Comparative validation of automated perfusion analysis software for ischemic penumbra estimation and EVT decision-making
Jonguk Kim, Jong-Hyeok Park, Dongmin Kim, Myungjae Lee, Joon-Tae Kim, Leonard Sunwoo, Cheolkyu Jung, Wi-Sun Ryu, Beom Joon Kim

TL;DR
This study compares two software tools for analyzing brain perfusion in stroke patients and finds them highly consistent in estimating ischemic areas and treatment decisions.
Contribution
The study is the first to systematically compare automated PWI analysis platforms in acute stroke care.
Findings
JLK PWI showed excellent agreement with RAPID for ischemic core and hypoperfused volume measurements.
EVT eligibility classifications using DAWN criteria showed very high concordance between the two platforms.
The results support JLK PWI as a reliable alternative to RAPID in MRI-based perfusion analysis.
Abstract
While computed tomography perfusion is widely used in acute stroke imaging, magnetic resonance perfusion-weighted imaging (PWI) offers superior spatial resolution and tissue specificity, particularly when combined with diffusion-weighted imaging (DWI). However, no prior study has systematically compared automated PWI analysis platforms. This study aims to evaluate the performance of a newly developed software (JLK PWI) against the established RAPID platform in terms of volumetric agreement and clinical decision concordance. This retrospective multicenter study included 299 patients with acute ischemic stroke who underwent PWI within 24 h of symptom onset. Volumetric agreement between RAPID and JLK PWI was assessed using concordance correlation coefficients (CCC), Bland–Altman plots, and Pearson correlations. Agreement in endovascular therapy (EVT) eligibility was evaluated using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
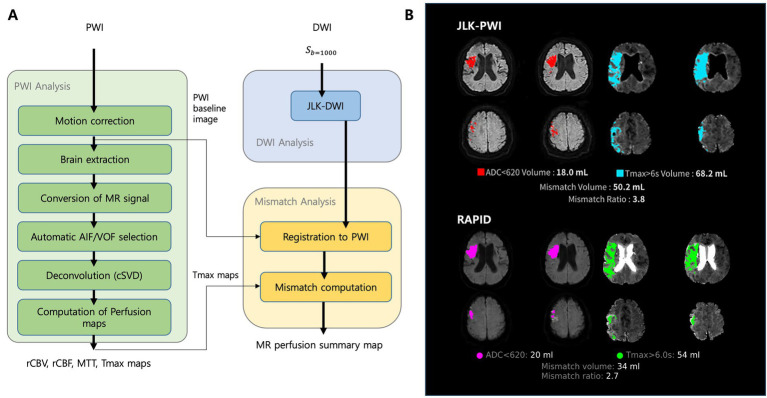 Figure 1
Figure 1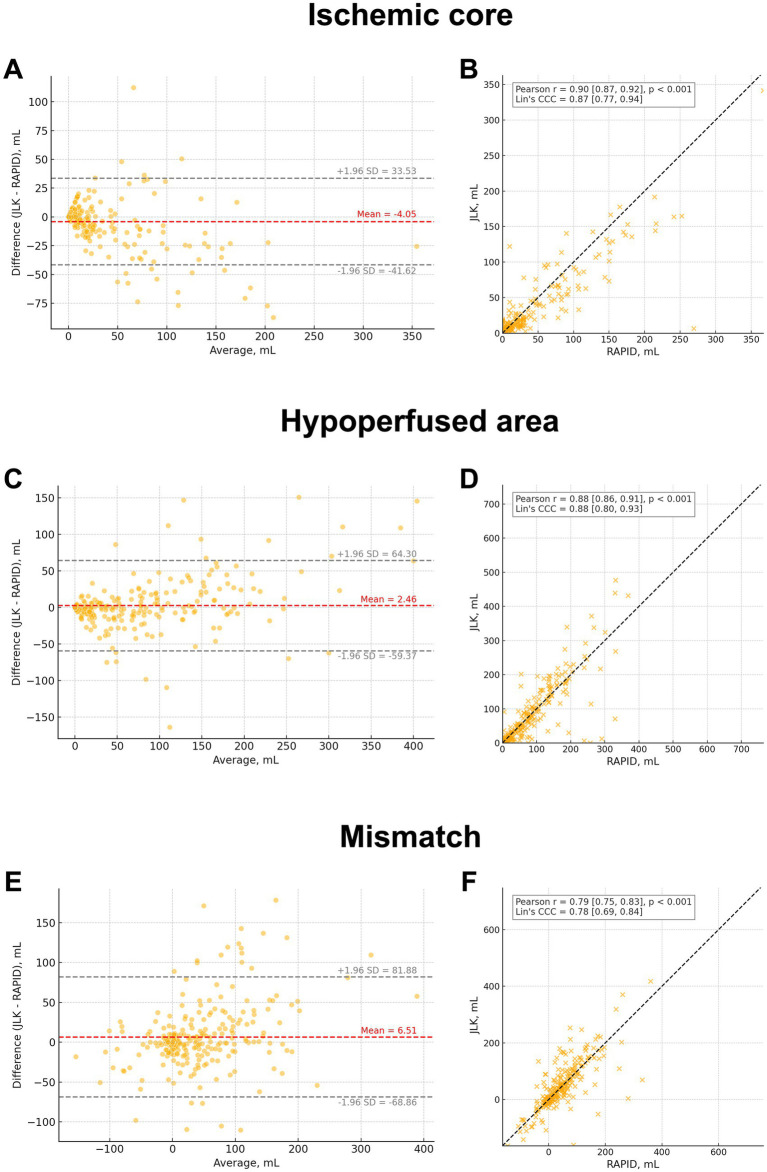 Figure 2
Figure 2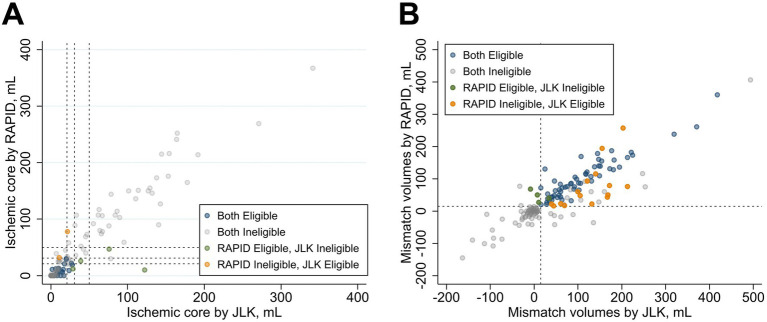 Figure 3
Figure 3| Variables | Values ( |
|---|---|
| Age, year | 70.9 ± 11.6 |
| Male | 167 (55.9%) |
| Initial NIHSS score, IQR | 11 [5–17] |
| Pre-stroke mRS ≤ 2 | 244 (81.6%) |
| Hypertension | 197 (65.9%) |
| Diabetes | 90 (30.1%) |
| Hyperlipidemia | 118 (39.5%) |
