Digital-based physical activity interventions implemented across the League of Arab States: a scoping review
Elizabeth Dodge, James Barry, Fatmah Almoayad, Samiah Alqabbani, Afrah Almuwais, Joanna Kruk, Basil H Aboul-Enein

TL;DR
This review explores how digital tools for physical activity are used in Arab countries to improve health, finding some success but limited long-term impact.
Contribution
The study provides a scoping review of digital physical activity interventions in the League of Arab States, highlighting their effectiveness and limitations.
Findings
Blended digital and educational strategies increased physical activity levels and improved health outcomes.
Interventions showed limited long-term effectiveness and geographical coverage.
Digital tools offer potential for health promotion in Arab countries despite cultural and access challenges.
Abstract
This scoping review investigates the use and impact of digital-based physical activity (PA) interventions in Arabic-speaking countries. These technologies have dramatically transformed healthcare management and offer a valuable tool for managing non-communicable diseases. Despite challenges such as limited healthcare access and cultural norms, these tools enable health promotion, preventive care, and personalized health plans. The aim of this scoping review is to evaluate the effectiveness of digital-based PA interventions, such as mobile apps, used across the League of Arab States. PRISMA-ScR guidelines were applied to conduct this scoping review across 10 databases using pertinent search terms for relevant studies published between 2010 and December 2024 to identify publications conducted across Arab countries. Sixteen studies on digital-based PA interventions in four Arab countries…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
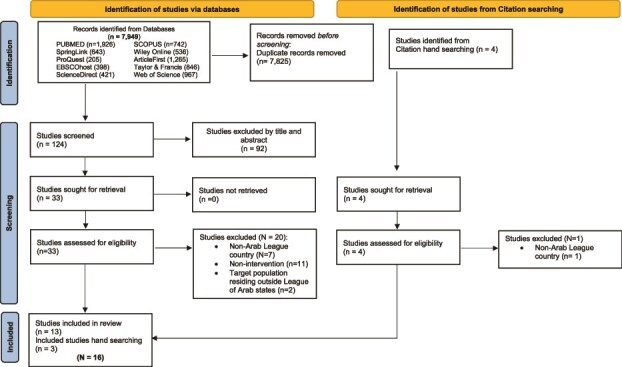 Figure 1
Figure 1| Databases | Search Period | keywords, search terms, and phrases |
|---|---|---|
| Scopus, PubMed, SpringerLink, Wiley Online, ProQuest, ArticleFirst, EBSCOhost, Taylor & Francis, Web of Science, and ScienceDirect | 2010 and December 31st, 2024 | ‘online’ [All Fields]; OR ‘app’ [All Fields]; OR ‘digital’ [All Fields]; OR ‘computer’ [All Fields]; OR ‘technology’ [All Fields] OR ‘internet’ [All Fields] OR ‘web-based’ [All Fields] OR ‘social media’ [All Fields] OR ‘eHealth’ [All Fields] OR ‘mHealth’ [All Fields] OR ‘smartphone’ [All Fields] |
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population |
Arabic speaking populations that reside in an Arab League member state |
Non-Arab or Arabic speaking populations Arab diaspora residing outside an Arab League member state. |
| Intervention type | Any kind of digital based physical activity (PA) intervention that address PA-related outcomes, including: Digital Applications of PA Digital Tools in enhance PA Educational interventions. Environmental Interventions. |
Non-digital based Interventions Interventions that do not address PA-related outcomes. |
| Comparators | Pre-intervention, baseline physical activity-related variables (i.e. anthropometric measures, PA-related knowledge, self-reported scales related to PA) of groups who were: Control: received no intervention. Received partial intervention (e.g. educational intervention only vs. multi-componential intervention.) | N/A |
| Outcomes of interest |
Changes in anthropometric outcomes, e.g.: BMI, WC, weight Changes in self-reported scales related to PA outcomes. Changes in PA-related knowledge. Changes in meeting the PA daily recommendations. Changes in adherence to PA. |
Non-PA related outcomes |
| Language | English, Arabic, French | All other languages |
| Study Type |
Experimental intervention studies with quantitative outcomes. Peer-reviewed original research articles Original research conference publications |
Non-numeric/categorical assessments or qualitative studies Non-Peer-reviewed articles Study protocols Narratives Similar article types Grey literature Communications Non-intervention based studies White papers |
|
| Country | Target Population | Type of Study | Sample Size | Intervention | Details of PA Intervention | Duration of Intervention | Theoretical Framework/ | Measured Parameters related to PA | Main Results | Main Recommendations |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| Gmmash et al. (2023). | Saudi Arabia | Adolescents (10–18 yo) | Pre- and post-experimental study | 27 participants | Phone Calls | As part of the intervention group participants received a motivational phone call from a trained physical therapist. | 8 weeks | Self-Determination Theory | Physical Activity Level | Participants had significant improvement on a PA scale ( | Significant improvements were detected in both groups after the virtual eight-week program. Preliminary data suggest that providing a virtual physical education program can improve adolescents’ physical health. |
|
| |||||||||||
