Predictive values of trigger tools for identifying adverse events in hospitalized patients using a medical record review: a systematic review
Luis Meave Gutiérrez-Mendoza, Elizabeth Manias, Patricia Nicholson

TL;DR
This systematic review evaluates how well trigger tools can identify adverse events in hospitalized patients by analyzing their predictive values.
Contribution
The study provides a comprehensive synthesis of the predictive values of various trigger tools for adverse event detection in hospitals.
Findings
The Institute for Healthcare Improvement Global Trigger Tool has an average positive predictive value of 54.5% and negative predictive value of 80.9%.
The Harvard Medical Practice Study tool has a lower positive predictive value of 43.9% and negative predictive value of 37.8%.
The IHI tool's high sensitivity (86.6%) and moderate specificity (68.2%) suggest it is effective for identifying adverse events.
Abstract
Efforts to identify the prevalence rate of adverse events have been implemented in hospital settings using different methods. The trigger tool method constitutes one option and involves a retrospective review of paper-based, electronic, or hybrid medical records. The aim of the systematic review was to provide a comprehensive description of the predictive value of trigger tools used to identify adverse events in hospitalized patients. A systematic search of MEDLINE, EMBASE, CINAHL, and the Cochrane Library was conducted for studies published between 2000 and October 2024. Eligible studies were peer-reviewed, published in English or Spanish, and reported a trigger tool methodology used to identify the prevalence of adverse events. Two independent reviewers extracted and synthesized the data on study characteristics, methodologies, and outcomes. When reported, tool predictive values were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
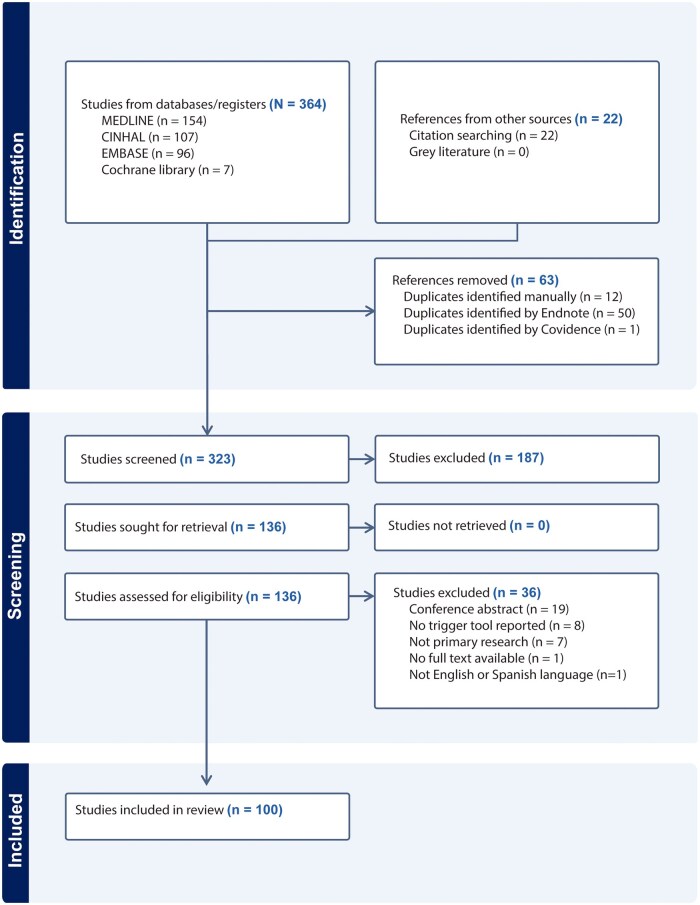 Figure 1
Figure 1| High-income countries | ( |
|---|---|
| Australia [ | |
| Harvard Medical Practice Study | |||||
|---|---|---|---|---|---|
| Sensitivity | Specificity | PPV | NPV | Prevalence of AEs | |
| Aibar (2015) [ | 53.6 | 3.6% | |||
| Brennan (2004) [ | 89.0 | 4.7% | |||
| Kobayashi (2008) [ | 89.3 | 28.0% | |||
| 85.7 | 25.0% | ||||
| Valencia Martín (2022) [ | 73.9 | 11.5 | 37.9 | 37.8 | 11.9% |
| Unbeck (2013) [ | 40.3 | 30.0% | |||
| Total |
|
|
|
|
|
| Study | Country | Type of hospital | Number of hospitals | Sample size number of records | Study period number of months | Type of Medical Records | Type of Trigger Tool | Original and Validated Trigger Tool | Modified, Adapted, or Translated | Developed New Triggers |
|---|---|---|---|---|---|---|---|---|---|---|
| Aibar | Spain | Mixed | 41 | 816 | 1 week | NR | HMPS | No | Yes | No |
| Aikawa | Japan | NR | 1 | 50 | 3 | EMR | IHI-GTT | No | Yes | No |
| Ali | Australia | NR | 4 | 500 | 36 | EMR | Medication-related triggers | No | No | Yes |
| Asavaroengchai | Thailand | Academic | 1 | 576 | 1 | NR | IHI-GTT | Yes | No | No |
| Baker | Canada | Mixed | 20 | 3745 | 12 | NR | HMPS | Yes | No | No |
| Bates | USA | Mixed | 11 | 2809 | 12 | EMR | IHI-GTT | No | Yes | Yes |
| Bjertnaes | Norway | Mixed | 23 | 400 | 3 | NR | IHI-GTT | No | Yes | No |
| Brennan | USA | Mixed | 51 | 30121 | 12 | NR | HMPS | Yes | No | No |
| Brösterhaus | Germany | Academic | 3 | 120 | 2 | EMR & PBMR | IHI-GTT | No | Yes | No |
| Brown | USA | NR | 1 | 426 | 7 | EMR | IHI-GTT | No | Yes | No |
| Carnevali | Belgium | Academic | 1 | 240 | 12 | EMR | IHI-GTT | No | Yes | No |
