Prevalence of Intestinal Amebiasis Among Saudi Residents Living in the Al-Baha Region, Saudi Arabia
Ashraf G Tımsah, Ibrahim Shatla, Mohammed M Alzahrani, Abdulaziz A Alzahrani, Faisal M Alzahrani, Osama A Alghamdi, Muhannad M Alghamdi, Saeed Alghamdi, Adel K Alghamdi, Majed A Alghamdi, Attia A Attia Alzahrani

TL;DR
This study finds that intestinal amebiasis caused by Entamoeba histolytica is prevalent in Saudi Arabia's Al-Baha region, especially among children aged 6-12.
Contribution
The study provides new prevalence data for E. histolytica in the Al-Baha region and identifies risk factors and clinical associations.
Findings
8.25% of 6,471 stool samples tested positive for E. histolytica, with children aged 6-12 years being the most affected group.
Cysts were the most common form detected (97%), and trophozoite presence was strongly associated with blood in stool and radiological complications.
Al-Baha city had the highest infection rate, suggesting localized transmission and sanitation challenges.
Abstract
Background: Entamoeba histolytica is a pathogenic protozoan parasite that can cause amoebiasis, which is one of the leading causes of death from parasitic infections. Aims: This study aimed to estimate the prevalence of intestinal amebiasis among Saudi patients who attended the two major hospitals, including King Fahad Hospital in Al-Baha and Prince Meshari Hospital in Baljurashi, which is a big governorate in Al-Baha, in addition to the Central Laboratory in the Al-Baha region. Methods: This is a retrospective study of demographic, clinical, radiological, and laboratory data collected from patients' records covering the period from January 2019 to December 2024. Results: Out of a total of 6,471 stool samples examined, 534 (8.25%) were positive for E. histolytica in the form of cysts or trophozoites. Of these positive cases, 305 (57.1%) occurred in males, while 229 (42.9%) were in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
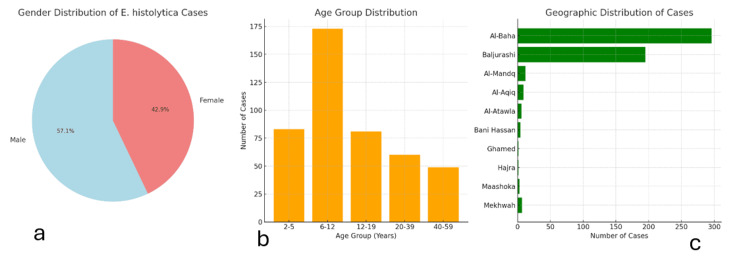 Figure 1