| Shaban et al., (2024). | Egypt | Adults with type II diabetes, over 50 | Quasi-experimental pretest-post-posttest design | 120 | Mobile app | The intervention group received access to the app, which provided personalized content on multiple factors, including PA. The control group received SOC and face-to-face counseling, with print educational materials | 4 months | Social Cognitive Theory, Self-efficacy | Summary of Diabetes Self-Care Activities (SDSCA), specifically the exercise section | The post- intervention group score on the exercise portion of the SDSCA statistically significantly increased ( | This study demonstrates the possibility of a digital-based nursing intervention to improve self-care behaviors in adults with Type II Diabetes Mellitus, including increasing exercise |
| Basuodan et al. (2023). | Saudi Arabia | Female Junior College students aged 19 (+/−0.9) years | Pre-posttest design | 46 | Virtual Introductory (zoom) class | 6-week course where students received daily online PA promotive messages via the WhatsApp smartphone application. One message every working day (5x/week) | 6 weeks | Social Cognitive Theory, Self-efficacy | physical activity IPAQ-Long form, and IPAQ-short form | Significant increase in the proportion of students who perform walking ( | The program is effective in increasing college students PA in specific domains such as walking for transportation and engaging in moderate PA for leisure, but not in |
| Alshahrani et al. (2021). | Saudi Arabia | Female College Students Age 18–28 | Pretest/posttest Randomized controlled open label experimental design | 110 | Using WhatsApp, the intervention group received a 15-minute orientation and 3 to 4 health-promotional/physical activity messages per week. | 10 weeks | Health Belief Model of Behavior Change | Baseline physical activity between control and intervention group | Significant difference was observed in the intervention group pre and post in all domains (work-related, ( | Technological advancements can be used as a tool for health promotion. | |
| Ismail et al. (2022). | Qatar | Employees in Qatar who spend most of the working day sedentary. | Mixed Methods | 58 participants | Mobile App | Two apps were used MotiFitLite which sent a static message to the control group | 66 days | Health Belief Model of Behavior Change | Physical Activity time | Neither group showed a significant monotonic trend in daily active time. | The Motifit lite encouraged users to take a break but did not show a significant difference in PA. A larger sample size could potentially show stronger results. |
| Alasfour, & Almarwani (2022). | Saudi Arabia | Women aged >50 with knee osteoarthritis (OA) | Two-arm | 40 | Smartphone App | ‘My Dear Knee’ is an Arabic Smartphone Application | 6 weeks | n/a | Self-reported exercise adherence | My Dear knee intervention group had statistically significantly higher adherence to exercise ( | The positive results on adherence rate suggest that this simple intervention is potentially effective. |
| Ali et al. (2021). | United Arab Emirates | Women with overweight or obesity | Non-randomized, two-arm feasibility study | 161 | Self-Monitoring Fitness App | Rashakaty website | 16 Weeks | Social Cognitive Theory | Physical Activity Levels | Compared to the basic intervention arm, the enhanced intervention arm demonstrated significant increases in minutes of vigorous PA ( | Use of language on website and educational materials should be more inclusive and culturally tailored. Mobile-and technology based education delivery can improve PA, and associated anthropometrics. |
| Alnasser et al. (2019). | Saudi Arabia | Women with overweight or obesity | Pre-test/post-test single arm | 240 | Phone App | Evidence Informed Mobile Health app (Twazon Arabic weight loss app) | 4 months | Health Belief Model of Behavior Change | Physical Activity | Limited differences were noted between engaged and unengaged app users; WC decreased significantly ( | Positive outcomes were seen but the limited sample size did not allow for any concrete conclusions. |
|
| |||||||||||
| Hasan et al. (2018). | United Arab Emirates | Adult females | Quasi-experimental pretest-posttest | 52 | Pedometer | Each participant was given a digital pedometer to wear and a physical activity logbook. Weekly follow-up was conducted to ensure progress. | 9 weeks | Lifestyle modification based educational material | PA Step Count | There was a noticeable but not significant increase in steps. | The findings suggest that participants in both the low active and high active lifestyle groups benefited from counting steps using a pedometer. |
|
| |||||||||||
| Saquib et al. (2023). | Saudi Arabia | Female | 2 * 2 randomized trial design | 181 | WhatsApp | Participants in the intervention group used a WhatsApp group chat, received two to three health promotional WhatsApp messages, and given pedometers for step count. Control group receives similar number of WhatsApp non-health related messages and no pedometer. | 12-Week | Social Cognitive Theory | Pedometer Step Count | There was no significant difference between group step counts; however, the intervention group had a significant group-by-time change in average daily step count ( | Delivering a PA intervention to university students through WhatsApp is a feasible and potentially effective way to increase daily steps |