| Classen | USA | NR | 2 | 65 | NR | PBMR | IHI-GTT | Yes | No | No |
| Classen | USA | Academic | 3 | 795 | 1 | EMR | IHI-GTT | Yes | No | No |
| Cohen | USA | Non-academic | 1 | 580 | 24 | NR | IHI-GTT | No | Yes | No |
| Connolly | Ireland | Mixed | 8 | 3177 | 24 | PBMR | HMPS | Yes | No | No |
| Croft | USA | Academic | 1 | 296 | 11 | NR | IHI-GTT | Yes | No | No |
| Davis | New Zealand | Mixed | 13 | 6579 | 12 | NR | HMPS | Yes | No | No |
| Deilkas | Norway | Mixed | 24 | 40851 | 46 | NR | IHI-GTT | No | Yes | No |
| Deilkas | Norway & Sweden | Mixed | 86 | 30127 | 12 | NR | IHI-GTT | No | Yes | No |
| Deilkas | Norway & Sweden | Mixed | 77 to 84 | 142004 | 72 | EMR | IHI-GTT | No | Yes | No |
| Dolci | Switzerland | Mixed | 2 | 538 | NR | EMR | IHI-GTT | No | Yes | No |
| Dotta | Argentina | Academic | 1 | 320 | 6 | EMR | IHI-GTT | No | Yes | No |
| El Saghir | Switzerland | Academic | 1 | 1008 | 12 | EMR | IHI-GTT | No | Yes | Yes |
| Fajreldines | Argentina | NR | 2 | 830 | 2 | EMR | IHI-GTT | Yes | No | No |
| Franklin | UK | Academic | 1 | 207 | 2 | EMR | IHI-GTT | No | Yes | No |
| Franklin | UK | Academic | 1 | 207 | 2 | EMR & PBMR | IHI-GTT | No | Yes | No |
| Garrrett Jr | USA | Mixed | 25 | 17295 | 36 | EMR | IHI-GTT | Yes | No | No |
| Gómez-López | Spain | Academic | 1 | 464 | 6 | NR | IHI-GTT | No | Yes | Yes |
| Good | USA | Mixed | 12 | 2369 | 12 | NR | IHI-GTT | Yes | No | No |
| Griffey | USA | Academic | 1 | 1726 | 13 | EMR | Emergency care triggers | No | Yes | Yes |
| Griffin and Classen, (2008) [ | USA | NR | 11 | 854 | 12 | NR | IHI-GTT | No | Yes | Yes |
| Grossmann | Switzerland | Non-academic | 1 | 240 | 12 | EMR | IHI-GTT | No | Yes | Yes |
| Gunningberg | Sweden | Private | 63 | 64917 | 48 | EMR | IHI-GTT | No | Yes | No |
| Guzmán-Ruíz | Spain | Non-academic | 1 | 291 | 12 | NR | IHI-GTT | No | Yes | Yes |
| Härkänen | Finland | Academic | 1 | 463 | 12 | EMR | IHI-GTT | No | Yes | No |
| Haukland | Norway | Non-academic | 1 | 6720 | 48 | NR | IHI-GTT | No | Yes | No |
| Hommel | Sweden | Mixed | 24 | 1998 | 36 | EMR & PBMR | IHI-GTT | No | Yes | No |
| Hu | China | Academic | 1 | 480 | 12 | EMR | IHI-GTT | No | Yes | No |
| Hug | USA | Non-academic | 6 | 1200 | 18 | NR | IHI-GTT | No | Yes | No |
| Hwang | Korea | Academic | 1 | 629 | 6 | EMR | IHI-GTT | Yes | No | No |
| Hwang | Korea | Academic | 2 | 1152 | 7 | EMR | IHI-GTT | No | Yes | No |
| Kennerly | USA | Academic | 8 | 16172 | 48 | EMR | IHI-GTT | No | Yes | No |
| Kennerly | USA | Non-academic | 8 | 9017 | 60 | EMR | IHI-GTT | No | Yes | No |
| Kobayashi | Japan | Academic | 1 | 200 | 12 | NR | HMPS | Yes | No | No |
| Kurutkan | Turkey | Academic | 1 | 229 | 12 | NR | IHI-GTT | Yes | No | No |
| Letaief | Tunisia | Academic | 1 | 620 | 12 | NR | HMPS | Yes | No | No |
| Lima-Junior | Brazil | Mixed | 2 | 370 | 12 | NR | HMPS | Yes | No | No |
| Lipitz-Snyderman | USA | Academic | 1 | 400 | 12 | NR | Oncology triggers | No | Yes | Yes |
| Magnéli | Sweden | Mixed | 24 | 1998 | 36 | EMR | IHI-GTT | No | Yes | No |
| Mattsson | Denmark | Academic | 1 | 240 | 12 | NR | IHI-GTT | No | Yes | Yes |
| Mayor | UK (Welsh) | Mixed | 11 | 4833 | 36 | EMR & PBMR | IHI-GTT & HMPS | Yes | No | No |
| Menéndez-Fraga | Spain | Academic | 1 | 240 | 12 | EMR | IHI-GTT | No | Yes | No |
| Merten | Dutch | Mixed | 21 | 7917 | 14 | NR | HMPS | Yes | No | No |
| Mevik | Norway | Academic | 1 | 1920 | 12 | NR | IHI-GTT | No | Yes | No |
| Mevik | Norway | Academic | 3 | 1233 | 10 | EMR & PBMR | IHI-GTT | No | Yes | No |