Figure 1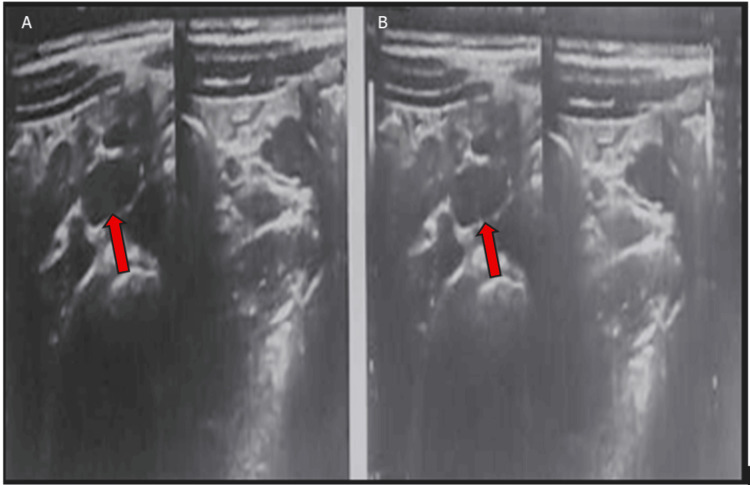 Figure 2
Figure 2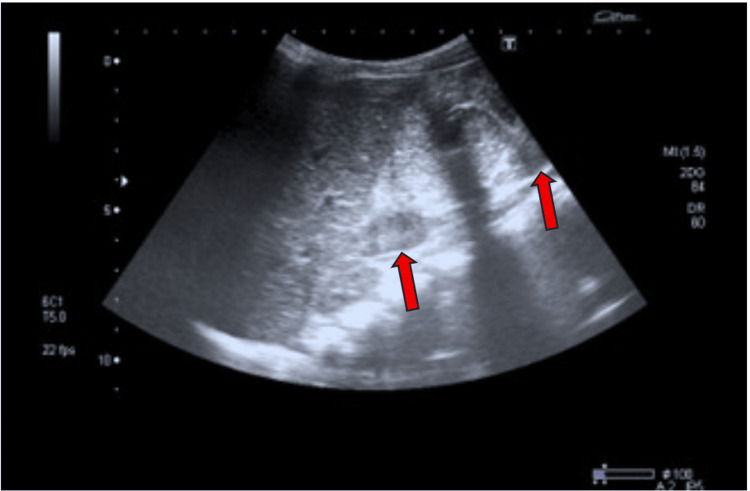 Figure 3
Figure 3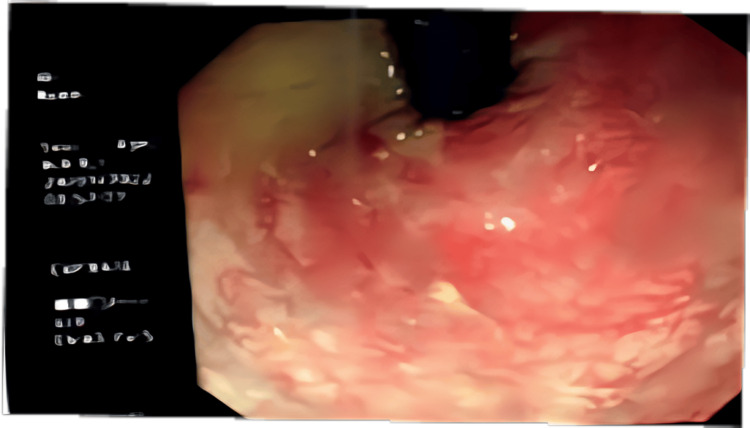 Figure 4
Figure 4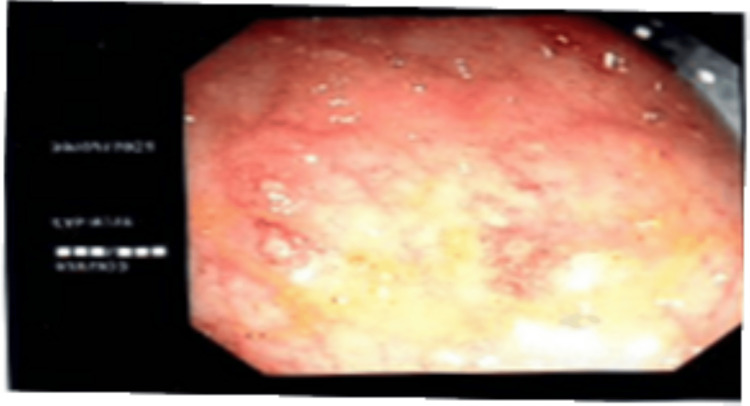 Figure 5
Figure 5| Characteristics | Variable | Number | % |
| Gender | Male | 305 | 57.1 |
| Female | 229 | 42.9 | |
| Age | Group 1 (2-5) | 83 | 15.5 |
| Group 2 (6-12) | 173 | 32.4 | |
| Group 3 (12-19) | 81 | 15.2 | |
| Group 4 (20-39) | 60 | 11.2 | |
| Group 5 (40-59) | 49 | 9.2 | |
| Group 6 (60 and more) | 88 | 16.5 | |
| Residence | Al-Aqiq | 9 | 1.7 |
| Al-Atawla | 6 | 1.1 | |
| Al-Baha | 296 | 55.4 | |
| Al-Mandq | 12 | 2.2 | |
| Baljurashi | 195 | 36.5 | |
| Bani Hassan | 4 | 0.7 | |
| Ghamed | 1 | 0.2 | |
| Hajra | 1 | 0.2 | |
| Maashoka | 3 | 0.6 | |
| Mekhwah | 7 | 1.3 |
| Findings | Number | % | ||
| Macroscopic findings | Consistency of stool | Formed | 49 | 9.2 |
| Semi-formed | 240 | 44.9 | ||
| Watery | 222 | 41.6 | ||
| Mucoid | 20 | 3.7 | ||
| Bloody | 3 | 0.6 | ||
| Stool colour | Black | 6 | 1.1 | |
| Brown | 181 | 33.9 | ||
| Green | 136 | 25.5 | ||
| Red | 22 | 4.1 | ||
| Tarry | 2 | 0.4 | ||
| Yellow | 187 | 35 | ||
| Blood | Null | 458 | 85.8 | |
| Present | 76 | 14.2 | ||
| Indigested food | Null | 400 | 74.9 | |
| Present | 134 | 25.1 | ||
| Cysts | Null | 16 | 3 | |
| Present | 518 | 97 | ||
| Microscopic findings | Coinfections | Ascaris lumbricoides | 1 | 0.2 |
| Bacterial infection (non-specific) | 30 | 5.6 | ||
| Escherichia coli | 11 | 2.1 | ||
| Enterobius vermicularis | 1 | 0.2 | ||
| Null | 486 | 91.1 | ||
| Yeast | 5 | 0.9 | ||
| WBC | 1-15 cell/μL | 123 | 23 | |
| 16-75 cell/μL | 134 | 25.1 | ||
| More than 76 cell/μL | 168 | 31.5 | ||
| Null | 109 | 20.4 | ||
| RBC | 0-5 cell/μL | 50 | 9.4 | |
| 11-25 cell/μL | 148 | 27.7 | ||
| 5-10 cell/μL | 193 | 36.1 | ||
| More than 26 cell/μL | 59 | 11 | ||
| Null | 84 | 15.7 | ||
| Vegetative form (trophozoite) | Null | 404 | 75.7 | |
| Present | 130 | 24.3 | ||
| Category | Finding | Number | % |