| Al-Kuwari et al. (2017). | Qatar | Adults in Qatar | Longitudinal Intervention | 268 | Pedometer | Pedometer and an online self-monitoring online account | 1 year | Social Cognitive Theory | Physical Activity (Steps per Day) | Significant increase in steps per day ( | Pedometer based intervention has long term effects on increasing physical activity levels |
| Al-Ghafri et al. (2021). | Oman | Adults aged 18–60 with type 2 diabetes and no contraindications to Physical Activity | Quasi-experimental pretest-posttest | 174 | WhatsApp | Each member in the intervention group received a PA consultation, Pedometer, and standardized messages using WhatsApp Messenger App | 12 months | Health Belief Model, Stages of Change, and Social Cognitive Theory | Physical Activity using 13-item Global Physical Activity Questionnaire (self-efficacy SE, social support SS) and expressed as MET equivalent | The intervention group scored higher in self-efficacy in engaging with PA ( | The MOVEdiabetes intervention for physical activity was associated with positive changes in self-efficacy related PA. |
| Al-Mohannadi et al. (2019). | Qatar | Health Care Workers in Qatar | Two Cross Sectional Surveys, pre-post intervention | 212 | Pedometers | Step into Health Participants received a pedometer that uploads to an online platform | 3 months | Social Cognitive Theory | Step Count | Average step count was significantly increased from pre-post intervention ( | Step Into Health workplace interventions showed an increase in PA, but those numbers decreased after the intervention period. |
| Al-Kuwari et al. (2016). | Qatar | Adults | Cross-sectional longitudinal study | 970 Adults | Pedometer Email | Email reminders when participants did not upload data for 14, 21, and 28 days | 12 weeks | Social Cognitive Theory | Step count | There was a significant increase in daily step count at 12-weeks ( | Pedometer programs combined with email and text reminders can be used to promote physical activity among middle-aged adults and elderly to prevent non-communicable diseases associated with sedentary lifestyles |
| Al-Kuwari & Al-Hamdani (2021). | Qatar | Male participants | Retrospective study | 1127 Participants | Pedometer and mobile app | 518 used pedometer and 609 used a smartphone app | 12 weeks | Social Cognitive Theory | Step Count | Both groups showed significant changes from pre-post intervention. The pedometer group significantly increased their daily steps ( | The findings suggest that the use of the Step Into Health program when combined with either a programmed digital pedometer, or the use of a smartphone pedometer app can significantly increase PA. |
| Salih Khidir et al. (2021). | Qatar | University Staff and Students ages 18–64 | Experimental pretest-posttest design | N = 397 | Pedometers or mobile app | All participants were invited to take part in a 4-month walking competition between participating campuses. | 5-months phase 1- and 5-months phase 2 | Social Cognitive Theory | Step Counts | Significant increase in step uploads during phase 1 where participants received reminders, however there was not a significant increase in steps in either phase. | The study showed a mix of walking competitions, and use of mobile technology to evaluate step counts did not statistically significantly increase steps, however, the reminders to upload daily step activity were effective. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhysical Activity and Health · Mobile Health and mHealth Applications · Cardiovascular and exercise physiology
INTRODUCTION
Digital-based interventions for non-communicable disease
Non-communicable diseases (NCDs), including cardiovascular disease (CVD), type II diabetes mellitus, cancer, and musculoskeletal disorders, are the leading causes globally, of morbidity and mortality [1–3]. According to the World Health Organization, over 41 million people die each year from NCDs, accounting for roughly 74% of all deaths worldwide [4]. The burden is disproportionately borne by people of lower socioeconomic status, those without access to consistent healthcare, and minority populations in countries with advanced economies [5–9], while also having a disproportionate impact on low-and middle-income-countries (LMIC’s) [3, 5, 10]. Across the Organization for Economic Cooperation and Development countries, low socio-economic status is consistently and significantly associated with NCD related morbidity and mortality [8]. Digital-based and digitally delivered interventions can provide low-cost, easily accessible interventions that target behavior change related to non-communicable diseases, and have been shown to be effective at promoting positive health behaviors to help prevent or manage NCD’s [11–13]. Interventions target a range of behaviors associated with NCD’s, including, but not limited to, mental well-being, smoking cessation, adoption of healthy eating behaviors, and increasing physical activity (PA) [14–17].
