A Tough Bullet to Swallow
John A. Cooper, Elizabeth Statham, Stephen Brown, Shajan Peter

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
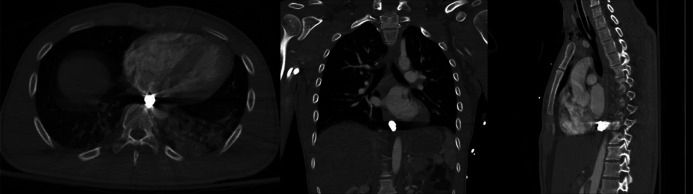 Figure 1
Figure 1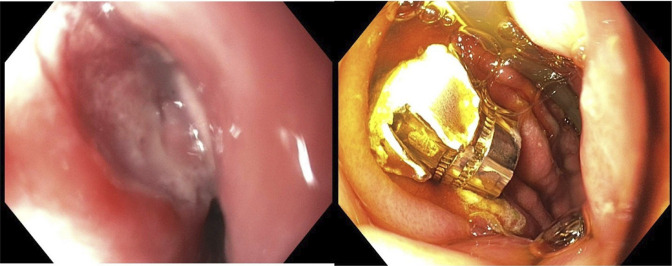 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma Management and Diagnosis · Foreign Body Medical Cases · Traumatic Ocular and Foreign Body Injuries
CASE REPORT
Gunshot wounds to the neck may result in complex injuries, including rare instances of ballistic fragment ingestion or migration.
A 27-year-old man presented after a Gunshot wound to the posterior pharyngeal region. Computed tomography angiogram of the chest and abdomen revealed a ballistic fragment in the posterior mediastinum near the diaphragm, within the expected location of the esophageal lumen (Figure 1). No soft tissue gas, fracture, or vascular injury was present, suggesting esophageal entry rather than direct mediastinal trauma. The patient developed hemiparesis, necessitating MRI, which was delayed due to the metallic fragment. Gastroenterology was consulted for endoscopic removal. Esophagogastroduodenoscopy, performed approximately 36 hours after injury, revealed ulceration in the subglottic space, likely representing the bullet's entry site (Figure 2). The fragment was located distal to the gastroesophageal junction and retrieved using a Roth net (Figure 2).
Computed tomography imaging of swallowed bullet.
Endoscopic image of swallowed bullet.
Early endoscopy in penetrating pharyngeal trauma remains controversial but can be safely performed in stable patients without perforation. In this case, it enabled successful diagnosis and retrieval without complications. Clinicians should consider endoscopy in stable patients with suspected ingestion or migration of ballistic fragments, especially when MRI is indicated and no perforation is evident.
DISCLOSURES
Author contributions: J. Cooper: Manuscript compilation and review; E. Statham, S. Brown, and S. Peter: Manuscript review. S Peter is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.