Unusual Midline Chest Wall Cellulitis in an Infant Without Trauma or Skin Barrier Disruption
Morihide Kanawa, Hiro Nakao, Tatsuki Ikuse, Mitsuru Kubota, Kensuke Shoji

TL;DR
A one-year-old child developed chest wall cellulitis without trauma or skin issues, suggesting a rare blood-borne infection.
Contribution
This case highlights hematogenous cellulitis as a possible cause in pediatric patients with atypical infections.
Findings
Cellulitis was localized to the xiphoid process without abscess or osteomyelitis.
Methicillin-susceptible Staphylococcus aureus was identified from blood culture.
Imaging and microbiological evaluation supported diagnosis and management.
Abstract
Cellulitis in children usually develops on the extremities or face following minor trauma or skin barrier disruption, and involvement of the trunk is uncommon. We report a one-year-old previously healthy boy who presented with fever and a rapidly enlarging anterior chest wall mass. Laboratory tests revealed elevated inflammatory markers without evidence of immunological abnormality. Ultrasonography showed a 12-mm swelling beneath the lower sternum with increased blood flow but no abscess. Cellulitis was diagnosed, and intravenous cefazolin was initiated. Blood culture obtained on admission grew methicillin-susceptible Staphylococcus aureus. On hospital day nine, contrast-enhanced magnetic resonance imaging demonstrated cellulitis localized to the xiphoid process without evidence of osteomyelitis. The patient completed two weeks of intravenous cefazolin and was discharged without…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1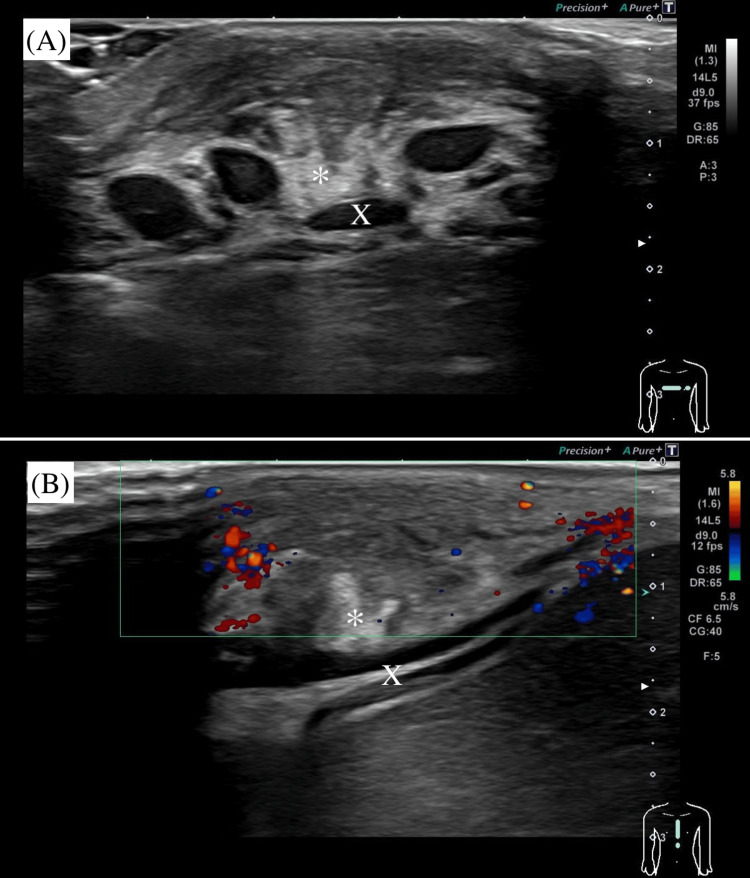 Figure 2
Figure 2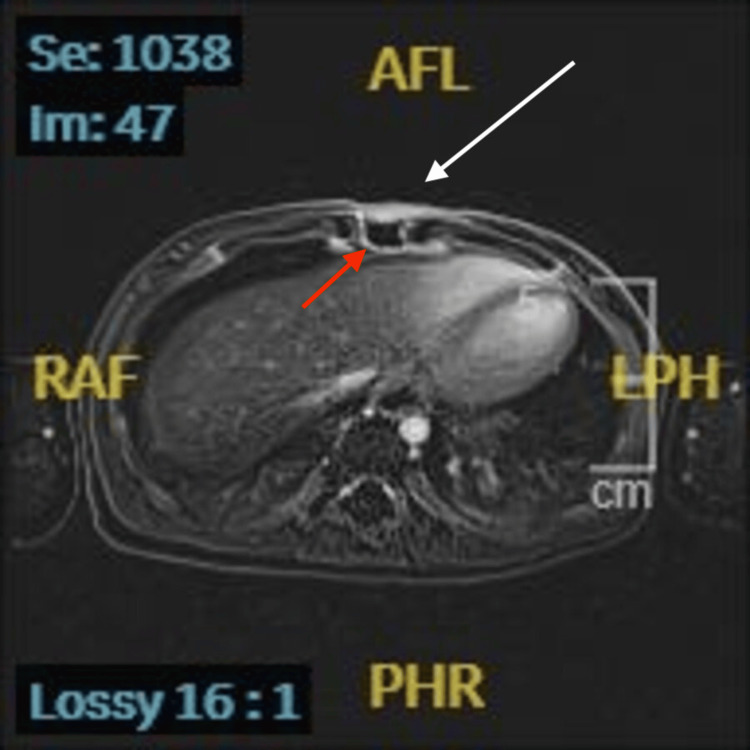 Figure 3
Figure 3| Parameter | Patient value | Reference value |
| White blood cells | 10460/μL | 4300–19600 |
| Neutrophils | 40.9% | 20–35 |
| Lymphocytes | 48.1% | 55–70 |
| Monocytes | 9.9% | 2–8 |
| Eosinophils | 0.8% | 1–4 |
| Basophils | 0.3% | 0–1 |
| Red blood cells | 405×104/μL | 393–538 |
| Hemoglobin | 10.2 g/dL | 10.5–14.1 |