Digital-based PA interventions
One of the key benefits of digital- and app-based interventions is their ability to empower individuals to take control of their health and wellness [18]. These technologies promote health lifestyles by providing users with real-time feedback on their health metrics, such as PA, heart rate, sleep patterns, and more, enabling them to make informed decisions about their lifestyle and healthcare management [19]. Digital-based interventions specifically focused on increasing PA have been shown to be effective to varying degrees when supplied by various digital and mobile delivery modalities (email, text message, zoom, WhatsApp) as well as across varied populations; the evidence shows a consistent positive, yet sometimes weak association between digitally delivered interventions and their outcomes [20–24].
Digital-based interventions in the Arab States
One of the most prominent health challenges in Arabic-speaking countries is the increasing prevalence of non-communicable diseases (NCDs) such as cardiovascular diseases, diabetes, and obesity. Risk factors for NCDs, such as unhealthy diet, physical inactivity, and sedentary lifestyles, are prevalent in the region, contributing to the increasing burden of NCDs. Lifestyle changes associated with urbanization and economic development have also contributed to the rising prevalence of NCDs in Arabic-speaking countries [25–29]. A recent review found that digital health interventions in fragile states in the Middle East and North Africa can provide solutions to help address health needs in areas of geopolitical instability [30]. A digital health intervention designed to help displaced persons with depression and/or anxiety found clinically relevant improvements in participants that had consistent digital access’ noting that the success of such interventions is limited by access to electricity and technology with which to engage with them [31]. A review by Al Dweik et al [32] found that digital-based mental health interventions implemented in the United Arab Emirates were feasible, accessible, flexible, and often improved clinical outcomes; however challenges such as participant level of digital literacy, access to technology, reading ability, and concerns that digital modality could totally replace (to the detriment of the client) face-to-face or physical interactions with their mental health professionals [32]. The League of Arab States includes both low-and middle-income countries, as well as those that have more advanced economies; while this review predominantly includes studies that are not conducted in LMIC’s, there are shared cultural norms, health beliefs, and similar social and political structures to navigate in the provision of public health interventions. Therefore, it is critical to examine potential challenges and barriers to the delivery of digital-based health interventions in the Arab States, while also identifying commonalities in successful digital-based interventions that can be applied to increase efficacy of such interventions.
Digital-based PA interventions in the Arab States
The use of mobile health app technology has been used to encourage the population in Arabic-speaking countries to follow PA guidelines which is essential for improving overall health and well-being. Implementing health promotion interventions, programs, and campaigns targeting different communities, such as schools, workspaces, and public places, can be effective in promoting and maintaining PA [33–38]. Mobile health promotion interventions focused on developing strategies that foster individual motivation to start walking regularly and maintain their commitment to the activity. Identifying and addressing barriers to walking, such as time constraints, lack of motivation, or safety concerns, can contribute to enhancing individual commitment to walking as a regular PA [39–43]. Culturally relevant educational campaigns that integrate the health benefits of exercise into familiar cultural narratives can increase intervention adherence and efficacy, including culturally tailored interventions, community-based initiatives offering gender-specific exercise classes, walking groups, or fitness events within culturally safe environments. Addressing these challenges is critical to fostering equitable opportunities for PA [44].
The advent of wearable and digital health technology and the use of health apps on mobile phones have revolutionized the way individuals manage their health and wellness, gaining popularity worldwide, including in Arabic-speaking countries, and are transforming the landscape of healthcare management [45]. Advancements in digital-based technology have enabled the integration of digital devices, mobile applications, and communication tools, such as activity monitors and digital mobile applications, to influence behavior positively and encourage the adoption of a healthier lifestyle [46]. In Arabic-speaking countries, where access to healthcare services may be limited in certain areas or for certain populations, wearable health technology and health apps can bridge the gap by allowing remote monitoring of patients’ health metrics. Another significant advantage of wearable health technology and mobile technology health apps is their potential to enhance remote monitoring and telehealth, patients can wear monitoring devices that record vital information that can get uploaded remotely to healthcare providers [43].
The state of health in Arabic-speaking countries is shaped by a range of factors, encompassing social, economic, environmental, and cultural determinants of health [44, 47, 48]. According to the World Health Organization Eastern Mediterranean Regional Office, the rate of non-communicable diseases associated with obesity-related comorbidities such as diabetes and heart disease is rapidly rising in this region [25, 44, 49–51]. Therefore, this scoping review aims to evaluate the effectiveness of digital-based PA interventions, such as mobile apps, used within the League of Arab States. This information is essential for suggesting culturally and socially appropriate health promotion strategies that address sedentary lifestyle behaviors in Arabic-speaking communities.
