Unintentional Mitral Lateral Isthmus Block During Pulmonary Vein Isolation With a Pentaspline Pulsed‐Field Ablation Catheter
Yuhei Kasai, Takayuki Kitai, Junji Morita, Kei Murakami, Kazuhiro Satomi

TL;DR
A case shows that using a specific ablation catheter can unintentionally block the mitral isthmus during heart procedures.
Contribution
Highlights a new clinical observation about unintended lesion extension during pulmonary vein isolation with a pentaspline pulsed-field ablation catheter.
Findings
Unintentional bidirectional mitral isthmus block occurred during pulmonary vein isolation.
Careful sheath–catheter alignment is crucial to avoid unintended lesions near the mitral annulus.
Abstract
This case demonstrates an unintentional bidirectional mitral isthmus block created during pulmonary vein isolation using a pentaspline pulsed‐field ablation catheter. The finding underscores the importance of careful sheath–catheter alignment at the left inferior pulmonary vein to prevent unintended lesion extension toward the mitral annulus.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
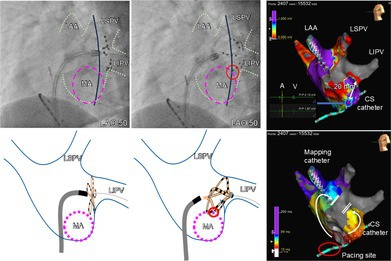 Figure 1
Figure 1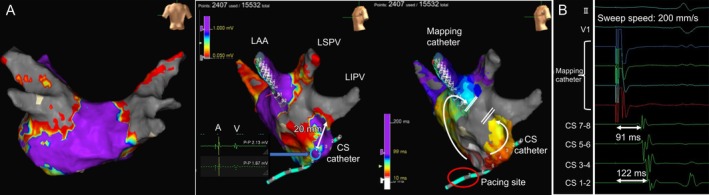 Figure 2
Figure 2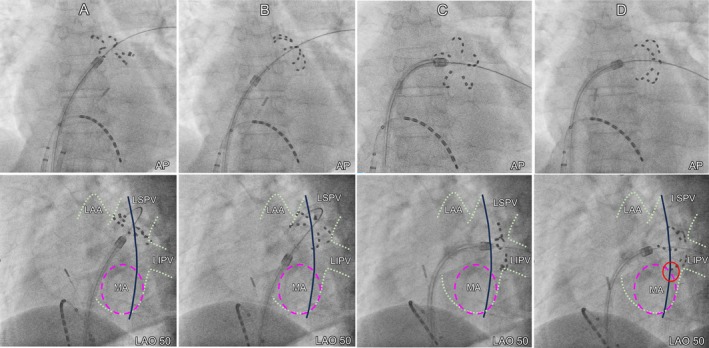 Figure 3
Figure 3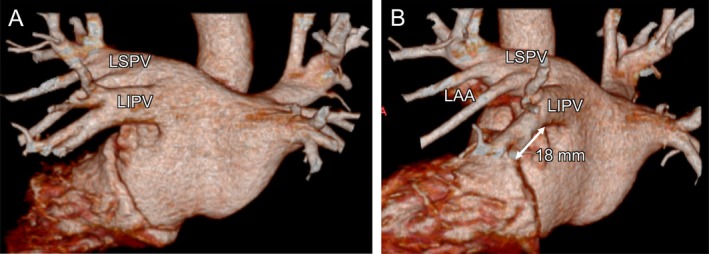 Figure 4
Figure 4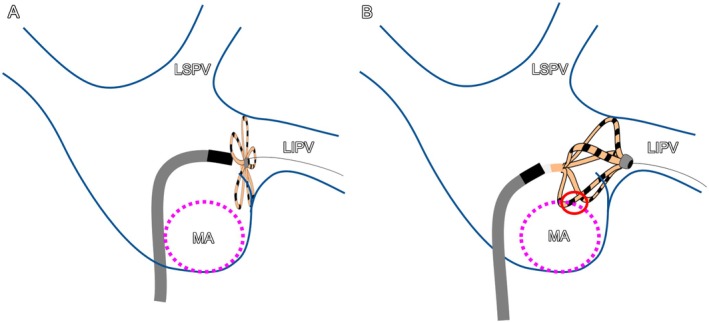 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac pacing and defibrillation studies
Pulsed‐field ablation (PFA) is a novel nonthermal technique for atrial fibrillation (AF) ablation that selectively targets myocardial cells while sparing surrounding noncardiac tissue. Recent clinical studies and real‐world data have demonstrated the procedural efficacy and reproducibility of pulmonary vein isolation (PVI) using the pentaspline PFA catheter (FARAWAVE, Boston Scientific, Marlborough, MA, USA) [1, 2]. In Japan, the clinical use of PFA is currently limited to PVI; however, in other countries, previous studies have reported the creation of mitral isthmus block lines using the FARAPULSE system [2, 3]. This typically required additional applications delivered in a flower configuration at the mitral isthmus. Here, we describe a unique case in which bidirectional mitral isthmus block was unintentionally achieved with a minimal number of applications.