| Smoking | 79 (26.4%) |
| Atrial fibrillation | 131 (43.8%) |
| Stroke subtype | |
| Large artery atherosclerosis | 87 (29.1%) |
| Cardioembolism | 135 (45.2%) |
| Small vessel occlusion | 25 (8.4%) |
| Undetermined | 39 (13.0%) |
| Other determined | 13 (4.4%) |
| MR manufacturer | |
| GE | 102 (34.1%) |
| Siemens | 17 (5.7%) |
| Philips | 180 (60.2%) |
| Magnetic field strength, T | |
| 1.5 | 117 (39.1%) |
| 3 | 182 (60.9%) |
| Intravenous thrombolysis | 157 (52.5%) |
| Endovascular thrombectomy | 214 (71.6%) |
| Occlusion site | |
| Anterior circulation large vessel occlusion | 208 (69.6%) |
| Basilar artery occlusion | 31 (10.4%) |
| No large vessel occlusion | 60 (20.1%) |
| Time indices | |
| Last known well to PWI, min | 360 [216–750] |
| PWI to puncture, min ( | 55.5 [40.8–82.3] |
| Trial criteria | RAPID | JLK PWI | Cohen’s kappa (95% CI) | ||
|---|---|---|---|---|---|
| Not eligible | Eligible | ||||
| DAWN | All ( | Not eligible | 88 | 2 | 0.873 (0.773 to 0.973) |
| Eligible | 4 | 29 | |||
| Age >80 and NIHSS score ≥10 ( | Not eligible | 28 | 0 | 0.841 (0.620 to 1.000) | |
| Eligible | 2 | 7 | |||
| Age ≤80 and NIHSS score 10–19 ( | Not eligible | 55 | 2 | 0.897 (0.779 to 1.000) | |
| Eligible | 1 | 18 | |||
| Age ≤80 and NIHSS score ≥20 ( | Not eligible | 5 | 0 | 0.800 (0.357 to 1.000) | |
| Eligible | 1 | 4 | |||
| DEFUSE 3 ( | Not eligible | 86 | 15 | 0.761 (0.660 to 0.862) | |
| Eligible | 4 | 58 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Ischemic Stroke Management · Advanced MRI Techniques and Applications · Cardiac Imaging and Diagnostics
Introduction
The advent of automated perfusion imaging analysis has significantly improved the triage of patients with acute ischemic stroke, particularly by extending the treatment window for endovascular therapy (Albers et al., 2018; Nogueira et al., 2018). Computed tomography perfusion (CTP) has become the predominant modality in emergency settings due to its rapid acquisition and broad accessibility (Kim et al., 2024b). As a result, many studies have compared CTP-based software platforms in terms of infarct core estimation, perfusion mismatch, and outcome prediction (Xiong et al., 2019; Suomalainen et al., 2022; Kim et al., 2024a).