| Moraes | Brazil | Academic | 1 | 220 | 12 | EMR & PBMR | IHI-GTT | No | Yes | No |
| Mortaro | Italy | Non-academic | 1 | 1320 | 66 | EMR | IHI-GTT | No | Yes | No |
| Mull | USA | Non-academic | 1 | 273 | 1 to 3 | EMR | IHI-GTT | No | Yes | No |
| Müller | South Africa | Academic | 1 | 160 | 8 | PBMR | IHI-GTT | No | Yes | No |
| Naessens | USA | Academic | 1 | 235 | 12 | NR | IHI-GTT | Yes | No | No |
| Naessens | USA | Academic | 3 | 1138 | 61 | NR | IHI-GTT | Yes | No | No |
| Najjar | Palestine | Mixed | 2 | 640 | 4 | NR | IHI-GTT | No | Yes | Yes |
| Nilsson | Sweden | Academic | 1 | 128 | 24 | PBMR | IHI-GTT | No | Yes | No |
| Nilsson | Sweden | Mixed | 63 | 64917 | 48 | NR | IHI-GTT | No | Yes | No |
| Nilsson | Sweden | NR | NR | 2552 | 6 | NR | Mental health triggers | No | Yes | No |
| Nwulu | United Kingdom | Academic | 1 | 467 | 12 | EMR | IHI-GTT | No | Yes | No |
| O’Leary | USA | Academic | 1 | 250 | 12 | EMR | Mix from IHI-GTT & HMPS | No | Yes | No |
| Ock | Korea | NR | 1 | 96 | NR | EMR | IHI-GTT & HMPS | No | Yes | No |
| Otero | Spain | Mixed | 12 | 720 | 3 | NR | Medication-related triggers | No | Yes | Yes |
| Pandya | India | Academic | 1 | 463 | 10 | NR | IHI-GTT | Yes | No | No |
| Paulander | Sweden | Academic | 5 | 60 | 3 | NR | IHI-GTT | No | Yes | No |
| Pérez Zapata | Spain | Academic | 1 | 350 | 12 | EMR | IHI-GTT | No | Yes | No |
| Pérez Zapata | Spain | Mixed | 31 | 1132 | 9 | NR | IHI-GTT | No | Yes | No |
| Pettersson | Sweden | Academic | 1 | 163 | 24 | EMR | IHI-GTT | No | Yes | No |
| Pierdevara | Portugal | Academic | 1 | 90 | 9 | EMR | IHI-GTT | No | Yes | No |
| Pierdevara | Portugal | Academic | 1 | 90 | 9 | NR | IHI-GTT | No | Yes | Yes |
| Resar | USA | Mixed | 54 | 12074 | 46 | NR | IHI-GTT | No | Yes | No |
| Rutberg | Sweden | Academic | 1 | 960 | 48 | EMR | IHI-GTT | No | Yes | No |
| Sajith | Singapore | Academic | 1 | 515 | 6 | EMR & PBMR | Mental health triggers | No | Yes | Yes |
| Samal | USA | Academic | 1 | 88 | 22 | EMR | IHI-GTT | No | Yes | No |
| Sari et al (2015) [ | Iran | NR | 4 | 1162 | 6 | NR | HMPS | Yes | No | No |
| Scarpis | Italy | Academic | 1 | 291 | 3 | PBMR | IHI-GTT | No | Yes | No |
| Schildmeijer | Sweden | NR | 5 | 50 | 8 | NR | IHI-GTT | No | Yes | No |
| Schmied | Austria | Academic | 1 | 421 | 12 | NR | IHI-GTT | No | Yes | No |
| Sekijima | USA | Academic | 1 | 300 | 4 | NR | IHI-GTT | No | Yes | No |
| Sharek | USA | Mixed | 10 | 2400 | 72 | EMR & PBMR | IHI-GTT | Yes | No | No |
| Sousa | Portugal | Mixed | 3 | 1669 | 12 | NR | HMPS | Yes | No | No |
| Storesund | Norway | Mixed | 2 | 700 | 29 | EMR | IHI-GTT | No | Yes | No |
| Suarez | Spain | Academic | 1 | 1440 | 72 | EMR | IHI-GTT | No | Yes | No |
| Thomas | USA | Mixed | 28 | 14700 | 12 | NR | HMPS | Yes | No | No |
| Thomas | USA | NR | NR | 500 | 12 | PBMR | HMPS | Yes | No | No |
| Toribio-Vicente | Spain | Academic | 1 | 233 | 12 | EMR & PBMR | IHI-GTT | No | Yes | No |
| Unbeck | Sweden | Academic | 1 | 350 | 12 | EMR | IHI-GTT & HMPS | Yes | No | No |
| Val | Spain | Academic | 1 | 251 | 12 | EMR | IHI-GTT | No | Yes | Yes |
| Valencia-Martín | Spain | Mixed | 34 | 9975 | 1 | EMR | HMPS | Yes | No | No |
| Valkonen | Finland | Academic | 1 | 834 | 60 | EMR | IHI-GTT | No | Yes | No |
| Wilson et al (2012) [ | Egypt, Jordan, Kenya, Morocco, Tunisia, Sudan, South Africa, and Yemen | Mixed | 26 | 15548 | 12 | NR | HMPS | Yes | No | No |
| Wong | Canada | Academic | 1 | 141 | 4 | EMR & PBMR | IHI-GTT | No | Yes | Yes |