METHODS
The scoping review was performed in accordance with the PRISMA extension for scoping reviews and Arksey and O’Malley’s framework [52, 53]. The search was conducted in the winter of 2024 and the results communicate literature published between 2010 and December 2024. For the purpose of this review, Arabic-speaking countries are defined as the 22 member countries of the Arab League States [54, 55]. Ten academic electronic databases were used for the literature search: Scopus, PubMed, SpringerLink, Wiley Online, ProQuest, ArticleFirst, EBSCOhost, Taylor & Francis, Web of Science, and ScienceDirect. These databases were selected due to their medical and biomedical scope. The following combination of search terms, keywords, and phrases were used: ‘Online’; ‘app’; ‘digital’; ‘computer’; ‘technology’; ‘internet’; ‘web-based’; ‘social media’; ‘eHealth’; ‘mHealth’; ‘smartphone’; AND ‘Physical Activity’; ‘Exercise’; ‘Intervention’; ‘Program’ AND ‘Algeria’; ‘Egypt’; ‘Bahrain’; ‘Comoros’; ‘Djibouti’; ‘Iraq’; ‘Jordan’; ‘Saudi Arabia’; ‘Kuwait’; ‘Lebanon’; ‘Libya’; ‘Mauritania’; ‘Morocco’; ‘Oman’; ‘Occupied Palestinian Territories’; ‘Qatar’; ‘Yemen’; ‘Somalia’; ‘Sudan’; ‘Syria’; ‘Tunisia’; ‘the United Arab Emirates’ (See supplemental material file and Table 1).
The search strategy was customized to fit the indexing systems of each respective database. All retrieved articles were screened for their relevance to the topic. Additionally, reference lists of included studies were examined for further relevant studies (see Fig. 1). Titles and abstracts were assessed for relevance, and pertinent journal abstracts were reviewed by three authors (J.K., E.D., and B.A-E.). One author (B.A-E) utilized Rayyan QCRI software to aid in the screening process [56]. Potential disagreements between reviewers were resolved by consensus. Potential studies for inclusion were independently evaluated based on relevance, merit, and eligibility criteria for inclusion and exclusion (see Table 2). Final decisions regarding inclusion and the documentation of exclusion reasons were made collectively by all authors. Figure 1 illustrates the elimination process leading to the selection of articles for this review. The data extracted from the studies included in the review include author, year of publication, country of intervention, the target population, sample size, intervention type, details of the intervention as related to digital-based delivery of an intervention measuring PA and related anthropometrics as outcomes, the intervention duration, the theoretical framework or model used in intervention development, the outcome measures, main findings, and main recommendations. The characteristics of the data extracted from the included studies are summarized in Table 3. Methodological quality assessment is not a requirement for scoping reviews, included studies were not evaluated for quality [57]. No ethical oversight was found to be necessary for this review and, therefore, no institutional review board was acquired.
PRISMA 2020 flow diagram
RESULTS
This review included 16 studies that were conducted between 2016 to 2024, in five Arabic-speaking countries. Six studies were conducted in Saudi Arabia [58–63]. Six studies were also conducted in Qatar [64–69]. Two studies were conducted in The United Arab Emirates [70, 71] and a single study was conducted in each Oman [72] and Egypt [73]. The research designs employed in these studies were diverse, and included retrospective [57], cross-sectional [56, 58], randomized controlled trials [47, 49], and pre-post experimental designs [48, 50, 51, 59, 62, 63], among others described in Table 3.
The studies included in this review spanned a wide range of sample sizes, and included a total of 4183 participants. The largest sample size was in the retrospective study conducted by Al-Kuwari & Al-Hamdani [66] and included 1127 participants while the smallest sample size was 27 participants in a pre-post–test experimental pilot study [62]. The duration of the included interventions ranged from 6 weeks [58, 61], and 1 year [69, 72], with a mean intervention duration of 16.77 weeks. The participant age also ranged greatly, from Adolescents 10–18 [62] to adults aged 64 [68], indicating that digitally delivered interventions use may be an effective tool to engage with a variety of ages.
Of the 16 studies included in this review, 15 explicitly incorporated a theoretical framework or model into their methodologies. The Self-Determination Theory was applied in the study by Gmmash et al [62]. The most commonly employed theoretical basis for the interventions was the Social Cognitive Theory (SCT) which was utilized in 10 interventions [61, 63, 65–70, 72, 73], with Basuodan et al [61], and Shaban et al [73] both using SCT and emphasizing the construct of self-efficacy [50] and Al-Ghafri et al [72] using SCT in combination with the Health Belief and Stages of Change models [63] . Other interventions relied on the Health Belief Model of Behavior Change [59, 60, 64], or Lifestyle Modification [71] as the framework to elicit behavior change. Only one included study by Alasfour & Almarwani [58] did not explicitly note a theoretical framework or model that the intervention was based upon; the ‘My Dear Knee’ app was designed to help women with knee osteoarthritis complete PT exercises.