In contrast, magnetic resonance perfusion-weighted imaging (PWI) has received less attention in the context of automated analysis. Previous studies have compared commercial PWI platforms to manual reference or reported differences between platforms (Galinovic et al., 2012; Chatterjee et al., 2015; Deutschmann et al., 2021; Xiong et al., 2022; Teichmann et al., 2025). However, these studies were generally limited by modest sample sizes, single-center designs, or the absence of direct comparative evaluations with RAPID across diverse stroke populations and clinical decision-making frameworks. This gap has hindered efforts to standardize MRI-based stroke workflows, despite their growing clinical applications.
PWI offers several technical advantages over CTP. It provides higher spatial resolution, is free from beam-hardening artifacts, and is less susceptible to contrast timing errors (Konstas et al., 2009; Liu et al., 2024). These features improve image quality, particularly in challenging regions such as the posterior fossa or in patients with small vessel disease. Additionally, when paired with DWI, PWI enables more accurate delineation of infarct core and penumbra (Kane et al., 2007), and avoids the risk of ionizing radiation exposure (Cohnen et al., 2006), making it suitable for selected patient populations and research contexts.
Recent clinical trials (Mohammaden et al., 2024; Goyal et al., 2025; Psychogios et al., 2025) targeting medium vessel occlusion (MeVO) have underscored the need for more refined imaging biomarkers to better identify patients who may benefit from treatment (Ospel et al., 2024; Salim et al., 2024; Cai et al., 2025). The combined spatial precision and tissue specificity of PWI-DWI may enhance patient stratification and inform more personalized treatment strategies.
In this study, we introduce a newly developed PWI analysis platform (JLK PWI, JLK Inc., Republic of Korea) and compare its performance with that of a widely used commercial software (RAPID, RAPID AI, CA, USA). We evaluate inter-platform agreement in volumetric parameters, including ischemic core, hypoperfused area, and mismatch volume, as well as in treatment eligibility based on DAWN and DEFUSE-3 trial criteria (Albers et al., 2018; Nogueira et al., 2018). This study aims to evaluate the clinical viability of JLK PWI as a robust alternative for MRI-based stroke assessment.
Methods
Study design and study population
This retrospective multicenter study included patients with acute ischemic stroke who underwent PWI within 24 h of symptom onset at two tertiary hospitals in Korea. A total of 216 patients from Seoul National University Bundang Hospital who underwent both PWI and endovascular thrombectomy between January 2019 and April 2024, and 102 patients from Chonnam National University Hospital who underwent PWI within 24 h of symptom onset with or without endovascular thrombectomy (EVT) between January 2015 and December 2015, were initially screened. After pooling the datasets, 318 patients met the inclusion criteria. Of these, patients were excluded due to abnormal arterial input function (n = 6), severe motion artifacts (n = 2), or inadequate images (n = 11). Consequently, 299 patients were included in the final analysis. The study protocol was approved by the institutional review board of Seoul National University Bundang Hospital [IRB# B-1710-429-102], and written informed consent was obtained from all patients or their legal representatives.