| Xu | China | Academic | 1 | 240 | 12 | EMR | IHI-GTT | No | Yes | Yes |
| Zadvinskis | USA | Academic | 1 | 317 | 1 | EMR | IHI-GTT | No | Yes | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPatient Safety and Medication Errors · Pharmacovigilance and Adverse Drug Reactions · Electronic Health Records Systems
Introduction
Adverse events in hospitalized patients constitute a significant public health problem in high-, middle-, and low-income countries [1, 2]. These events, which have been identified as one of the leading causes of death by the World Health Organization (WHO), are also the third most common cause of death in the USA [3]. The financial impact is substantial, with an average of 15% of public hospital budgets in high-income countries spent addressing adverse events [4]. The significant financial burden of adverse events in hospitalized patients within the Organisation for Economic Co-operation and Development (OECD) countries, where trillions of dollars are spent on their consequences, highlights the need for a reliable method to identify them [4].
Different methods used to identify adverse events in hospitalized patients include (i) retrospective medical record reviews, (ii) voluntary or mandatory incident reporting systems, (iii) patient safety and health quality indicators, and (iv) patient self-reporting post discharge [5–10]. The prevalence of adverse events can vary depending on which method is implemented [10]. When an adverse event is identified by one method, it may not be identified using a different method [5–10].
The retrospective medical records review method used to identify adverse events has been widely accepted as the ‘gold standard’ [11]. The Harvard Medical Practice Study (HMPS) and the Institute for Healthcare Improvement Global Trigger Tool (IHI-GTT) are two prominent examples that use this approach. The HMPS was published in 1991 by Brennan et al. as a feasible option to identify medical errors in hospitalized patients with predefined screening criteria [12]. The time-consuming nature of using the HMPS and the significant staff involvement for medical record reviews necessitated the development of a more efficient method. In 2003, the Institute for Healthcare Improvement developed the Global Trigger Tool as an alternate method, with an updated tool published in 2009 [13]. The IHI-GTT has been officially translated into the local language of several countries [14, 15], while others have adapted, modified, unified triggers according to the local settings, or used explicitly designed triggers for particular areas of interest [16, 17].
Use of a trigger tool involves a two-stage process. In the initial stage, a primary reviewer, typically a nurse, reviews medical records to identify triggers, clues, or predefined screening criteria that suggest the probability that the patient has experienced an adverse event [13]. This process aims to purposefully locate adverse events, followed by an in-depth assessment. Subsequently, in the second stage, a secondary reviewer, usually a physician, validates the presence of an adverse event by reviewing the medical records flagged with positive triggers, clues, or those meeting the screening criteria. This method, adaptable to paper-based, electronic, or hybrid medical records, has been successfully replicated across high-, middle-, and low-income countries and employed to identify the prevalence of adverse events in diverse hospital settings, including public teaching, non-teaching, and private organizations [18–22].