The 16 studies included in this review employed a diverse range of interventions, leveraging various digital tools and strategies. The majority of the interventions included utilized an app to deliver the intervention that relied solely on an app for delivery [58–61, 64, 70, 73], while others [63, 65–69, 72] used a multi-modality approach that combined apps, emails, and/or text messaging with pedometers. Hasan et al [71] used just a digitally programmed pedometer and a PA logbook to track their steps in. Finally, Gmmash et al [62] utilized zoom to train participants on PA, followed by weekly phone calls from a trained physical therapist. The parameters of interest extracted from each study were the outcome measures related to PA, as well as related anthropometric changes.
The majority of the studies reported a significant impact of the digitally delivered intervention on PA, or related anthropometrics. Five studies utilizing a PA scale to measure activity saw statistically significant increases in PA score [61, 62, 65, 72, 73] in the intervention groups, while Saquib et al [63] reported no between group differences, however, they did find a group-by-time change (P = 0*.*4) in the intervention groups daily step count.
In studies that reported PA as step count, there were mixed findings. Hasan et al [71] found a noticeable but non-significant increase in steps, however interestingly, they did find statistically significant improvements (significance was set at P < 0*.5) across all anthropometric measures with the exception of fat-free-mass; these included improvements in BMI, Body fat mass, waist:hip ratio, waist circumference, and visceral fat area. These findings indicate that even a nominal increase in steps can have positive and significant impacts on indices of obesity. However, three studies [65, 67, 69] demonstrated that their digital-based intervention significantly increased step count in the intervention group (P < 0.05, P = 0.48, P = 0.01, respectively), while one study [66] found that both their pedometer group and their smartphone app group significantly increased their step count from pre-post intervention (P = 0.01, and P < 0.05, respectively), there was no significant difference between groups (P = 0.61), indicating that the intervention + either a digital pedometer or a smartphone app to track steps can contribute to increased step counts. Salih Khidir et al [68], did not find any increase in steps between phases of the intervention, however they did note that in phase one when there were participant reminders to log their steps that there was a significant increase in the uploading of steps data, indicating that incorporation of periodic reminders or ‘nudges’ to participants can increase adherence to intervention protocol. Ali et al [70] found statistically significant increases in minutes of vigorous PA (P = 0.25), days of moderate PA (P < 0.001), minutes of moderate PA (P < 0.001), and walking (P < 0.001), as well as a significant decrease in sitting time (P < 0.001) in the enhanced intervention group compared to the basic intervention group. Alshahrani et al [60] reported significant findings in time spent in PA from pre-post in the intervention group across all domains, including time spent in PA at work, related to transportation (i.e. walking, rather than driving, parking further away from your destination), recreational PA and total PA. Also reporting on time spent in PA, Ismail et al [64] found no significant difference between the intervention and control groups in overall activity, however, the intervention group did have significantly increased PA at work. One study [58] investigated self-reported exercise adherence in the ‘My Dear Knee’ app; which found that the intervention group reported significantly higher (P = 0.02) adherence to exercise compared to the control group. Anthropometrics related to PA also exhibited change in the enhanced intervention arm compared to the basic, with significant decreases in WC (P < 0.001), BMI (P < 0.042), % body fat, (P < 0.001), amount boy fat (P < 0.001), with a decrease in fat-free mass (P = 0.*43) compared to the basic intervention group [70].
DISCUSSION
This scoping review identified 16 studies conducted between 2016 and 2024 that evaluated the impact of digitally delivered PA interventions across five Arabic-speaking countries. The majority of the included studies demonstrated that digital interventions, whether app-based, multi-modal, delivered via phone or complimented using pedometers, were effective in increasing PA levels and improving related anthropometric outcomes. Notably, five studies [61, 62, 65, 72, 73] that measured PA using validated scales reported statistically significant improvements; these five studies all utilized a theoretical framework to inform the development and delivery of the intervention materials, and include Self-Determination Theory [62], Social Cognitive Theory (SCT) with Constructs of Self-Efficacy [61, 73], Health Belief Change combined with Stages of Change and SCT [72], and Social Cognitive theory [65]. While connected but distinct concepts, each of these interventions conceptual frameworks utilized the construct of self-efficacy to effect behavior change.