| Platelets | 39.6×104/μL | 16.8–65.0 |
| C3‡ | 105 mg/dL | 65–135 |
| C4‡ | 21 mg/dL | 17–45 |
| CH50‡ | 40.7 CH50/mL | 25.0–48.0 |
| IgA‡ | 57 mg/dL | 16–128 |
| IgE‡ | 538.0 IU/mL | 5.4–1100.0 |
| IgG‡ | 650 mg/dL | 460–1220 |
| IgM‡ | 120 mg/dL | 57–260 |
| HBs antibody‡ | Positive | – |
| Total bilirubin | 0.31 mg/dL | 0.16–0.67 |
| Aspartate aminotransferase | 33 U/L | 23–57 |
| Alanine aminotransferase | 19 U/L | 9–38 |
| Lactate dehydrogenase | 285 U/L | 202–437 |
| Total protein | 6.8 g/dL | 5.7–7.5 |
| Albumin | 3.9 g/dL | 3.4–4.7 |
| Blood urea nitrogen | 9.4 mg/dL | 3.7–18.6 |
| Creatinine | 0.18 mg/dL | 0.16–0.33 |
| Sodium | 134 mmol/L | 135–143 |
| Chloride | 102 mmol/L | 101–110 |
| Potassium | 4.8 mmol/L | 3.6–5.1 |
| Creatine kinase | 97 U/L | 39–299 |
| C-reactive protein | 5.09 mg/dL | <0.3 |
| Soluble interleukin-2 receptor† | 829 U/mL | 157–474 |
| Erythrocyte sedimentation rate‡ | 19 mm/h | 0–10 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Antimicrobial Resistance in Staphylococcus · Infective Endocarditis Diagnosis and Management
Introduction
In children, cellulitis most frequently affects the extremities or facial areas, often following minor trauma or skin disruption [1]. In contrast, cellulitis of the trunk is rare. In a cohort comprising both adults and children, cellulitis of the trunk accounted for only 4.5% of all cases, underscoring its rarity [2]. When evaluating an acquired anterior chest wall mass in children, the differential diagnosis includes trauma, benign tumor, malignant neoplasm, and inflammatory or infectious causes such as Tietze syndrome, cyst, sternal osteomyelitis, and abscess. Although cellulitis is generally diagnosed clinically, imaging modalities, such as ultrasonography and magnetic resonance imaging (MRI), may assist in challenging cases, that is, atypical or complicated cases, by ruling out abscess and by evaluating the extent of infection, including possible deep involvement, the risk of systemic spread, or overlap with other chest wall conditions.
