Propranolol (1 mg/kg/day) with intralesional bleomycin versus propranolol monotherapy for infantile hemangioma: a randomized controlled trial
Yanyan Guo, Xinxian Liu, Sicheng He, Bin Zhou

TL;DR
Combining low-dose propranolol with bleomycin injections improves treatment outcomes for infantile hemangioma compared to propranolol alone.
Contribution
Demonstrates that adding bleomycin to low-dose propranolol enhances efficacy and cosmetic results for infantile hemangioma.
Findings
Combination therapy achieved a 77.69% excellent response rate versus 50.00% with monotherapy after 6 months.
Combination therapy showed faster tumor atrophy and better tumor volume reduction compared to monotherapy.
Combination therapy resulted in significantly lower scarring scores and improved cosmetic outcomes.
Abstract
To evaluate the efficacy and safety of oral propranolol (1 mg/kg/day) combined with intralesional bleomycin injections versus propranolol monotherapy at the same dosage for infantile hemangioma (IH). This study investigates if a low-dose propranolol regimen can be enhanced with local therapy to improve outcomes while maintaining a favorable safety profile. This single-center, prospective, randomized controlled trial enrolled 260 infants (aged 3–11 months, mean age 5.34 ± 2.57 months) with IH requiring systemic therapy. Participants were randomly assigned (1:1) to either the combination group (propranolol plus monthly intralesional bleomycin, n = 130) or the monotherapy group (propranolol alone, n = 130). The primary efficacy endpoint was the proportion of patients achieving an excellent therapeutic response (complete regression or marked effectiveness) at 6 months. Secondary outcomes…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
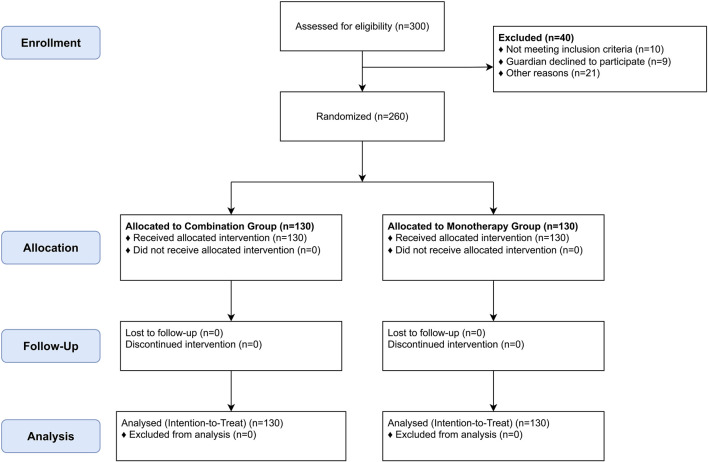 FIGURE 1
FIGURE 1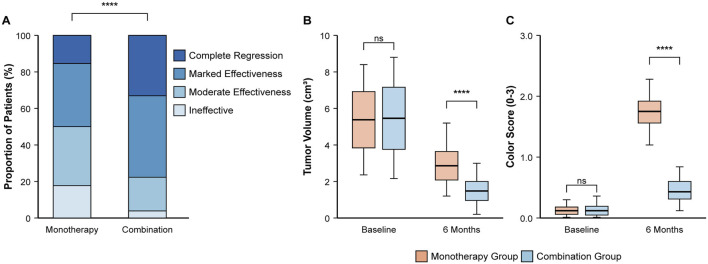 FIGURE 2
FIGURE 2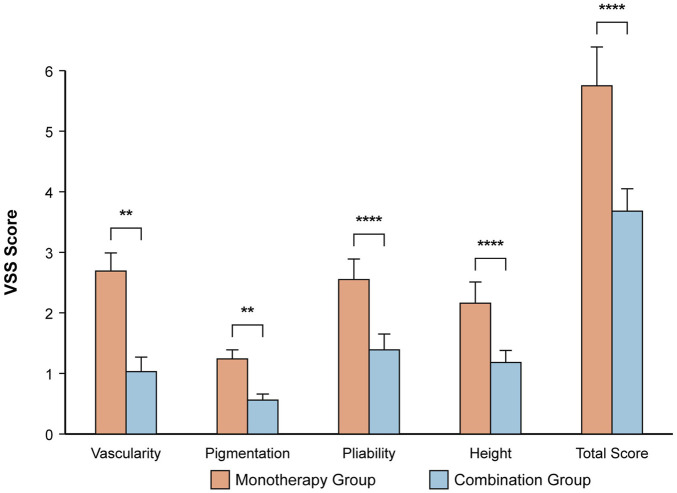 FIGURE 3
FIGURE 3| Reason for exclusion | Number of patients (n) | Percentage (%) |
|---|---|---|
| Did not meet inclusion criteria | 10 | 25.0% |
| - Age outside of 3–11 months range | 6 | |
| - Prior treatment received | 4 | |
| Guardian declined to participate | 9 | 22.5% |
| Other reasons | 21 | 52.5% |
| - Presence of significant comorbidity (e.g., cardiac) | 8 | |
| - Logistical issues (e.g., family lived too far away) | 7 | |
| - Failed cardiac screening | 6 | |
| Total Excluded | 40 | 100% |
| Characteristic | Monotherapy group (n = 130) | Combination group (n = 130) | Test statistic (t/χ2) | P-value |
|---|---|---|---|---|
| Age (months), mean ± SD | 5.16 ± 2.33 | 5.49 ± 3.07 | 1.005 (t) | 0.316 |
| Sex (Male: Female), n | 62:68 | 60:70 | 0.097 (χ2) | 0.755 |
| Tumor site, n (%) | ||||
| Head and Neck | 78 (60.00%) | 82 (63.07%) | 0.269 (χ2) | 0.604 |
| Trunk | 32 (24.61%) | 35 (26.92%) | 0.234 (χ2) | 0.629 |
| Limbs | 20 (15.39%) | 13 (10.00%) | 2.273 (χ2) | 0.132 |
| Outcome category | Monotherapy group (n = 130) | Combination group (n = 130) | χ2 value | P-value |
|---|---|---|---|---|
| Complete Regression, n (%) | 20 (15.38%) | 43 (33.07%) | 10.783 | 0.001 |
| Marked Effectiveness, n (%) | 45 (34.61%) | 58 (44.61%) | 2.997 | 0.083 |
| Moderate Effectiveness, n (%) | 42 (32.31%) | 24 (18.46%) | 6.326 | 0.012 |
| Ineffective, n (%) | 23 (17.69%) | 5 (3.85%) | 13.031 | <0.001 |
| Excellent Response (Complete + Marked), n (%) | 65 (50.00%) | 101 (77.69%) | 21.849 | <0.001 |
| Response grade | Monotherapy group (n = 130) | Combination group (n = 130) | Overall χ2 value | Overall P-value |
|---|---|---|---|---|
| Obvious Atrophy, n (%) | 19 (14.61%) | 52 (40.00%) | 23.951 | <0.001 |
| Mild Atrophy, n (%) | 78 (60.00%) | 51 (39.23%) | ||
| No Obvious Change, n (%) | 33 (25.39%) | 27 (20.77%) | ||