Previous systematic reviews have not addressed the predictive values of trigger tools [10, 11, 23–25]. The positive predictive value (PPV) indicates the probability that a patient has experienced an adverse event during hospitalization if a positive trigger is identified in their medical record. Probabilities are influenced by sensitivity, specificity, and prevalence values. The PPV for the IHI-GTT of 30.4% was reported in one systematic review involving eight studies [26]. The negative predictive value (NPV) of 99.0% was reported in one study [26]. The PPV for the HMPS (33.4%) was reported in a systematic review involving 12 studies [26], while no evidence of the NPV was found. This lack of information about the NPV constitutes an existing gap in the literature to be addressed [11]. Therefore, the aim of our systematic review was to provide a comprehensive description of the predictive value of trigger tools used to identify adverse events in hospitalized patients.
Methods
Design, search strategy, and data sources
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [27] and was registered in PROSPERO 1 January 2023 (CRD42023384335). Eligible studies were identified by searching CINAHL, Cochrane Library, EMBASE, and MEDLINE, CINAHL. The search was limited to peer-review research articles published in English or Spanish, between 2000 and October 2024, as one author is proficient in both languages. Reference lists of included articles were also screened. The complete search strategy is outlined in Supplementary File S1.
Eligibility criteria
Only primary research that reported the use of a trigger tool to identify the prevalence of adverse events was included. Research designs including cohort studies, case control studies, cross-sectional studies, and randomized controlled trials conducted in hospital settings in high-, middle-, and low-income countries were included. Articles comprising reviews, secondary research, posters, opinions, published conference abstracts, grey literature, outpatient departments, community settings, and studies conducted in patients younger than 18 were excluded.
Study selection
A search of four databases was conducted by one investigator, with all retrieved articles imported into EndNote^®^ 20. Following removal of duplicates, all references from the library were imported into Covidence^®^. Two independent reviewers screened article titles and abstracts to identify studies that included any information on trigger tools used to identify or measure adverse events in hospitalized patients according to inclusion criteria. The full text of all eligible articles was reviewed by the two independent reviewers. Any disagreement between the two reviewers was resolved by discussion, or by consulting a third reviewer until consensus was reached. The reference lists of included papers were reviewed to include any relevant articles not identified in the original search. One hundred articles were included in the systematic review (Fig. 1).
Systematic review flow diagram detailing the search results and the selection process
Data extraction
A standardized data extraction form was developed using Microsoft Word^®^ and Microsoft Excel^®^ based on information reported in each article (Supplementary File S2, Table 1). The relevant information extracted included: (i) author, year, and country; (ii) aim of the study; (iii) research design; (iv) setting; (v) sample size; (vi) inclusion and exclusion criteria, (vii) type of trigger tool, (viii) stages of the review process and staff involved, (ix) results, and (x) predictive values of the trigger tool.
Data synthesis
A narrative synthesis was undertaken through a structured process that involved organizing and summarizing the relevant studies characteristics [28]. The data were described based on relevant characteristics, such as differences in hospital setting, type of medical records, trigger tool used, number, background, and years of experience of the reviewers and predictive values reported. A meta-analysis of the predictive values across studies was not undertaken due to methodological heterogeneity. Findings were thoroughly examined to draw conclusions addressing the aim of the systematic review. The percentage reported in the results sections was calculated using Microsoft Office Excel 365.
Quality assessment
The risk of bias was assessed using the Joanna Briggs Institute (JBI) critical appraisal checklist for studies reporting prevalence data [29], which evaluates nine domains such as sample frame, sampling method, sample size, data collection, and statistical analysis. No modifications were made for this review. Two independent reviewers conducted the appraisal, resolving disagreements by consensus or consultation with a third reviewer; 11.0% (n = 11) of articles were double-checked, with 100% agreement (Supplementary File S3, Table 2).
Results
The systematic review included 100 articles, including 37 countries (Table 1); 86% of the studies were conducted in 21 high-income countries, 10.0% in seven upper-middle-income countries, 3.0% in three lower-middle-income countries, and 1.0% included eight countries: one upper-middle income, five lower-middle-income, and two low-income countries.
Of the 100 studies included in this systematic review, 66.0% did not report a predictive value, highlighting a significant gap in the literature; 16% of studies reported a predictive value for the trigger tool used in the study, 12.0% reported predictive values for individual triggers, and 6.0% reported predictive values for both the trigger tool and individual triggers used in the studies. Across these 34 studies reviewed, predictive values for individual triggers varied widely, ranging from 0 to 100%. Of these, only 23.5% reported a threshold of >20% for individual triggers, which was interpreted as indicators of medium to good trigger [16, 32, 58, 59, 84, 85, 114, 117]. Notably, only one study explicitly defined a PPV above >20% as an acceptable threshold for assessing the tool’s overall quality [60].