Case presentation
A one-year-old boy was referred to our hospital for evaluation of a mass in the anterior chest. He had had a fever starting four days before admission, and the parent reported noticing the swelling a day before. The patient was up to date with routine immunizations, including Bacillus Calmette-Guerin (BCG). He had no notable perinatal, developmental, or past medical history. He had no trauma. On presentation, he was afebrile, with a pulse of 110 beats/min and a respiratory rate of 36 breaths/min. The patient’s weight was 8.4 kg, height was 76 cm, and the calculated Kaup index was 14.5. Physical examination revealed a well-circumscribed, smooth-marginated, protruding lesion measuring 30 mm in diameter on the anterior chest, surrounded by an area of pale erythema measuring 50 mm in diameter, which had no tenderness, heat, or mobility (Figure 1).
Photograph of the anterior chest wall showing a well-circumscribed, smooth-marginated, 30 mm subcutaneous mass on the midline over the xiphoid process.
No cardiac murmur was detected. Echocardiography was not performed, as there were no clinical signs suggestive of endocarditis. The results of laboratory testing are shown in Table 1.
Inflammatory markers were elevated, whereas immunological test results were within normal range. Total IgE was elevated at 538 IU/mL. However, the patient had no history or clinical features suggestive of atopy, such as eczema, wheezing, or allergic rhinitis, and no signs consistent with hyper-IgE syndrome. Soluble interleukin-2 receptor was measured as part of the evaluation for possible hematological disorders. Ultrasonography revealed a 12-mm swelling in soft tissue located anterior to the lower end of the sternum, corresponding to the xiphoid process and increasing blood flow around the mass, with no evidence of abscess (Figure 2).
Ultrasonographic image of the anterior chest wall showing a 12-mm subcutaneous hypoechoic lesion () with increased peripheral vascularity, located anterior to the xiphoid process (X). No evidence of abscess was observed.*
Cellulitis was diagnosed, and intravenous cefazolin (100 mg/kg/day, every 8 hours) was administered. Blood culture on admission was positive for methicillin-susceptible Staphylococcus aureus the next day. Follow-up blood cultures obtained on hospital day three (two sets) were both negative. During hospitalization, the patient remained afebrile. The erythema resolved by hospital day three, and the swelling gradually subsided, disappearing completely by hospital day eight. On hospital day nine, contrast-enhanced MRI demonstrated inflammatory changes confined to the soft tissue overlying the xiphoid process, without evidence of osteomyelitis (Figure 3).
Contrast-enhanced axial T1-weighted MRI demonstrating subcutaneous swelling and enhancement (white arrow) at the xiphoid level (red arrow), consistent with cellulitis.
The patient completed two weeks of cefazolin and was discharged uneventfully.