| Radiology | Colonic mass US (CT abdomen revealed a 3.4 cm mass in diameter) | 1 | 0.2 |
| CTW/distension | 4 | 0.8 | |
| Enlarged ML US | 2 | 0.4 | |
| Dilated bowel US | 2 | 0.4 | |
| Distension, edematous, and thick-walled US | 13 | 1.9 | |
| Null | 194 | 36.3 | |
| Complications | Bloody diarrhea | 3 | 0.6 |
| Diarrhea alternates with constipation | 6 | 1.2 | |
| Colonic mass | 1 | 0.2 | |
| Boats of severe diarrhea | 25 | 3.8 | |
| Mucoid diarrhoea | 20 | 3.7 | |
| Tarry stool | 2 | 0.4 | |
| Severe anemia | 1 | 0.2 | |
| Null | 477 | 89.3 |
| Examination | Category | Cyst, n (%) | Trophozoite, n (%) | P-value |
| Consistency of stool | Formed | 35 (8.7) | 14 (10.8) | >0.05 |
| Semi-formed | 204 (50.5) | 36 (27.7) | <0.001 | |
| Watery | 153 (37.9) | 69 (53.1) | <0.01 | |
| Mucoid | 11 (2.7) | 9 (6.9) | <0.05 | |
| Bloody | 1 (0.2) | 2 (1.5) | >0.05 | |
| WBC | Null | 33 (8.2) | 12(9.2) | >0.05 |
| 1-15 cells/μL | 93(23) | 30 (23.1) | >0.05 | |
| 16-75 cells/μL | 113 (28) | 21 (16.2) | <0.01 | |
| >76 cells/μL | 43 (10.6) | 12 (9.2) | >0.05 | |
| RBC | Null | 63 (15.6) | 21 (16.2) | >0.05 |
| 5-10 cells/μL | 165 (40.8) | 28 (21.5) | <0.001 | |
| 11-25 cells/μL | 106 (26.2) | 42 (32.3) | >0.05 | |
| >26 cells/μL | 32 (7.9) | 27 (20.8) | <0.001 | |
| Radiology | Finding | 13 (7.7) | 9 (10.9) | >0.05 |
| No finding | 118 (92.3) | 73 (89.1) | ||
| Complications | Complications | 27 (6.7) | 30 (23.1) | <0.001 |
| No complications | 377 (93.3) | 100 (76.9) | ||
| Colonoscopy | Finding | 19 (16.7) | 14 (23) | 0.3112 |
| No Finding | 95 (83.3) | 47 (77) | ||
| Blood | Present | 31 (7.7) | 45 (34.6) | <0.001 |
| Null | 373 (92.3) | 85 (65.4) | ||
| Mucus | Present | 326 (80.7) | 108 (83.1) | >0.05 |
| Null | 78 (19.3) | 22 (16.9) | ||
| Indigested food | Present | 63 (15.6) | 71 (54.6) | <0.001 |
| Null | 341 (84.4) | 59 (45.4) |
| Parameter | Cystic forms, mean ± SD | Trophozoite, mean ± SD | P-value | Significance |
| WBC | 10.1 ± 4.92 | 9.3 ± 5.9 | 0.513 | >0.05 |
| HB | 12.07 ± 1.93 | 12.66 ± 2.15 | 0.195 | >0.05 |