Clinical data collection
Using a standardized protocol (Kim et al., 2014), we prospectively collected demographic data, vascular risk factors (hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, atrial fibrillation, and smoking history), prior medication use, pre-stroke functional status, and index stroke characteristics, such as initial stroke severity (NIH Stroke Scale, NIHSS) and subtypes. Stroke subtypes were determined by an experienced vascular neurologist, using a validated MRI-based classification system built on the TOAST (Trial of ORG 10172 in Acute Stroke Treatment) criteria (Ko et al., 2014).
Imaging and image reconstruction
All perfusion MRI scans were performed on either 3.0 T (62.3%) or 1.5 T (37.7%) scanners. Regarding the vendors, 34.1% of scans were conducted using GE systems, 60.2% using Philips systems, and 5.7% using Siemens systems, all equipped with an 8-channel head coil. Dynamic susceptibility contrast-enhanced perfusion imaging was performed using a gradient-echo echo-planar imaging (GE-EPI) sequence. The imaging parameters were as follows: repetition time (TR) = 1,000–1,500 ms (6.3%), 1,500–2,000 ms (66.7%), or 2,000–2,500 ms (27.0%); echo time (TE) = 30–40 ms (1.0%), 40–50 ms (91.8%), or 60–70 ms (7.2%); field of view (FOV) = 210 × 210 mm^2^ (5.7%), or 230 × 230 mm^2^ (94.3%); and slice thickness of 5 mm with no interslice gap, covering the entire supratentorial brain with 17–25 slices. Images were reconstructed and exported in DICOM format for subsequent post-processing and quantitative perfusion analysis. To minimize inter-scanner variability, all datasets underwent standardized preprocessing and normalization prior to PWI mapping. All image analyses were done in the central image laboratory operated by Seoul National University Bundang Hospital.
Automated PWI analysis
For infarct core estimation, RAPID employed the default threshold of ADC < 620 × 10^−6^ mm^2^/s. JLK PWI utilized a deep learning–based infarct segmentation algorithm applied to the b1000 DWI images, which was developed and validated in previous studies using large manually segmented datasets (Ryu et al., 2023, 2024, 2025).
As illustrated in Figure 1A, JLK PWI performs automated preprocessing and perfusion parameter calculations through a multi-step pipeline. The workflow includes motion correction to acquisition artifacts, brain extraction by skull stripping and vessel masking, and conversion of MR signal. The software automatically selects the arterial input function and venous output function, followed by block-circulant single value deconvolution and calculation of quantitative perfusion maps, including CBF, CBV, MTT, and Tmax.
Two-panel figure showing MR perfusion workflow and example outputs. Panel A shows schematic pipeline for perfusion processing. Panel B represents a representative patient showing co-registered diffusion and perfusion maps with color overlays; ischemic core and hypoperfused tissue are quantified (mL) and mismatch ratio is displayed.
The infarct core from JLK-DWI is automatically co-registered to the perfusion maps, allowing mismatch computation between diffusion and perfusion lesions. The hypoperfused region was delineated using the threshold of Tmax >6 s. All segmentations and resulting images were visually inspected to ensure technical adequacy before inclusion in the analysis. Figure 1B presents a representative case comparing infarct core and hypoperfusion segmentation between JLK PWI and RAPID.
Statistical analysis
Descriptive statistics were used to summarize baseline characteristics. Continuous variables were reported as means with standard deviations (SD) or medians with interquartile ranges (IQR), depending on data distribution. Categorical variables were presented as counts with percentages. Agreement between the two platforms in perfusion parameter measurements (ischemic core volume, hypoperfused volume, and mismatch volume) was assessed using concordance correlation coefficients (CCC), Pearson correlation coefficients, and Bland–Altman plots. The magnitude of agreement was classified as: poor (0.0–0.2), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), and excellent (0.81–1.0) (Landis and Koch, 1977).
For EVT eligibility, classification agreement between the RAPID and JLK software was evaluated using Cohen’s kappa coefficient, applied separately for each subgroup defined by the DAWN and DEFUSE-3 trial criteria. The DAWN classification stratified eligible infarct volume based on age and NIHSS into three prespecified categories, while the DEFUSE-3 classification used a mismatch ratio ≥1.8, an infarct core volume <70 mL and an absolute volume of penumbra ≥15 mL. Cases with discordant EVT eligibility classifications were additionally analyzed descriptively.