Among the 15 studies that reported the implementation of the HMPS, only 33.3% reported predictive values [42, 61, 62, 70, 86]; two studies reported a PPV of 53.6% [61] and 40.3%, respectively [70], while another reported a PPV of 37.9%, a NPV of 37.8%, a sensitivity of 73.9%, and specificity of 11.5% [62]. Additionally, one study reported a sensitivity of 89.0% for the tool [86], and another study involving two independent reviewers reported a sensitivity of 89.3% and 85.7%, respectively [42].
Of the 75 studies that reported the implementation of the IHI-GTT, 13.3% reported an average PPV of 54.5%, an average NPV of 80.9%, sensitivity of 86.6%, and specificity of 68.2%. The average tool predictive values were calculated by computing the arithmetic mean of values reported across studies that provided predictive values. The predictive values of the HMPS and IHI-GTT are presented in Table 2.
The hospital settings included academic (51.0%), non-academic (8.0%), private (1.0%), or a combination that was described as mixed hospitals (30.0%). In 10.0% of the studies, the type of hospital was not reported (Table 3).
Nine hundred and thirty-two hospitals were involved with 552 623 medical records retrospectively reviewed using a trigger tool in the studies retrieved. Although two studies did not mention the number of hospitals involved, the total number of medical records reviewed was reported [22, 71]. The medical records reviewed involved either electronic (42.0%), paper-based (6.0%), or a combination (hybrid) (10.0%). However, in 42.0% of the studies, the type of medical record review was not explicitly reported (Table 3). The study period for the medical record review varied widely between studies, ranging from one month [7, 85, 62, 113] to 72 months [53, 63, 87]. One study was conducted over a 1-week period [61], and in three studies [44, 79, 88], the period was not reported.
Of the included studies, 75.0% reported using the IHI-GTT, 15.0% used the HMPS, 3.0% used the IHI-GTT and HMPS [70, 44, 81], and 6.0% did not use either of the trigger tools mentioned [30, 58, 59, 71, 84, 89], and a subset of triggers from both the IHI-GTT and the HMPS [90] was used in 1.0%. Of the six studies that did not use either of the previously mentioned trigger tools, all involved the development of modifications or alternatives based on the IHI-GTT, comprising mental health triggers (n = 2) [58, 71], medication-related event triggers (n = 2) [30, 59], emergency department triggers (n = 1) [89], and oncology triggers (n = 1) [84].
All studies reported a collaborative two-stage review process. One study [70] reported an additional third stage for consensus in case of disagreement to validate an adverse event by secondary reviewers. A comprehensive review process was followed, involving two or more reviewers in 86.0% of the studies, with 8.0% not reporting the number of reviewers. Six studies only involved a single reviewer due to limited resources [22, 64, 65, 72, 82, 83]. In 60.0% of the studies, the review process involved at least one nurse and one physician, fostering a sense of inclusivity. The first stage was conducted with nurses as primary reviewers in 50.0% and physicians in the second stage as secondary reviewers in 40.0% of the studies. Other healthcare staff also participated in the first stage, including pharmacists, medical students, and residents, and in 7.0% of studies, the background of the members involved in the review team were not explicitly reported [7, 17, 64, 85, 91, 92, 66]. In most studies (72.0%), a physician validated the adverse events independently of the first reviewer. Seventy-eight per cent of the reviewers included internal staff where the study was conducted. Both internal and external reviewers were involved in 12.0% of the studies [20, 39, 61, 62, 73, 87, 113, 93–97], 4.0% involved external reviewers [21, 22, 88, 91], and 6.0% did not report this information [7, 19, 86, 30, 64, 47].
The time limit for reviewing medical records was reported in 46.0% of the studies with 80.4% reporting a 20-min time limit as supported by the IHI-GTT. However, a wide range was reported—from 15 min [80] when only the medication module of the IHI-GTT was implemented to 45 min when the full tool was used [73]. It is important to note that one study reported a time limit of 20 min for the first stage with the second stage requiring an additional 6 min using the IHI-GTT method [48]. One study reported the first stage of the HMPS required 30 min with the second stage completed in 32 min [19].
The prevalence of adverse events using the trigger tools varied widely from 1.1% when only one trigger was used (pressure ulcers) [74] to 83.0% when the original medication module trigger tool was used [82]. The prevalence of adverse events ranged from 7.2% [45] to 35.1% [98] when the original IHI-GTT tool was used, which was higher than the prevalence of adverse events reported when the original HMPS tool was used (range: 2.9% [21] to 28.0% [42]).
Quality assessment showed high methodological quality among the included studies, with domain-specific compliance rates as follows: appropriate sample frame (99%), appropriate sampling method (99%), adequate sample size (98%), detailed description of subjects and setting (97%), adequate coverage in data analysis (100%), valid identification methods (100%), standardized and reliable measurement (100%), and appropriate statistical analysis (99%). The response rate was not applicable in this study. Overall, the risk of bias was low.