| PCV | 36.55 ± 5.03 | 37.77 ± 5.69 | 0.306 | >0.05 |
| MCV | 75.68 ± 9.7 | 79.44 ± 7.51 | 0.028 | < 0.05 |
| MCH | 25.53 ± 2.82 | 26.96 ± 4.28 | 0.100 | >0.05 |
| MCHC | 32.96 ± 1.58 | 33.43 ± 1.42 | 0.134 | >0.05 |
| PLT | 364.37 ± 115.76 | 351.79 ± 140.97 | 0.667 | >0.05 |
| RDW | 14.14 ± 1.62 | 14.39 ± 2.97 | 0.669 | >0.05 |
| Neutrophils | 53.41 ± 22.33 | 53.27 ± 22.19 | 0.976 | >0.05 |
| Lymph | 36.26 ± 21.28 | 35.3 ± 20.97 | 0.832 | >0.05 |
| Mono | 9.39 ± 5.19 | 9.44 ± 5.25 | 0.965 | >0.05 |
| Esino | 1.43 ± 1.52 | 1.74 ± 2.37 | 0.507 | >0.05 |
| Baso | 0.34 ± 0.25 | 0.67 ± 3.26 | 0.605 | >0.05 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Parasites and Host Interactions · Global Health and Surgery
Introduction
*Entamoeba histolytica *(E. histolytica) is a protozoan causing colonic amebiasis as well as extra-intestinal manifestations. Although 90.0% E. histolytica infections are asymptomatic, 50 million people become symptomatic, with about 100,000 deaths annually, and so it is considered the third cause of death from parasitic infections [1]. Amoebic liver abscess formation is a common complication that develops in the right lobe of the liver and is the most common extraintestinal complication. It can be seen from months to years after colonic exposure to infection [2]. Respiratory tract and cardiac brain infection complications are rare complications [1].
E. histolytica is prevalent worldwide and higher in countries with low socioeconomic status and poor hygienic habits. Countries with a high rate of infections include Africa, India, Mexico, and South America [3]. In Bangladesh, a study among three-year-old preschool children showed that E. histolytica accounted for 2.2% of dysentery cases [1]. As high as 42.0% *E. histolytica *seroprevalence has been reported in rural areas of Mexico [4]. Factors that increase mortality and complicated infections include young age, corticosteroid treatment, malignancy, malnutrition, pregnancy, and alcoholism [1]. Fulminant amoebic colitis is associated with 40% mortality [5].