Subgroup analyses were conducted for patients with anterior circulation large vessel occlusion (including internal carotid artery, middle cerebral artery M1-M2 branches, and anterior cerebral artery) and those with basilar artery occlusion. In each subgroup, agreement metrics and outcome prediction models were separately generated to evaluate software performance across stroke types. Additional analyses stratified by MRI vendor and field strength were conducted to assess the consistency of agreement across acquisition settings.
All statistical analyses were performed using STATA version 16.0 (StataCorp LLC, College Station, TX) and R version 4.2.3 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value < 0.05 was considered statistically significant.
Subject characteristics
For 299 subjects included, the mean age was 70.9 years (SD 11.6), and 55.9% were male. The median NIHSS score on admission was 11 (IQR: 5–17). The most common stroke subtype was cardioembolism (45.2%), followed by large artery atherosclerosis (29.1%) and undetermined etiology (13.0%). Intravenous thrombolysis was administered in 157 patients (52.5%).
Regarding occlusion sites, 208 (69.6%) subjects had anterior circulation large vessel occlusion, and 31 had basilar artery occlusion (10.4%). Meanwhile, 60 (20.1%) subjects had no large vessel occlusion on MRI. The median time from the last known well to PWI was 360 min (IQR: 216–750) min, and the median time from PWI to groin puncture was 55.5 min (IQR: 40.8–82.3).
Results
Concordance of ischemic core, hypoperfused, and mismatch volumes
Ischemic core volumes showed high agreement between RAPID and JLK PWI, with CCC = 0.87 (95% CI, 0.77–0.94; Figure 2B). The Bland–Altman plot showed a mean difference of −4.05 mL and limits of agreement ranging from −41.62 to 33.53 mL (Figure 2A). Similarly, hypoperfused volumes showed high agreement (CCC = 0.88 [95% CI, 0.80–0.93]; Figure 2D). The mean difference was 2.46 mL, with limits of agreement from −59.37 to 64.30 mL (Figure 2C). Mismatch volumes demonstrated substantial agreement (CCC = 0.78 [95% CI, 0.69–0.84]; Figure 2F), with a mean difference of 6.51 mL and limits of agreement from −68.86 to 81.88 mL (Figure 2E). Overall concordance was good, although relatively large volumetric discrepancies were observed in some subjects, as reflected in the wide limits of agreement (see Table 1).
Agreement between JLK and RAPID perfusion outputs. Bland-Altman plots (A, C, E) show differences versus means for ischemic core, hypoperfused volume, and mismatch; central mean line and ±1.96 SD limits are drawn. Scatter plots (B, D, F) show correlations with linear fits; Pearson’s r and Lin’s concordance correlation coefficient (CCC) are reported. The panels summarize bias, limits of agreement, and strength of association across metrics, demonstrating high concordance for core and clinically meaningful agreement for hypoperfusion and mismatch.
Subgroup analyses for patients with anterior circulation large vessel occlusion (Supplementary Figure 1) and basilar artery occlusion (Supplementary Figure 2) showed similar trends in agreement across core, hypoperfusion, and mismatch volumes. In the basilar artery occlusion group (n = 31), ischemic core volumes demonstrated high agreement between RAPID and JLK PWI (CCC = 0.95 [95% CI, 0.88–0.97]), whereas hypoperfusion volumes showed moderate agreement with CCC = 0.55 (95% CI, 0.31–0.81).
Additional subgroup analyses by different field strengths and MRI vendors demonstrated consistently high concordance across scanner types, with comparable CCC values for ischemic core, hypoperfused, and mismatch volumes (Supplementary Figures 3–7).
Concordance of EVT eligibility based on DAWN and DEFUSE-3 criteria
To assess the concordance in determining eligibility for EVT, we applied the strict inclusion criteria from the DAWN and DEFUSE-3 trials to the relevant subgroups within our patient cohort. For the DAWN trial criteria, the analysis included 123 patients with an anterior circulation large vessel occlusion and an initial NIHSS score of 10 or higher. In this subgroup, the agreement between RAPID and JLK PWI was excellent (Cohen’s κ = 0.873; 95% CI, 0.773–0.973; Table 2, Figure 3A).