Discussion
In this patient, the lesion occurred on the anterior chest wall, a highly unusual site for cellulitis. More importantly, however, the clinical presentation was atypical: the lesion was painless, without warmth, and the patient remained afebrile at admission. This lack of classical inflammatory signs contributed to the diagnostic challenge. Additionally, the absence of skin barrier disruption or underlying chronic condition made the source of infection unclear. BCG vaccination has been reported as a potential cause of soft tissue infection in the chest wall [3]. In the present case, testing for mycobacteria, including BCG, was not performed. However, since S. aureus was isolated from blood cultures and the patient improved with antibiotic therapy targeting S. aureus, mycobacteria were not suspected as the causative pathogen. Several reports have described infections around the sternum caused by a congenital dermoid sinus of the anterior chest region [4]; however, in our case, ultrasonography demonstrated no fistulous tract, making this diagnosis unlikely.
Although the clinical presentation in our case was atypical, several findings supported the diagnosis of cellulitis. Laboratory testing showed elevated inflammatory markers, blood culture yielded S. aureus, and imaging revealed inflammatory changes limited to the subcutaneous tissue without abscess formation. Moreover, the lesion improved promptly with intravenous cefazolin. Taken together, these findings confirmed the diagnosis of cellulitis despite the unusual clinical appearance. In pediatric skin and soft-tissue infections, ultrasonography has been reported to have a sensitivity of 89.9% and specificity of 79.9% for distinguishing cellulitis from abscess [5], supporting its role as a useful adjunct while acknowledging its limitations. Moreover, cellulitis and osteoarticular infection have been reported to coexist in 11% of pediatric cases [6], and MRI is regarded as superior for evaluating possible osteomyelitis or deep extension. In our case, ultrasonography helped characterize the lesion, and MRI appropriately excluded osteomyelitis.
In our case, immunoglobulin levels, complement components, and anti-HBs titers were all within normal limits, suggesting no apparent immunodeficiency. However, we acknowledge that this work-up does not exclude all forms of primary immunodeficiency. Disorders such as chronic granulomatous disease or hyper-IgE syndrome, which can predispose patients to S. aureus infection, may not be ruled out by these tests alone.
Infective endocarditis was considered as a differential diagnosis in view of the history of fever and positive blood culture. However, the patient had no cardiac murmur or other findings suggestive of infective endocarditis, and the chest wall lesion was consistent with localized cellulitis rather than a secondary embolic lesion. In addition, follow-up blood cultures obtained on hospital day three were negative, arguing against persistent bacteremia, which is typically required for the diagnosis of endocarditis. Therefore, echocardiography was not performed, and endocarditis was considered unlikely.
In this case, we considered the possibility that bacteremia originated from an unrecognized primary focus and subsequently localized to the chest wall. Alternatively, cellulitis itself may have represented the primary source of bacteremia, as S. aureus skin infections are a well-known cause of bloodstream infection. However, the atypical clinical presentation at admission and the absence of local inflammatory signs made it difficult to determine whether the chest wall lesion was the source or a metastatic focus.
Hematogenous dissemination of S. aureus to the skin is rarely documented. Cutaneous lesions in bacteremia are usually observed in the setting of metastatic infection or infective endocarditis rather than as isolated cellulitis. Del Giudice et al. noted that skin manifestations of S. aureus bacteremia without endocarditis are extremely rare [7]. In children, reports of true hematogenous cellulitis remain scarce.
Dissemination is facilitated by microbial virulence factors such as α-toxin, protein A, and surface adhesins (MSCRAMMs), including clumping factor and fibronectin-binding proteins. Some strains harbor Panton-Valentine leukocidin (PVL), which is strongly associated with recurrent or deep abscesses; although its contribution to invasive dissemination is variable, both PVL and α-toxin can intensify local inflammation [8]. Host defenses, particularly intact skin barriers, neutrophil function, and innate immunity, are essential to prevent spread, while inborn errors of immunity may predispose certain patients to invasive or recurrent S. aureus infection [9]. Although the available evidence is limited, the rarity of pediatric cases highlights the value of individual reports. In our patient, the presence of S. aureus bacteremia without features of endocarditis, imaging evidence of localized cellulitis without abscess or osteomyelitis, and resolution under pathogen-directed therapy support hematogenous cellulitis as a plausible explanation, while acknowledging both its rarity in children and the alternative possibility that the chest wall lesion represented the primary focus of bacteremia.