In Saudi Arabia, high rates of infection with intestinal parasitic diseases among food handlers (14%), expatriates (55.7%), the Abha community (13.2%), Riyadh school children (14.2%), and patients attending hospitals (31.3%) have been reported [6]. Elsewhere in Saudi Arabia, E. histolytica was identified in 4.7% of hospital attendees in Makkah [7] and in 20% of infants and children aged 1 month to 16 years who presented with gastroenteritis in Jeddah [8]. A prevalence of E. histolytica infection was reported in 9.3% of intestinal parasitic infections [9] and in 53.3% of individuals with intestinal parasites in the Riyadh region [10]. Additionally, the parasite was detected in 2.7% of food handlers in the southern part of Saudi Arabia and in 16.15% of both symptomatic and asymptomatic individuals in Hail [11]. Consequently, E. histolytica is an important contributor to intestinal parasitic infection despite the prevalence variation, likely due to geographical and population group variations, which may reflect variation in hygiene standards. This disparity prompts studies to be conducted in more geographical locations to contribute to understanding the big picture of the burden of infection in the country at large. Additionally, to the best of our knowledge, the studies on E. histolytica in Al-Baha remain scarce. Therefore, this study investigates the prevalence of the associated clinical, radiological, and hematological manifestations. Consequently, E. histolytica remains an important contributor to intestinal parasitic infections, despite variations in its prevalence, likely due to geographical differences and population groups. The variation can also reflect variation in hygiene standards, as the low prevalence among food handlers suggests. This disparity prompts studies to be conducted in additional geographical locations to contribute to understanding the broader picture of the infection burden across the country. Therefore, this study investigates the prevalence of intestinal amebiasis and sociodemographic factors and clinical indicators among patients who attended healthcare facilities.
Materials and methods
Study populations
The population of these governorates was estimated to be over 314,532 people, representing about 91% of the total population of Al-Baha Province in Saudi Arabia [12]. We used Raosoft sample size calculator (Raosoft, Inc., Seattle, WA, USA) to calculate the sample size, with a 95% confidence interval (CI) and a 0.05 margin of error. As there were no previous studies in Al-Baha on the prevalence of E. histolytica infection, we assumed the expected population proportion to be 0.5. The resulting sample size needed was 384, and the final sample size was 534. This study utilized a cross-sectional design and retrospectively assessed the prevalence of intestinal amoebiasis among Saudi people living in the Al-Baha region, which is located in the southwestern Hejaz region of Saudi Arabia. The data for the study were collected from patients' files from January 2019 to December 2024 in King Fahad Hospital, Prince Meshari Hospital, and the Central Laboratory in Al-Baha after obtaining ethical approval from the Research Ethics Committee at the Faculty of Medicine in Al-Baha University (REC/MIC/BU-FM/2022/52).
Data collection
Data for the study were collected retrospectively from patients' files through a data source survey. The survey encompassed a wide range of information, including sociodemographic variables such as age, sex, and residency, as well as various clinical indicators such as stool consistency, color, presence of blood and mucous, white blood cell (WBC) count, red blood cell (RBC) count, presence of cysts and trophozoites, food ingestion patterns, presence of other infections, and radiological investigations. In addition, stool specimens were processed and examined using standard parasitological techniques, including direct wet mount preparation, saline concentration, and formol-ether or zinc sulfate flotation concentration methods in some cases, to diagnose E. histolytica based on the clinical manifestations.
Statistical analysis
IBM SPSS Statistics for Windows, Version 21 (Released 2013; IBM Corp., Armonk, New York, United States) was used in this study for data processing and analysis. The data were presented as mean ± standard deviation (SD) or standard error of the mean. To assess differences between groups, one-way analysis of variance (ANOVA) was employed, and we used the chi-squared test for statistical analysis, with p <0.05 set as the level of significance. We also used multivariable logistic regressions analysis to assess the association between the prevalence of E. histolytica and potential risk factors.
Results
Of the 6,471 stool samples investigated, 534 (4.7%) were positive for E. histolytica. These cases were from patients with a mean age of 26.53 ± 25.77 years and included 305 (57.1%) males and 229 (42.9%) females, with the highest rates observed in children aged 6-12 years and residents of Al-Baha city, followed by those living in Baljurashi (Table 1 and Figures 1a-1c).
Visual representation of the key demographic data for patients infected with Entamoeba histolytica.(a) Gender distribution: Males account for a higher percentage of E. histolytica infections (57.1%) compared to females (42.9%).(b) Age group distribution: Children aged 6-12 are the most affected group.(c) Geographic distribution: Most infections occur in Al-Baha city and Baljurashi.