Discussion
Statement of principal findings
This systematic review has highlighted key findings. The IHI-GTT and the HMPS are the most frequently cited trigger tools in the literature for retrospective medical record reviews. Despite the widespread use of trigger tools to identify the prevalence of adverse events in hospitalized patients in high-, middle-, and low-income countries, the predictive values of the tool are only reported in about one in seven studies.
Significant differences in the predictive values and prevalence of adverse events between the IHI-GTT and the HMPS have been identified in the systematic review. The prevalence of adverse events identified with the trigger tools was higher when the IHI-GTT was implemented compared with the HMPS. This can be explained as the IHI-GTT includes three times the number of triggers (53 vs 18 triggers) and is divided into six modules. On the one hand, the modular integration of the IHI-GTT allows the users to use the entire tool, selected modules, or selected triggers. On the other hand, limited studies reported using the full IHI-GTT [6, 7, 34, 45, 87, 91, 96, 98–100, 105, 113, 114]. This explains why the HMPS, which has fewer triggers, had better predictive values reported in a previous systematic review [26] but a lower prevalence of adverse events than the IHI-GTT. In addition, it is evident from this systematic review that the IHI-GTT has been translated into languages other than English [53, 55], constituting an asset of the method that can be easily implemented in different countries and local hospital settings.
In recent years, modifications or alternatives to the original IHI-GTT have been developed. These include automated detection systems using electronic health records, natural language processing, and machine learning algorithms, which aim to identify adverse events with greater efficiency and accuracy while reducing the time required from clinical staff to review medical records [17, 48, 79, 90]. Moreover, adapted versions of the IHI-GTT have been tailored to specific contexts, including mental health [58, 71], medication-related events [30, 59], emergency care [89], and oncology [84]. Recognizing these innovations highlights both the ongoing relevance and the limitations of the original IHI-GTT. However, despite the proliferation of these approaches, evidence regarding their validity and predictive performance, particularly their predictive values remains limited.
The predominance of the IHI-GTT and HMPS in the literature likely reflects the established validation, broad applicability, and the availability of training resources [13], which facilitate the use of these tools to identify adverse events with retrospective medical records review to improve patient safety. In contrast, newer or modified trigger tools may have limited uptake due to a narrower clinical scope, the need for local adaptation, and limited published evidence on the validity and reliability of these tools [30, 84, 58, 59, 81, 89]. Further research should examine the comparative performance of these emerging tools and the potential to enhance adverse event detection in specialized settings.
The retrospective medical records review has been widely standardized as a two-stage process for both the IHI-GTT and the HMPS. This approach is generally standardized to reduce physicians’ time, as only one study reported a single physician conducting both stages [65]. The first stage was not always conducted by two experienced nurses, and the validation in the second stage did not involve a physician, as recommended by the IHI-GTT instructions and methods section [13]. However, other staff such as pharmacists and respiratory therapists also participated in the first stage. Although the IHI-GTT studies did not adhere to the planned methods or staff involvement, reliable results were obtained. This is important because this systematic review provides strong evidence that the IHI-GTT is a feasible and user-friendly tool, producing reliable outcomes when used by various healthcare professionals.
The total number of reviewers and teams involved in the medical records review could be a significant factor that influences the medical record review process. The minimum of three participants recommended by the IHI-GTT was not adhered to in all of the studies reviewed. When only one pharmacist was involved in the review of the medication trigger tool, a prevalence of 83% for adverse drugs events was reported [82]. In Spain, when only one physician [65] conducted both stages, an adverse events prevalence of 35.4% was reported, highlighting that the full review process can be conducted involving one physician with reliable outcomes. The two studies where one physician conducted both stages reported an average adverse event of 16.3% (range 12.8% to 19.0%) with the HMPS [22] and 35.4% with the IHI-GTT [65]. This could be explained as more consistency or less heterogeneity criteria exist when the review team is limited. However, the time involved could be time-consuming when only one reviewer is involved.
The experience of the reviewers in both stages were not reported in 64.0% (n = 64) of the studies. In 36% of the studies (n = 36), the experienced of the reviewers involved in the process ranged from no experience to more than 30 years of experience [5, 58, 49, 75]. The most frequent reported included nurses with more than 5 years of experiences and physicians with more than 10 years of experience [16, 19, 34, 44, 56, 58, 67, 79, 96, 107]. This is important because the evidence suggests that an experienced reviewer needs to be involved in the process.
Strengths and limitations
This systematic review had several strengths. First, this review adhered to the PRISMA statement and followed the registered study protocol in PROSPERO. Second, the search strategy included studies from 37 countries. Third, this is the first systematic review to include predictive values of the IHI-GTT and HMPS trigger tools used to identify the prevalence of adverse events in hospitalized patients, offering a fresh perspective on patient safety. Hence, the outcomes presented are generalizable.