Outcome of selection criteria using RAPID versus JLK. Panel A compares ischemic core volumes (mL); Panel B compares mismatch volumes (mL). Points are colored by eligibility: both eligible (blue), both ineligible (gray), RAPID-only eligible (green), and JLK-only eligible (orange).
For the DEFUSE-3 trial criteria, the analysis included 163 patients with an anterior circulation large vessel occlusion and an initial NIHSS score of 6 or higher. The agreement between the platforms was substantial (Cohen’s κ = 0.761; 95% CI, 0.660–0.862). Both platforms concordantly identified 58 patients as eligible and 86 as ineligible. There were 19 discordant cases, with 15 deemed eligible by JLK PWI only and 4 by RAPID only (Table 2, Figure 3B). A detailed breakdown of the discordant classifications for DEFUSE-3 is provided in Supplementary Table 1. For the 15 patients deemed eligible only by JLK PWI, the most common reason for ineligibility by RAPID was an ischemic core volume >70 mL (13 of 15 cases). For the four patients deemed eligible only by RAPID, the primary reasons for ineligibility by JLK PWI were a mismatch volume <15 mL (3 of 4 cases) and a mismatch ratio <1.8 (1 of 4 cases).
Discussion
To our knowledge, this study is among the first to conduct a comprehensive validation of a newly developed MRI perfusion software (JLK PWI) against the established RAPID platform, using both volumetric and clinical decision-making metrics. Importantly, our analysis is not limited to core–hypoperfusion volume comparisons but also includes EVT triage concordance based on DAWN and DEFUSE-3 criteria, as well as volumetric concordance of infarct core estimation between JLK PWI and diffusion-restricted lesions defined by RAPID (ADC < 620). This multifaceted approach offers a pragmatic perspective for assessing real-world performance of automated perfusion software within acute stroke workflows.
A notable strength of our study lies in its inclusion of broad stroke population, encompassing both anterior and posterior circulation large vessel occlusion, and a wide spectrum of imaging time windows up to 24 h. Most prior validation studies have focused on CTP-derived perfusion maps or DWI-based core estimation alone (Austein et al., 2016; Suomalainen et al., 2022). By leveraging PWI-DWI integration in a clinical setting, we demonstrate that the JLK PWI achieves excellent volumetric agreement with RAPID (CCC = 0.87) and high agreement in EVT decision-making (Cohen’s κ up to 0.90 for DAWN). These results support the use of JLK PWI not only as a technical substitute, but also as a clinical decision-making tool (Neumann-Haefelin et al., 1999; Mishra et al., 2025).
Accurate, automated estimation of infarct core is critical for patient selection in reperfusion therapies, particularly in extended time windows and in settings where CTP is unavailable or unsuitable (Evans et al., 2018; Mishra et al., 2025). Our findings show that JLK PWI maintains high fidelity in infarct core and hypoperfusion volume estimation across diverse patient profiles. Notably, EVT eligibility classifications showed high concordance between the two platforms, with 95% agreement for DAWN (κ = 0.873) and 88% agreement for DEFUSE-3 (κ = 0.761). These findings suggest that JLK PWI can be effective in guideline-based treatment decisions.
It is noteworthy that the agreement rate for DAWN criteria is substantially higher than that for DEFUSE-3. A plausible explanation is that JLK PWI showed more consistent performance in estimating the infarct core on DWI, which is central to the clinical-DWI mismatch approach underlying DAWN. In contrast, DEFUSE-3 additionally incorporates hypoperfusion and mismatch volumes from PWI, where greater variability was observed between the two platforms. This variability may be related to differences in imaging characteristics. DWI provides higher spatial resolution and more reliable lesion delineation, whereas PWI is more sensitive to contrast timing and post-processing (Demeestere et al., 2020). Also, variation in hypoperfusion segmentation algorithms across platforms may contribute. These findings suggest that PWI-based mismatch measurements should be interpreted with caution when applied in clinical decision-making.
Furthermore, JLK PWI software demonstrated good agreement for ischemic core estimation and reasonable agreement for hypoperfusion volumes even in posterior circulation strokes, where perfusion analysis remains technically challenging (Pallesen et al., 2018). While the number of patients with basilar artery occlusion in our cohort was limited, these findings suggest its potential utility in future studies and clinical protocols involving basilar occlusions or MeVOs, which are increasingly recognized as important therapeutic targets despite the current lack of standardized imaging criteria (Cimflova et al., 2021; Alemseged et al., 2023).