A major limitation of this report is that histopathological confirmation was not obtained, as a skin biopsy was not performed. Therefore, the precise etiology of the lesion cannot be definitively established. While hematogenous dissemination of S. aureus was considered most plausible, other possibilities include rupture of a congenital cyst with secondary infection, scrofuloderma arising from an underlying tuberculous focus, or secondary infection following an insect bite. Recognition of these alternatives highlights the diagnostic uncertainty and the importance of considering a broad differential diagnosis when evaluating midline chest wall lesions in children.
Notably, the patient presented with fever four days before admission, and a positive blood culture for methicillin-susceptible S. aureus was obtained. These findings raise the possibility of hematogenous dissemination, whereby bacteremia from an unrecognized primary focus resulted in localization to the anterior chest wall.
Furthermore, this case underscores the clinical significance of midline inflammatory lesions in children. Such presentations may represent the initial manifestation of systemic infection or serve as a portal for dissemination. Prompt recognition, microbiological evaluation, and appropriate therapy are essential to prevent progression to severe complications.
Conclusions
Although hematogenous cellulitis is rare, particularly in the absence of underlying immunodeficiency or apparent skin barrier disruption, this case highlights that it should be considered in children presenting with soft-tissue infection at uncommon sites. Recognition of such cases is important, as delayed diagnosis may lead to progression and more severe complications. When the presentation is atypical or the site is unusual, imaging and microbiological evaluation may be considered as part of the differential diagnosis to guide management. Further accumulation of similar reports will help to clarify the clinical characteristics and optimal management of hematogenous cellulitis in pediatric patients, and to raise awareness that midline inflammatory lesions in children may herald systemic infection and therefore warrant careful evaluation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cellulitis in children: a retrospective single centre study from Australia BMJ Paediatr Open Salleo E Mac Kay CI Cannon J King B Bowen AC 05202110.1136/bmjpo-2021-001130 PMC 828761234337163 · doi ↗ · pubmed ↗
- 2Cellulitis incidence in a defined population Epidemiol Infect Ellis Simonsen SM van Orman ER Hatch BE Jones SS Gren LH Hegmann KT Lyon JL 29329913420061649013310.1017/S 095026880500484 XPMC 2870381 · doi ↗ · pubmed ↗
- 3Chest wall tuberculosis after Bacillus Calmette-Guérin vaccination Pediatr Infect Dis J Iwai M Fukushima T Watanabe N 0541202210.1097/INF.000000000000367636102718 · doi ↗ · pubmed ↗
- 4Congenital dermoid sinus of anterior chest: case report and review of literature Int J Surg Case Rep Alenezi M 10859110920233753610010.1016/j.ijscr.2023.108591 PMC 10415688 · doi ↗ · pubmed ↗
- 5Point-of-care ultrasonography for the diagnosis of skin and soft tissue abscesses: a systematic review and meta-analysis Ann Emerg Med Gottlieb M Avila J Chottiner M Peksa GD 67777620203208138310.1016/j.annemergmed.2020.01.004 · doi ↗ · pubmed ↗
- 6Rate of concomitant cellulitis and osteoarticular infections in a pediatric population J Pediatr Orthop B Ryan CB Romere CM Shah R Souder CD Ellington M 4764803220233644535710.1097/BPB.0000000000001037 · doi ↗ · pubmed ↗
- 7Skin infections caused by Staphylococcus aureus Acta Derm Venereol Del Giudice P 0100202010.2340/00015555-3466 PMC 912895132207539 · doi ↗ · pubmed ↗
- 8Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management Clin Microbiol Rev Tong SY Davis JS Eichenberger E Holland TL Fowler VG Jr 6036612820152601648610.1128/CMR.00134-14PMC 4451395 · doi ↗ · pubmed ↗