet. On day 13, it was noted that motor function was recovering with hip adduction power bilaterally at MRC grade 1/5.
Direct Gram staining of CSF was negative, and bacterial culture was performed with no growth of bacterial pathogens by 48-h incubation. Bacterial PCR was negative for Haemophilus influenzae, Neisseria meningitidis and Streptococcus pneumoniae. A total of 10 ml of CSF was sent for mycobacterial culture with no growth at 42-day incubation. The CSF samples underwent PCR testing using an in-house assay for HSV-1, HSV-2, varicella zoster virus, enteroviruses and parechoviruses. HSV-2 was detected in the first CSF sample at a cycle threshold (Ct) of 22.2. The patient was extensively investigated for infectious and autoimmune conditions, and the results can be found in Table 2.
Electromyography showed mild abnormalities in lower limb motor studies with preserved sensory studies but no clear motor activity in the lower limbs in keeping with a central pathology. T1, T2, diffusion weighted, short tau inversion recovery magnetic resonance imaging (MRI) of the head and spine with gadolinium enhancement was performed with findings largely confined to within the brain stem and spinal cord. There were multiple intramedullary cord lesions. The appearances were in keeping with a diagnosis of ADEM (Fig. 1). Predominant spinal involvement and enhancement of the spinal meninges are uncommon features but previously described [1314].
MRI of the head and spine. (a) Axial T1 post-gadolinium contrast of the brain. Focal leptomeningeal enhancement high left frontal lobe (arrow). (b) Axial T2 fluid-attenuated inversion recovery of the brain. A focal high signal lesion at the parafalcine cortex right frontal lobe (arrow). (c) Sagittal T2-weighted images of the craniocervical junction. A high signal lesion in the anterior medulla oblongata (arrow). (d) Axial diffusion-weighted imaging of the craniocervical junction. Restricted diffusion within the lesion (arrow). (e) Complementary low signal on the apparent diffusion coefficient map (arrow). (f) Sagittal T2-weighted images of the cervicothoracic spine. Multiple focal high signal lesions within the spinal cord, measuring up to two vertebral levels in length (arrows). These lesions are associated with cord swelling and did not enhance after contrast. (g−i) Axial T2-weighted images at three levels of the dorsal spine. Heterogeneity of location with the cord substance, with some predilection for grey matter (arrows). (j) Sagittal T1 of the lumbar spine with intravenous gadolinium contrast. Florid leptomeningeal enhancement over the surface of the conus (arrows).
A repeat lumbar puncture was performed on day 26 of admission, prior to completion of intravenous antiviral therapy. CSF testing results across the admission are summarized in Table 1. CSF microscopy with Gram staining, bacterial culture and viral PCR screen, excluding HSV-2, remained negative throughout.
MRI at this time showed interval improvement in intracranial and spinal appearances, with no new evidence of leptomeningeal enhancement and previous findings less appreciable in keeping with response to treatment.
Treatment was rationalized as culture results became available, with tuberculosis treatment continuing until negative mycobacterial culture. Intravenous aciclovir was continued for a total of 28 days before being switched to 500 mg valaciclovir once daily for a total of 6 months. Dexamethasone was discontinued at day 10 after liaison with the clinical neurology service.
He underwent extensive physiotherapy and had a gradual progressive improvement in motor and sensory function. On day 90 of admission, the patient was transferred to the physical disability rehabilitation unit (PDRU). At this time, he had MRC grade 2/5 bilateral lower limb weakness with normal sensation to pinprick and light touch, although he remained areflexic with flaccid muscle tone in T10-S5 myotomes. He remained catheterized due to multiple failed trials without catheter and was intermittently incontinent of faeces.
The patient underwent a further 45 days of physical rehabilitation in the PDRU. By the time of discharge, power had improved to MRC grade 4/5 on his right and 3/5 on his left lower limb. He was mobilizing with a wheelchair and was independent with all transfers and self-care. Bowel function normalized; however, the patient continued to require intermittent self-urinary catheterization 2–3 times weekly due to incomplete bladder emptying.
The patient made continued improvement over the next 3 years. His leg power had progressed to MRC grade 5/5 on the right and 4+/5 on the left and he had become independently mobile with elbow crutches. He was able to drive, work in retail for around 5 h per day and attend a gym. However, neurological sequelae, in the form of lower limb spasticity and chronic urinary retention, remain.
Discussion
This is a case of ADEM with strong molecular and serological evidence of a concurrent HSV-2 CNS infection.
Acute haemorrhagic leucoencephalitis is the most severe and rapidly progressive form of ADEM [1516]. Nonetheless, the absence of evidence of cerebral bleeding in this patient and non-hyperacute course both make this diagnosis unlikely.