Some limitations must be acknowledged. First, the generalizability of our findings may be limited by the retrospective design and the inclusion of two tertiary stroke centers. Second, MRI scans were acquired using both 3.0 T and 1.5 T systems from different vendors, and heterogeneity in acquisition parameters and contrast timing may influence software outputs. Third, we did not include specific imaging data such as infarct growth or collateral status (de Havenon et al., 2019), which could provide additional context for discrepancies in EVT decision classification.
Future studies should prospectively validate JLK PWI in broader clinical settings, including underrepresented stroke populations such as MeVOs and wake-up strokes. Integration of additional imaging biomarkers, such as collateral grading (Tetteh et al., 2023), or radiomic texture features (Li et al., 2024), may further enhance prediction models and assist in complex clinical decisions. In addition, longitudinal studies examining infarct evolution and clinical outcomes after EVT could provide insight into the long-term predictive validity of automated core estimation tools like JLK PWI.
Conclusion
In conclusion, JLK PWI demonstrates excellent technical and clinical agreement with established commercial software, offering reliable infarct core estimation and high concordance in EVT decision-making. Its applicability across diverse stroke types and its foundation in deep learning–based analysis position it as a promising tool for real-time stroke triage. As imaging-based selection becomes increasingly nuanced, JLK PWI may play a critical role in improving access to individualized, time-sensitive reperfusion therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Albers G. W.Marks M. P.Kemp S.Christensen S.Tsai J. P.Ortega-Gutierrez S.. (2018). Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N. Engl. J. Med. 378, 708–718. doi: 10.1056/nejmoa 1713973, PMID: 29364767 PMC 6590673 · doi ↗ · pubmed ↗
- 2Alemseged F.Nguyen T. N.Alverne F. M.Liu X.Schonewille W. J.Nogueira R. G. (2023). Endovascular therapy for basilar artery occlusion. Stroke 54, 1127–1137. doi: 10.1161/strokeaha.122.040807, PMID: 36722343 · doi ↗ · pubmed ↗
- 3Austein F.Riedel C.Kerby T.Meyne J.Binder A.Lindner T.. (2016). Comparison of perfusion CT software to predict the final infarct volume after thrombectomy. Stroke 47, 2311–2317. doi: 10.1161/strokeaha.116.013147, PMID: 27507864 · doi ↗ · pubmed ↗
- 4Cai L. Y.Hoseinyazdi M.Lakhani D. A.Salim H.Mei J.Dmytriw A. A.. (2025). Redefining ischemic core, penumbra, and target mismatch on perfusion imaging in acute anterior distal medium vessel occlusion. Stroke Vasc. Interv. Neurol. doi: 10.1161/svin.125.001900 · doi ↗
- 5Chatterjee N. R.Ansari S. A.Vakil P.Prabhakaran S.Carroll T. J.Hurley M. C. (2015). Automated analysis of perfusion weighted MRI using asymmetry in vascular territories. Magn. Reson. Imaging 33, 618–623. doi: 10.1016/j.mri.2015.01.009, PMID: 25601529 PMC 4426216 · doi ↗ · pubmed ↗
- 6Cimflova P.Mc Donough R.Kappelhof M.Singh N.Kashani N.Ospel J. M.. (2021). Perceived limits of endovascular treatment for secondary medium-vessel-occlusion stroke. Am. J. Neuroradiol. 42, 2188–2193. doi: 10.3174/ajnr.a 7327, PMID: 34711552 PMC 8805763 · doi ↗ · pubmed ↗
- 7Cohnen M.Wittsack H.-J.Assadi S.Muskalla K.Ringelstein A.Poll L. W.. (2006). Radiation exposure of patients in comprehensive computed tomography of the head in acute stroke. AJNR Am. J. Neuroradiol. 27, 1741–1745.16971627 PMC 8139787 · pubmed ↗
- 8de Havenon A.Mlynash M.Kim-Tenser M. A.Lansberg M. G.Leslie-Mazwi T.Christensen S.. (2019). Results from DEFUSE 3. Stroke 50, 632–638. doi: 10.1161/strokeaha.118.023407, PMID: 30726184 PMC 6628906 · doi ↗ · pubmed ↗