The findings indicate that digitally delivered interventions can be powerful tools for addressing sedentary behaviors and associated non-communicable diseases (NCDs) in Arabic-speaking populations, and build upon recent literature noting that purposeful use of social media/digital interventions, especially when culturally tailored, can effect behavior change in this population [73–77]. These findings align with the success of digitally delivered public health interventions globally [78–81]. Consistent with prior research, the reviewed interventions delivered through mobile apps and wearable devices provided participants with tools to monitor progress, receive feedback, and sustain engagement over time. The role of self-monitoring and feedback was particularly evident in studies where reminders or ‘nudges’ led to improved adherence [60, 61, 65, 67–69, 72], suggesting that ongoing interaction and support are key components of success. While many of the included interventions demonstrated improvements in PA behaviors, the heterogeneity of study designs and populations (15/16 articles were from Arabic-speaking countries that are considered advanced economies, so adaptations for use in LMIC Arab-Speaking nations are needed, and this is an area for future research) highlights the need for culturally tailored approaches, particularly if these approaches are to be used across the 22 nations within the League of Arab States. For example, interventions that incorporate gender-specific programming, culturally relevant messaging, and considerations for local health beliefs showed higher engagement and effectiveness [82–85]. This reinforces the importance of embedding digital interventions within the social and cultural context of Arabic-speaking countries to enhance uptake and sustainability.
The results of this review align with global literature showing the effectiveness of digital health interventions in promoting PA. Consistent with prior research, interventions delivered through mobile apps and wearable devices provided participants with tools to monitor progress, receive feedback, and sustain engagement over time [86–89]. Interestingly, even interventions resulting in modest increases in steps demonstrated meaningful improvements in anthropometric indicators such as BMI, waist circumference, and body fat percentage, underscoring the potential for small, sustained changes to yield significant health benefits. [71, 86]
Given the rising prevalence of NCDs in the region, these findings have significant implications for public health policy and practice. Digital interventions present a scalable and cost-effective strategy to reach diverse populations, including those in rural or underserved areas with limited access to traditional healthcare services. Importantly, the use of mobile apps and wearable devices provides opportunities for real-time data collection and remote monitoring, which can be integrated into healthcare systems to improve population-level surveillance and management of chronic conditions.
However, the success of these interventions is dependent on addressing barriers such as digital literacy, cultural tailoring and acceptability, access to reliable technology, and user engagement. It is important to recognize that geographical coverage in digital health interventions plays a crucial role in the culturally diverse Arab League, which consists of 22 member countries, each with its own unique cultural, social, and economic contexts. This diversity impacts health behaviors and the adoption of technology. By including various countries helps to ensure that specific population needs are addressed and to enhance the generalizability of research findings [90].
Understanding the necessary cultural and linguistic adaptations is key for the successful implementation of digital health interventions within diverse populations. For instance, adapting digital programs for Syrian refugees in the UK underscores the importance of cultural sensitivity when tackling mental health concerns, such as suicidal thoughts [91]. Language and cultural barriers may hinder individuals’ ability to effectively utilize digital health resources. This issue is also evident in Germany, where Arabic-language digital programs experience lower adoption rates compared to their German counterparts [30]. Ensuring that these interventions are culturally and linguistically tailored can significantly increase their accessibility and effectiveness.
In lower-income Arab countries, the adoption of healthcare technology is affected by inadequate infrastructure, low digital literacy, and inconsistent regulatory frameworks [92]. This is because many of these nations lack the necessary resources and infrastructure to utilize digital health tools effectively. To address these challenges, it is critical to employ strategies such as user-centered design, seamless integration of new tools with existing systems, and gain political support. Economic constraints further complicate this situation, as limited funding restricts investment in essential infrastructure [93]. However, with improved planning and investment, these obstacles can be navigated, ultimately leading to enhanced healthcare access and outcomes across the region.
The increasing utilization of mobile phones in low- and middle-income countries enhances the ability of digital health services to reach a broader audience across the league of Arab States, especially in resource-limited areas. This allows telemedicine and digital technologies to significantly improve healthcare delivery by facilitating disease diagnosis, enabling early illness detection, reducing costs, and providing essential health services in a more accessible manner, particularly for individuals in remote or underserved regions [94].
The finding that reminders and behavioral prompts enhanced adherence suggests that interventions should prioritize interactive features that foster motivation and accountability. Furthermore, collaboration between public health officials, technology developers, and community stakeholders will be essential to design solutions that are equitable and inclusive.
Strengths and limitations
This review highlights the growing body of research supporting the use of digital PA interventions in Arabic-speaking countries. A notable strength of the included studies was the widespread integration of behavior change theories, such as SCT and the Health Belief Model, providing a strong conceptual foundation for intervention design. The diversity of study designs, ranging from randomized controlled trials to pre-post experimental studies, also offered a comprehensive view of intervention effectiveness.