The stool samples were semi-formed in 240 cases (44.9%), watery in 222 (41.6%), yellow in 137 (35.0%), brown in 181 (33.9%), and green in 136 (25.5%), with 76 (14.2%) containing blood and 134 (25.1%) showing undigested food. A total of 168 samples (31.5%) contained >76 WBCs/μL, 193 (36.1%) had 5-10 RBCs/μL, 404 (75.7%) contained vegetative forms, and 518 (97.0%) were positive for cysts. Co-infections included nonspecific bacteria in 30 samples (5.6%), Escherichia coli in 11 (2.1%), Ascaris lumbricoides in one (0.2%), Enterobius vermicularis in one (0.2%), and yeast in five (0.9%) (Table 2).
Ultrasound revealed a colonic mass in one patient (0.2%), which was confirmed by CT scan; enlarged mesenteric lymph nodes were observed in two patients (0.4%); and dilated bowel with distension and edematous thickened walls was noted on ultrasound in 13 patients (1.9%) (Table 3 and Figures 2-3). Complications included bouts of severe diarrhea in 25 patients (3.8%), mucoid diarrhea in 20 (3.7%), diarrhea alternating with constipation in six (1.2%), tarry stool in two (0.4%), and severe anemia in one patient (0.2%) (Table 3).
(A, B) Abdominal ultrasound images with the red arrows indicate dilated bowel loops containing echogenic foci of gaseous distension.
Ultrasound image showing bilateral mesenteric lymph nodes (LNs), measuring 13 × 6 mm on the right side and 17.4 × 4.7 mm on the left side (red arrows).
Colonoscopic findings in 175 cases (32.7%) revealed colonic hyperemia in one case (0.2%), colonic ulcers and mucosal erosions in 21 cases (3.9%), and large intestinal stricture in one case (0.2%) (Figures 4-5).
Colonoscopic image demonstrating mucosal hyperemia characterized by diffuse erythema and increased vascular pattern indicate inflammatory colitis.
Colonoscopic image showing colonic ulcerations with areas of mucosal erythema and exudative changes.
Of the 305 males, 233 (76.4%) had cysts and 72 (23.6%) had trophozoites, while among 229 females, 171 (74.7%) had cysts and 58 (25.3%) had trophozoites (p = 0.90). The presence of trophozoites was significantly associated with watery stool (p < 0.01), higher red blood cell count (p < 0.001), complications (p < 0.001), visible blood (p < 0.001), and undigested food (p < 0.001). In contrast, cysts were more common in semi-formed stools (p < 0.001) and were associated with moderate white blood cell counts (p < 0.01), while other findings showed no significant associations (p > 0.05) (Table 4).
Hematological parameters, including hemoglobin, RBC indices, and total and differential WBC counts, did not differ significantly (p > 0.05) between patients with cysts and those with trophozoites (Table 5).
Discussion
The current study showed that the prevalence of E. histolytica in the Al-Baha region of Saudi Arabia is 8.3%, which falls within the global range of infection, especially in developing countries where sanitation and hygiene standards may vary. Similar studies have been conducted in other regions of the country. For example, Jeddah, Saudi Arabia, has reported comparable prevalence rates ranging from 4% to 12% [13] and 1.6% in Riyadh [14]. Regarding gender distribution, the infection was more prevalent among males (305 cases; 57.1%) compared to females (229 cases; 42.9%). This gender disparity is often attributed to behavioral and occupational exposure, where males may be more likely to engage in outdoor activities or consume food from less hygienic sources [15]. The highest rate of infection was found in children aged 6-12 years (173 cases; 32.4%), followed by the 2-5 age group (83 cases; 15.5%). This aligns with global epidemiological trends showing increased susceptibility among children, possibly due to underdeveloped immune systems, higher exposure to contaminated environments, e.g., schools, public playgrounds, and the lack of hygiene in children [16]. Most E. histolytica cases originated from Al-Baha city (296 cases; 55.4%) and Baljurashi (195 cases; 36.5%). These areas likely have higher population densities, which may increase transmission opportunities. In contrast, rural areas such as Ghamed and Hajra reported very low numbers (one case each; 0.2%), potentially due to smaller populations or better sanitation practices in those households.