We identified the following limitations. First, only articles published in English and Spanish were included; articles published in another language may have been excluded. Second, despite the strong search strategy and manual review of citations, some articles may not have been included. Third, a meta-analysis was not conducted because despite the prevalence of adverse events reported in almost all the studies, no reported data or inconsistent reporting formats were identified, therefore a narrative synthesis was conducted. Fourth, heterogeneity across studies was identified, with some studies conducting a retrospective record review using specific triggers or modules, thereby limiting the ability to synthesize findings meaningfully.
Interpretation within the context of the wider literature
The two trigger tools reported in the literature to measure the prevalence of adverse events in hospital settings included the HMPS and the IHI-GTT methods. However, the IHI-GTT has several advantages over the HMPS, as presented in this systematic review. First, the original IHI-GTT can be used (including full number of triggers and modules) or only specific triggers or modules [13]. The tool can be translated into official languages or used in its original language [53, 55]. The two-stage retrospective medical review can be conducted by a single experienced and trained healthcare professional, such as a nurse, physician, pharmacist, or other healthcare providers, which is an asset of the IHI-GTT, as it enhances both the reliability and feasibility of the tool [83, 65, 72]. Both methods have been reproduced and implemented in different countries, with varying outcomes regarding the prevalence of adverse events. However, a higher prevalence of adverse events was identified when using the IHI-GTT, which included electronic, paper-based, or hybrid medical records [16, 75, 76, 107, 109].
Implications for policy, practice, and research
The findings in this systematic review are of significant value for future policy and practice in identifying the prevalence of adverse events across different hospital settings worldwide. The use of a trigger tool to determine the prevalence of adverse events offers a structured approach to improving healthcare outcomes. Currently, the IHI-GTT presents an accessible and feasible option for implementation in hospital settings without requiring substantial economic investment, making it particularly advantageous in resource-limited environments [13]. In future practice and research, the development of digital trigger tools has the potential to reduce the time spent identifying triggers in hospitals equipped with electronic medical records [17, 48, 79]. However, this approach necessitates the supervision of healthcare professionals to validate the findings effectively [85, 87]. Despite advances in digital tools, retrospective medical records reviews will continue to be critical. Moreover, the validation of adverse events will remain dependent on the expertise of physicians or other experienced healthcare professionals [50, 87, 90].
To enhance healthcare process and hospital outcomes globally, recommendations include the implementation of the IHI-GTT in projects aiming to identify the prevalence of adverse events. This approach is recommended across all countries, regardless of their income levels or type of medical records utilized, ensuring a standardized and effective methodology for improving patient safety and healthcare quality.
Conclusions
The predictive values of trigger tools described in this systematic review provide evidence supporting the IHI-GTT as an appropriate tool for identifying the prevalence of adverse events in hospitalized patients. The IHI-GTT can be used in different countries and hospital settings, and its feasibility and reliability ensure high reliability of the outcomes.
Supplementary Material
mzaf119_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Conceptual Framework for the International Classification for Patient Safety. Version 1.1: Final Technical Report January 2009. Geneva: World Health Organization, 2010. Contract No. WHO/IER/PSP/2010.2.
- 2World Health Organization. Patient Safety, Global Action on Patient Safety, Report by the Director-General. World Health Organization; 2018. Report No. EB 144/29.
- 3Makary MA , Daniel M. Medical error—the third leading cause of death in the US. BMJ 2016;353:i 2139. DOI: 10.1136/bmj.i 213927143499 · doi ↗ · pubmed ↗
- 4Slawomirski L , Auraaen A, Klazinga NS. The economics of patient safety: strengthening a value-based approach to reducing patient harm at national level. Paris: OECD 2017.
- 5Mull HJ , Brennan CW, Folkes T et al Identifying previously undetected harm: piloting the institute for healthcare improvement’s global trigger tool in the Veterans Health Administration. Qual Manag Health Care 2015;24:140–6.26115062 10.1097/QMH.0000000000000060 PMC 4570496 · doi ↗ · pubmed ↗
- 6Kurutkan MN , Usta E, Orhan F et al Application of the IHI global trigger tool in measuring the adverse event rate in a Turkish healthcare setting. Int J Risk Saf Med 2015;27:11–21.25766063 10.3233/JRS-150639 · doi ↗ · pubmed ↗
- 7Classen DC , Resar R, Griffin F et al ‘Global trigger tool’ shows that adverse events in hospitals may be ten times greater than previously measured. Health Aff (Millwood) 2011;30:581–9.21471476 10.1377/hlthaff.2011.0190 · doi ↗ · pubmed ↗
- 8Samal L , Khasnabish S, Foskett C et al Comparison of a voluntary safety reporting system to a global trigger tool for identifying adverse events in an oncology population. J Patient Saf 2022;18:611–6.35858480 10.1097/PTS.0000000000001050 PMC 9391281 · doi ↗ · pubmed ↗