Nevertheless, several limitations warrant consideration. The variability in intervention duration, delivery modality, and outcome measures made direct comparisons challenging. Some studies had small sample sizes, which may limit generalizability. Additionally, only one study was conducted in low- and middle-income countries across the League of Arab States, despite the significant burden of NCDs in these countries. This gap highlights a need for future research that prioritizes equity and accessibility across the full range of Arabic-speaking populations within this region.
Future directions for research
Future studies should focus on long-term sustainability and scalability of digital interventions. Research exploring strategies to integrate digital health tools into existing healthcare systems will be critical, particularly for chronic disease management. Additionally, more rigorous designs, including large-scale randomized controlled trials, are needed to strengthen the evidence base. Efforts should also be directed toward understanding how gender, socioeconomic status, and cultural norms influence engagement and outcomes, to ensure interventions are both effective and culturally sensitive.
CONCLUSION
Digital health interventions represent a promising avenue for increasing PA and addressing the growing burden of NCDs in Arabic-speaking countries. This review demonstrates that such interventions can effectively improve PA behaviors and related health outcomes when thoughtfully designed and culturally adapted. By leveraging technology and behavior change theory, there is an opportunity to create sustainable, accessible solutions that promote health equity and support population-level wellness. The evidence from this review suggests a promising potential for digital-based PA interventions in enhancing the health status and behaviors of populations. A range of interventions, encompassing diverse strategies such as phone calls, mobile applications, social media platforms, and wearable devices like pedometers, yielded various degrees of success, with several studies demonstrating significant improvements in PA levels, anthropometric measurements, dietary habits, and psychosocial parameters. Notably, the interventions showing the most effectiveness tended to be those that integrated multiple digital tools, utilized a theoretical or conceptual framework for the intervention, and fostered engagement through ‘nudges’ to participants. Most of the interventions employed focus on using digital health as a tool for motivation and encouragement to ensure adherence to a PA plan, and/or sustain healthy behaviors. This approach might explain the positive results indicated in this review. Despite these encouraging findings, the limited geographical coverage of the studies, primarily focusing on Saudi Arabia, Qatar, the United Arab Emirates, Oman, and Egypt, along with the variable sample sizes and research designs employed, indicate the need for larger-scale and more diverse studies. Further studies are necessary to identify the most effective interventions, particularly concerning long-term impact on health outcomes. Through this, digital technologies can be effectively utilized to promote PA and overall health in the Arab region.
Supplementary Material
Supplementary_material_FINAL_oqaf028
PRISMA-ScR-Fillable-Checklist_10Sept2019_oqaf028
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kardan M, Jung A, Iqbal M et al. Efficacy of digital interventions on physical activity promotion in individuals with noncommunicable diseases: an overview of systematic reviews. BMC Digital Health 2024;2:40. 10.1186/s 44247-024-00097-6 · doi ↗
- 2World Health Organization . Going digital for noncommunicable diseases: the case for action, Geneva, Switzerland: World Health Organization, Accessed Sept 3rd, 2025. https://iris.who.int/handle/10665/378478
- 3Xiong S, Lu H, Peoples N et al. Digital health interventions for non-communicable disease management in primary health care in low-and middle-income countries. NPJ Digit Med 2023;6:12. 10.1038/s 41746-023-00764-436725977 PMC 9889958 · doi ↗ · pubmed ↗
- 4world Health Organization . Noncommunicable diseases, Geneva, Switzerland: World Health Organization, Accessed Sept 3rd, 2025. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
- 5Manderson L, Jewett S. Risk, lifestyle and non-communicable diseases of poverty. Glob Health 2023;19:13, 13. 10.1186/s 12992-023-00914-z PMC 997826936864476 · doi ↗ · pubmed ↗
- 6Mendenhall E, Kohrt BA, Norris SA et al. Non-communicable disease syndemics: poverty, depression, and diabetes among low-income populations. Lancet (London, England) 2017;389:951–63. 10.1016/s 0140-6736(17)30402-628271846 PMC 5491333 · doi ↗ · pubmed ↗
- 7Chen S, Kuhn M, Prettner K et al. The macroeconomic burden of noncommunicable diseases in the United States: estimates and projections. P Lo S One 2018;13:e 0206702. 10.1371/journal.pone.020670230383802 PMC 6211719 · doi ↗ · pubmed ↗
- 8Lago-Peñas S, Rivera B, Cantarero D et al. The impact of socioeconomic position on non-communicable diseases: what do we know about it? Perspect Public Health 2021;141:158–76. 10.1177/175791392091495232449467 · doi ↗ · pubmed ↗