Urinary carbonic anhydrase 1 as a marker of hematuria in IgA nephropathy
Tomas G J M Post, Nils Rother, Elmar Pieterse, Ilse M Rood, Luuk B Hilbrands, Jonathan Barratt, Raphaël Duivenvoorden

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
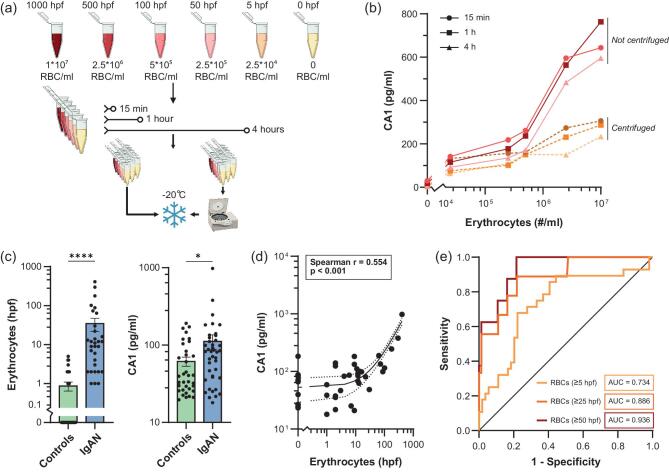 Figure 1
Figure 1- —Dutch Kidney Foundation10.13039/501100002997
- —Radboudfonds
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoagulation, Bradykinin, Polyphosphates, and Angioedema · Bipolar Disorder and Treatment · Enzyme function and inhibition
To the Editor,
In immunoglobulin A nephropathy (IgAN) hematuria is a risk factor for the development of kidney failure and a decrease in hematuria is associated with improved kidney survival [1]. Hematuria can be quantified by (automated) conventional bright field microscopy of the urinary sediment. However, because erythrocytes lyse rapidly in urine, it is difficult to reliably measure hematuria in urine samples that are collected and centrally stored in large multicenter studies. As a result, treatment effects on hematuria are often not reported in clinical trials. Additionally, it has been reported that automated microscopic analysis underestimates the severity of hematuria in kidney diseases [2–4]. Therefore, there is a need for a quantitative marker of hematuria that can be measured in a standardized manner in stored urine samples. We investigated whether carbonic anhydrase 1 (CA1) is a useful marker of hematuria that can serve as an alternative to microscopic erythrocyte quantification in urine. Carbonic anhydrases (CA) are zinc-metallo enzymes, responsible for catalyzing the reversible hydration of carbon dioxide, of which 12 isoforms exist. CA1 is primarily located in the cytosol of red blood cells and is the most abundant protein in erythrocytes, besides hemoglobin [5, 6].
To investigate the value of CA1 as a marker of hematuria, we first performed an in vitro experiment using blood and urine from a healthy subject (Fig. 1a; for full methods see Supplementary Material). Erythrocytes were isolated and diluted in clean urine to concentrations reflecting the clinically observable range of 5–1000 erythrocytes per high-power field (hpf) in the urine sediment. Samples were left at room temperature for different periods of time, and part of the urine was centrifuged prior to freezing. After thawing the urine samples the CA1 concentration was determined using an enzyme-linked immunosorbent assay (ELISA). We found a logarithmic relationship between the concentration of CA1 and the number of erythrocytes added to the urine (Fig. 1b). After centrifugation, low levels of CA1 could still be measured, most likely due to lysis of erythrocytes prior to centrifugation. The CA1 levels after centrifugation also had a logarithmic relationship with the number of added erythrocytes. After demonstrating that urine CA1 levels correlated with urine erythrocyte numbers, we investigated the correlation between urine CA1 levels and hematuria as quantified by automated microscopy of urinary sediments in a cohort of 41 IgAN patients from the Radboudumc in Nijmegen, the Netherlands, and 35 healthy controls. Patients had a mean age of 39 years [standard deviation (SD) 14.5 years], a mean body mass index (BMI) of 24.9 kg/m^2^ (SD 4.2 kg/m^2^), a mean estimated glomerular filtration rate (eGFR) of 59.9 mL/min/1.73 m^2^ (SD 26.6 mL/min/1.73 m^2^) and a mean protein/creatinine ratio of 1.04 mg/mg (SD 0.93 mg/mg), 30% were female, 90% were treated with renin–angiotensin–aldosterone system (RAAS) inhibitors and none had previously been treated with immunosuppressive medication. Erythrocyte counts in the urinary sediment, determined by automated microscopy, and CA1 levels in the urine were higher in IgAN patients than in the healthy controls (Fig. 1c). In a multivariate linear regression analysis with backward elimination we found no association between the