Regarding morphological forms, a large majority (518 cases; 97%) of infections were in cystic form, whereas trophozoites were identified in only 130 samples (24.3%). Cystic forms are more resilient and transmissible, while trophozoites indicate active infection. The lower trophozoite detection rate could be due to sample collection timing, as trophozoites degrade rapidly outside the host [17]. The study found co-infections, primarily with non-specific bacterial pathogens (5.6%) and E. coli (2.1%), alongside a few helminthic parasites like *A. lumbricoides *and E. vermicularis. These findings suggest possible fecal-oral transmission due to poor hygiene or inadequate water treatment [18]. Semi-formed stools characteristics were the most common (44.9%), followed by watery stools (41.6%). This indicates a classical manifestation of E. histolytica infections [19]. Blood and mucus presence, while less frequent, highlight the potential for invasive disease. Additionally, the presence of undigested food in 25.1% of cases may reflect gastrointestinal malabsorption, potentially linked to E. histolytica pathogenicity. Complications included mucous diarrhea in 3.7% and severe watery diarrhea in 2.6% of cases, with blood detected in 5.1%. Cellular analysis showed that a significant proportion of samples contained >26 RBCs/µL (11%) and >76 WBCs/µL (31.5%), supporting the diagnosis of inflammatory intestinal conditions commonly associated with invasive amebiasis [1]. Significant associations were found between trophozoite presence and watery stools (p < 0.01) or mucoid stools (p < 0.05). Semi-formed stools were more commonly associated with cyst carriers, while blood in stool was significantly associated with trophozoite presence (p < 0.001), suggesting mucosal invasion. Undigested food was also significantly more frequent in trophozoite carriers (54.6%) compared to cyst carriers (15.6%) (p < 0.001), likely due to impaired digestion from intestinal inflammation [20]. These findings support that trophozoites, rather than cysts, are responsible for active and symptomatic disease. White and red blood cells in stool were significantly associated with trophozoite presence: WBCs (16-75/μL, p < 0.01) and RBCs (>26/μL, p < 0.001), indicating that mucosal invasion by trophozoites leads to colitis with leukocyte and erythrocyte exudation, consistent with an inflammatory response [21].
Radiological findings in our study showed that, of the 213 patients (39.8%) who underwent ultrasound (US), a colonic mass was identified in only one patient (0.2%) and confirmed by CT (3.4 cm in diameter). Enlarged mesenteric lymph nodes (MLNs) were found in two cases (0.4%), dilated bowel/distension was detected in six cases (1.2%), and edematous, thickened bowel walls were observed in 13 cases (1.9%). These findings, though present in a small percentage, are clinically significant. Thickened bowel walls and lymphadenopathy are signs of active inflammation or possible complications like ameboma formation (a mass-like lesion due to chronic E. histolytica infection) [17]. In the present study, colonoscopy was performed in 175 patients (32.7%). Findings included colonic ulceration/mucosal erosion in 21 cases (3.9%), colonic hyperemia in 11 cases (2.1%), and large intestinal stricture in one case (0.2%). These results are consistent with invasive amebiasis, where E. histolytica trophozoites invade the colonic mucosa, causing ulcerations, bleeding, and potentially strictures [22]. Complications were significantly more frequent in trophozoite carriers (23.1%) compared to non-trophozoite carriers (6.7%; p < 0.001). Severe diarrhea occurred in 3.8% of cases, mucoid diarrhea in 3.7%, and anemia or bloody/tarry stools were observed in a few severe cases. These complications are consistent with manifestations of invasive amebiasis, particularly in immunocompromised or pediatric patients [23]. Hematological variables due to the effect of E. histolytica infections in our study showed no significant differences between cyst and trophozoite carriers, but mean corpuscular volume (MCV) was significantly lower in cyst infections (p < 0.05), suggesting possible microcytic anemia in chronic asymptomatic infections. Hemoglobin and WBCs were slightly lower in trophozoite carriers, but differences were not statistically significant; this implies that systemic inflammation or anemia is not a dominant feature in uncomplicated intestinal amebiasis, unless complicated by invasive disease [24].