A 60‐year‐old man with symptomatic paroxysmal AF underwent PFA using the FARAPULSE system (Boston Scientific) under general anesthesia (Figure 1). Following transseptal puncture using a 16.8‐Fr PFA sheath (Faradrive, Boston Scientific) and a radiofrequency guidewire (Versacross, Boston Scientific), left atrial angiography was performed with a pigtail catheter during right ventricular burst pacing (Videos S1 and S2). PVI was performed under fluoroscopic guidance (without 3D mapping) with the minimum number of applications: eight per pulmonary vein (four in the flower and four in the basket configuration, for a total of 32 applications). Post‐ablation mapping using the Ensite X system (Abbott, Chicago, IL, USA) during pacing from the coronary sinus (CS) ostium confirmed successful PVI and, unexpectedly, revealed a complete mitral isthmus block line (Figure 2A). This high‐density map, constructed using an HD Grid catheter (Abbott) with more than 2000 acquisition points, was considered sufficiently reliable to demonstrate that a true conduction block had indeed occurred across the mitral isthmus. Subsequent pacing from a mapping catheter positioned in the left atrial appendage showed a proximal‐to‐distal activation sequence in the CS (Figure 2B). These findings confirmed bidirectional conduction block across the mitral isthmus. No major ST‐segment changes were observed during the procedure, which was completed without any complications. During the 6‐month follow‐up, the patient remained free of AF and atrial tachycardia.
Although previous studies have reported the creation of a mitral isthmus block line using the FARAPULSE system, this typically required additional applications in a flower configuration at the mitral isthmus [2, 3]. To the best of our knowledge, this is the first reported case in which a bidirectional mitral isthmus block was achieved with a minimum number of applications (32 applications). A retrospective review of fluoroscopic images (Figure 3) and schematic illustration (Figure 4) showed that (1) the left superior pulmonary vein applications did not appear to have contributed to the creation of the mitral isthmus block and (2) the PFA applications in the basket configuration at the left inferior pulmonary vein (LIPV) were delivered slightly more anteriorly and proximally than those in the flower configuration.
The cause of the unintentional lesion formation is considered to be related to suboptimal alignment between the FARADRIVE sheath and the FARAWAVE catheter during the LIPV applications. In Figure 3, the tip of the FARADRIVE sheath is clearly oriented toward the anterior wall, suggesting that the catheter was inadvertently pulled anteriorly, thereby extending the application toward the lateral mitral isthmus. This misalignment would have been easier to recognize in the right anterior oblique view, whereas in the AP view it can remain subtle when using the basket configuration. Particularly during applications at the LIPV, it would have been preferable to reposition the CS catheter into the CS to serve as an anatomical landmark. Additionally, the naturally short length (18 mm in computed tomography, Figure 1B; 20 mm in 3D mapping, Figure 2A) of the mitral isthmus may have facilitated this unexpected outcome. The durability of the lesion formation in the LIPV and the unintentional mitral isthmus block line remains uncertain, as neither AF nor atrial tachycardia has recurred, and no repeat ablation procedure has been undertaken.
This case highlights the importance of careful attention to catheter–sheath alignment and anatomical orientation during PFA applications at the LIPV to prevent unintentional mitral isthmus lesion formation—a phenomenon that cannot occur with PVI performed using radiofrequency ablation.
Ethics Statement
This research was conducted according to the principles of the Declaration of Helsinki.
Consent
The patient provided written informed consent for publication of the details of her case.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Video S1: Left atrial angiography performed with a pigtail catheter during right ventricular burst pacing (anteroposterior view).
Video S2: Left atrial angiography performed with a pigtail catheter during right ventricular burst pacing (left anterior oblique view).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. Y. Reddy , P. Neuzil , J. S. Koruth , et al., “Pulsed Field Ablation for Pulmonary Vein Isolation in Atrial Fibrillation,” Journal of the American College of Cardiology 74 (2019): 315–326, 10.1016/j.jacc.2019.04.021.31085321 · doi ↗ · pubmed ↗
- 2V. Y. Reddy , A. Anic , J. Koruth , et al., “Pulsed Field Ablation in Patients With Persistent Atrial Fibrillation,” Journal of the American College of Cardiology 76 (2020): 1068–1080, 10.1016/j.jacc.2020.07.007.32854842 · doi ↗ · pubmed ↗
- 3B. Davong , R. Adeliño , H. Delasnerie , et al., “Pulsed‐Field Ablation on Mitral Isthmus in Persistent Atrial Fibrillation: Preliminary Data on Efficacy and Safety,” JACC Clinical Electrophysiology 9 (2023): 1070–1081, 10.1016/j.jacep.2023.03.021.37354173 · doi ↗ · pubmed ↗