urinary CA1 level and age, BMI, eGFR, proteinuria, sex or RAAS inhibitor use. We found no association between the MEST-C scores and erythrocyte count or urinary CA1 level in a subgroup of 10 patients that had a kidney biopsy within 3 years before study inclusion. The urinary CA1 levels showed a high correlation with erythrocyte counts, with a Spearman's rho of 0.459 (P < .001; Fig. 1d) and an interclass correlation coefficient of 0.702. CA1 levels and erythrocyte counts showed the strongest correlation in urine sediments with >25 erythrocytes per high-power field (hpf). The weaker correlation between CA1 levels and erythrocyte counts in urine sediments with <25 erythrocytes per hpf could be the result of the decreased reliability of automated microscopy analysis at lower levels of hematuria [2]. Multivariable regression analysis showed that the number of erythrocytes determines CA1 levels (P < .001) independent of the protein concentration in the urine (g/L), kidney function (eGFR Chronic Kidney Disease Epidemiology Collaboration, mL/min/1.73 m^2^), age and sex (Supplementary data, Table S1). To investigate urinary CA1’s capacity to identify IgAN patients with hematuria (erythrocytes >5/hpf), we performed a receiver operating characteristic (ROC) curve analysis, yielding an area under the curve (AUC) of 0.734 (Fig. 1e). Discriminative performance further improved for identification of IgAN patients with erythrocytes >25/hpf (AUC of 0.886) and erythrocytes >50/hpf (AUC of 0.936), which are erythrocyte counts that are usually observed in patients with active IgAN.
Our data reveal urinary CA1 as a biomarker for hematuria, which warrants further investigation in other IgAN patient cohorts for validation. Our data demonstrate that urinary CA1 can be used as a marker of hematuria. No reliable assays currently exist to determine hematuria in stored urine samples, as erythrocytes lyse rapidly in urine, and average hemoglobin dipsticks provide only qualitative information on hematuria. The commercially available CA1 ELISA assay is a test that can be performed in a standardized manner and offers the ability to estimate hematuria from frozen stored urine samples, and is independent of age, sex, proteinuria and kidney function. Our data suggest that the use of CA1 as a biomarker for hematuria can enable centralized assessment of pharmacologic effects on hematuria through the analysis of frozen urine samples from patients with IgAN (and possibly other glomerular diseases), collected in multicenter clinical trials.
Supplementary Material
gfaf133_Supplemental_File
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sevillano AM, Gutiérrez E, Yuste C et al. Remission of hematuria improves renal survival in Ig A nephropathy. J Am Soc Nephrol 2017;28:3089–99. 10.1681/ASN.201701010828592423 PMC 5619972 · doi ↗ · pubmed ↗
- 2Yang WS. Automated urine sediment analyzers underestimate the severity of hematuria in glomerular diseases. Sci Rep 2021;11:20981. 10.1038/s 41598-021-00457-634697364 PMC 8546052 · doi ↗ · pubmed ↗
- 3Wesarachkitti B, Khejonnit V, Pratumvinit B et al. Performance evaluation and comparison of the fully automated urinalysis analyzers UX-2000 and Cobas 6500. Lab Med 2016;47:124–33. 10.1093/labmed/lmw 00227069030 · doi ↗ · pubmed ↗
- 4Tantisaranon P, Dumkengkhachornwong K, Aiadsakun P et al. A comparison of automated urine analyzers cobas 6500, UN 3000-111b and i RICELL 3000 with manual microscopic urinalysis. Pract Lab Med 2021;24:e 00203. 10.1016/j.plabm.2021.e 0020333553552 PMC 7847969 · doi ↗ · pubmed ↗
- 5Villeval J, Testa U, Vinci G et al. Carbonic anhydrase I is an early specific marker of normal human erythroid differentiation. Blood 1985;66:1162–70. 10.1182/blood.V 66.5.1162.11623931725 · doi ↗ · pubmed ↗
- 6Purkerson JM, Schwartz GJ. The role of carbonic anhydrases in renal physiology. Kidney Int 2007;71:103–15. 10.1038/sj.ki.500202017164835 · doi ↗ · pubmed ↗