The parasite that causes amoebic dysentery infections is usually transmitted by eating contaminated food. The greatest way to prevent the transmission of this disease is to wash hands thoroughly with soap and running water after using the bathroom and before eating. Good hygiene is the key to preventing amoeba or dysentery, and there are a number of practices and procedures that can achieve prevention, including washing vegetables and fruits with vinegar or peeling well before eating them. Drinking bottled water is important, and canned soft drinks. If you need to drink tap water, boil it first and treat it with a little iodine [25].
Despite these findings, this study has certain limitations. The cross-sectional study limits causal inference, and the use of microscopy alone may have caused misclassification since it cannot differentiate other types of amoeba, but associated clinical manifestations suggest* E. histolytica *infections. The strengths of this study are through large sample size, which provides strong statistical power and enhances the reliability of the prevalence estimates. Also, data were collected from multiple sources of major hospitals and the central laboratory, which increases the representativeness of the sample, and the study included demographic, clinical, radiological, colonoscopy, and laboratory data, giving a multidimensional view of the disease and its presentation. Future research using molecular diagnostics and larger population-based samples with more colonoscopic and radiological data is recommended.
Conclusions
E. histolytica is an important protozoan infection among preschool children. The predominance of the cystic form underscores its potential for transmission, and co-infections indicate gaps in sanitation infrastructure. Efforts are needed to evaluate the health burden of E. histolytica in Al-Baha province to improve treatment of infected individuals at primary care centers and to reinforce hygiene. Consequently, screening of school children and adults, promotion of health education, and raising awareness among the Saudi population and educational staff about E. histolytica infections and their prevention remain necessary.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Entamoeba histolytica infection Stat Pearls [Internet] Chou A Austin RL Treasure Island (FL)Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 557718/32491650 · pubmed ↗
- 2Amebic liver abscess Stat Pearls [Internet] Jackson-Akers JY Prakash V Oliver TI Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 430832/28613582 · pubmed ↗
- 3Prevalence of Entamoeba histolytica in Bingham University and environs EC Microbiology Abioye JOK Mbagwu TT Seye Babatunde 242250 Stat Pearls Publishing 152019 https://ecronicon.net/assets/ecmi/pdf/ECMI-15-00617.pdf
- 4A review of the global burden, new diagnostics, and current therapeutics for amebiasis Open Forum Infect Dis Shirley D-AT Farr L Watanabe K Moonah S 052018 https://academic.oup.com/ofid/article/5/7/ofy 161/504960110.1093/ofid/ofy 161PMC 605552930046644 · doi ↗ · pubmed ↗
- 5Fulminant amebic colitis after corticosteroid therapy: a systematic review P Lo S Negl Trop Dis Shirley DA Moonah S 0102016 https://doi.org/10.1371/journal.pntd.000487910.1371/journal.pntd.0004879 PMC 496502727467600 · doi ↗ · pubmed ↗
- 6Factors associated with high prevalence of Entamaeba histolytica/dispar infection among children in Jeddah, KSA American-Eurasian J Agric Environ Sci Jamila S 5056142014 https://www.idosi.org/aejaes/jaes 14(1)14/10.pdf
- 7Prevalence of intestinal parasites among patients of Al-Noor Specialist Hospital, Makkah, Saudi Arabia Oman Med J Zaglool DA Khodari YA Gazzaz ZJ Dhafar KO Shaker HA Farooq MU 182185262011 https://pmc.ncbi.nlm.nih.gov/articles/PMC 3191688/2204341210.5001/omj.2011.44PMC 3191688 · doi ↗ · pubmed ↗
- 8Prevalence and characters of Entamoeba histolytica infection in Saudi infants and children admitted with diarrhea at 2 main hospitals at South Jeddah: a re-emerging serious infection with unusual presentation Braz J Infect Dis Hegazi MA Patel TA El-Deek BS 3240172013 https://doi.org/10.1016/j.bjid.2012.08.0212328754610.1016/j.bjid.2012.08.021PMC 9427352 · doi ↗ · pubmed ↗