CSF PCR was used as the primary aetiological diagnostic tool during the acute phase of illness. PCR does not directly measure the number of replicating virions, but the Ct values obtained using this method correlate with both disease severity and duration of illness [1718]. To put the results into context, data from CSF PCR assays performed in the local virology laboratory over a 20-month period between 2019 and 2021 were reviewed (Table 3). In this case, the Ct of 22.2 is lower than ever obtained for any pathogen in the examined timeframe, compatible with an early phase of a severe infection.
A few alternative explanations should be considered. Firstly, HSV-2 encephalitis, although uncommon in general, is in keeping with the finding of a high amount of HSV-2 DNA in the CSF [19]. On the other hand, although the neurological features of both ADEM and HSV encephalitis can be diverse, there were no clinical signs of generalized cerebral inflammation, such as seizures and reduced consciousness level. In addition, widespread MRI findings were in keeping with ADEM rather than HSV-2 encephalitis, which is often confined to the temporal and frontal lobes [419]. Secondly, postinfectious immune-mediated encephalitis is often described as one of the forms of ADEM but can also present differently [520]. It can be distinguished from ADEM by an absence of new lesions compared to the areas affected by HSV during the first episode of overt encephalitis with negative viral PCR during the second presentation [20]. Here, there was no preceding illness suggestive of HSV-2 encephalitis and the viral PCR is positive. Finally, acute HSV-2 CNS infection could have coincided with ADEM with distinct aetiology. In this case, pharyngitis antecedent to neurological presentation was indeed diagnosed and theoretically could have been the original cause of autoimmune neurological disease. However, its causative agent had never been identified; hence, it is impossible to conclusively link this presentation to the past event.
Multiple sclerosis (MS), the first attack of which can be highly similar to ADEM, should be thought of when evaluating the long-term prognosis of a patient with ADEM [2122]. All three proposed differentiation criteria (atypical sign – paraplegia, absence of oligoclonal bands and grey matter involvement) present in this case were supportive of ADEM rather than MS [23]. To date, our patient had not experienced recurrent or new symptoms suggestive of MS.
One limitation to the primary diagnosis is that a biopsy with relevant histological investigations is required for a final confirmation of ADEM. However, a close temporal association, robust detection by repeated PCR assays as well as the known role of a closely related HSV-1 in ADEM pathogenesis strongly support HSV-2 as the neurological disease-causing agent here. Additionally, we demonstrated HSV-2 type-specific immunoglobulin G seroconversion (Table 2), further solidifying the case for an acute HSV-2 CNS infection, while imaging was most in keeping with ADEM rather than alternative neurological conditions.
In summary, we describe a case of ADEM affecting primarily the spinal cord with strong molecular and serological evidence of HSV-2 CNS infection. The case was treated with a variety of antimicrobials, notably aciclovir, and a 10-day course of dexamethasone. The patient had a slow but steady improvement in neurological function over a period of months, but years later, neurological sequelae remain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Garg RK Acute disseminated encephalomyelitis Postgrad Med J 200379111710.1136/pmj.79.927.1112566545 PMC 1742586 · doi ↗ · pubmed ↗
- 2Leake JAD Albani S Kao AS Senac MO Billman GF et al Acute disseminated encephalomyelitis in childhood: epidemiologic, clinical and laboratory features Pediatr Infect Dis J 20042375676410.1097/01.inf.0000133048.75452.dd 15295226 · doi ↗ · pubmed ↗
- 3Silvia MT Licht DJ Pediatric central nervous system infections and inflammatory white matter disease Pediatr Clin North Am 2005521107112610.1016/j.pcl.2005.03.00316009259 · doi ↗ · pubmed ↗
- 4Stone MJ Hawkins CP A medical overview of encephalitis Neuropsychol Rehabil 20071742944910.1080/0960201060106943017676529 · doi ↗ · pubmed ↗
- 5Greenlee JE Encephalitis and postinfectious encephalitis Continuum (Minneap Minn)2012181271128910.1212/01.CON.0000423847.40147.0623221841 · doi ↗ · pubmed ↗
- 6Sakakibara R Hattori T Yasuda K Yamanishi T Micturitional disturbance in acute disseminated encephalomyelitis (ADEM)J Auton Nerv Syst 19966020020510.1016/0165-1838(96)00054-98912271 · doi ↗ · pubmed ↗
- 7Sasaki M Ohara S Hayashi R Iwahashi T Tsuyuzaki J Aseptic meningo-radiculo-encephalitis presenting initially with urinary retention: a variant of acute disseminated encephalomyelitis J Neurol 200625390891310.1007/s 00415-006-0131-116502219 · doi ↗ · pubmed ↗
- 8Young NP Weinshenker BG Lucchinetti CF Acute disseminated encephalomyelitis: current understanding and controversies Semin Neurol 200828849410.1055/s-2007-101913018256989 · doi ↗ · pubmed ↗