| Any Response (Obvious + Mild), n (%) | 97 (74.61%) | 103 (79.23%) | 0.781 | 0.377 |
| Time point | Monotherapy group (n = 130) | Combination group (n = 130) | t-value | P-value |
|---|---|---|---|---|
| Baseline, mean ± SD | 2.50 ± 0.35 | 2.53 ± 0.44 | −0.648 | 0.518 |
| After 6 Months, mean ± SD | 1.25 ± 0.41 | 0.43 ± 0.29 | 18.412 | <0.001 |
| VSS component | Monotherapy group (n = 130) | Combination group (n = 130) | t-value | P-value |
|---|---|---|---|---|
| Vascularity, mean ± SD | 1.69 ± 0.30 | 1.03 ± 0.24 | 19.108 | <0.001 |
| Pigmentation, mean ± SD | 1.24 ± 0.15 | 0.56 ± 0.10 | 43.167 | <0.001 |
| Pliability, mean ± SD | 2.55 ± 0.34 | 1.39 ± 0.26 | 30.820 | <0.001 |
| Height, mean ± SD | 2.16 ± 0.35 | 1.18 ± 0.20 | 26.680 | <0.001 |
| Total VSS Score, mean ± SD | 5.75 ± 0.64 | 3.68 ± 0.37 | 31.841 | <0.001 |
| Adverse event | Monotherapy group (n = 130) | Combination group (n = 130) | χ2 value | P-value |
|---|---|---|---|---|
| Local Redness and Pain, n (%) | 0 (0%) | 11 (8.46%) | 11.450 | <0.001 |
| Bradycardia (transient), n (%) | 3 (2.31%) | 4 (3.08%) | 0.149 | 0.700 |
| Hypotension (mild, transient), n (%) | 0 (0%) | 1 (0.77%) | 1.004 | 0.316 |
| Hypoglycemia (mild, transient), n (%) | 0 (0%) | 2 (1.54%) | 2.016 | 0.156 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations and Hemangiomas · Vascular Malformations Diagnosis and Treatment · Congenital Ear and Nasal Anomalies
Introduction
Infantile hemangioma (IH) is the most common benign vascular tumor of infancy, affecting approximately 4%–10% of infants, with a higher prevalence in females, premature infants, and those with low birth weight (Léauté-Labrèze et al., 2017; Sharma et al., 2024). The natural history of IH typically involves a proliferative phase within the first few weeks to months of life, followed by an involution phase that can last several years (Hoeger et al., 2015). While many IHs regress spontaneously, a clinically significant proportion, estimated at 15%–20%, may not resolve completely or can lead to complications such as ulceration, bleeding, functional impairment (e.g., visual or airway obstruction), or significant disfigurement, necessitating active treatment (Lu et al., 2024; Zavras et al., 2020).
Oral propranolol, a non-selective beta-blocker, has revolutionized IH treatment and is now considered the first-line systemic therapy (Krowchuk et al., 2019; Chen et al., 2024). Its mechanisms of action include vasoconstriction, inhibition of angiogenesis (e.g., via downregulation of vascular endothelial growth factor (VEGF) pathways), and induction of endothelial cell apoptosis (Storch and Hoeger, 2010; Lee et al., 2014). While the therapeutic dose of propranolol typically ranges from 1 to 3 mg/kg/day, with 2 mg/kg/day often used for optimal efficacy (Chen et al., 2023), there is a clinical imperative to minimize systemic exposure in young infants to reduce potential adverse effects like hypoglycemia, bradycardia, hypotension, and bronchospasm (Hermans et al., 2024). This has prompted research into the efficacy of lower-dose regimens.
Intralesional bleomycin, an antineoplastic agent with sclerosing properties, has emerged as a therapeutic option for vascular malformations and refractory or complex IHs (Horbach et al., 2016; Kiani et al., 2025). Bleomycin induces endothelial cell damage and promotes local fibrosis, leading to lesion regression (Muir et al., 2004). Local injection offers targeted therapy with higher drug concentrations at the lesion site and potentially fewer systemic side effects compared to systemic administration (Kumar et al., 2021). Previous studies have suggested that combining propranolol with other modalities may enhance efficacy (Guo et al., 2024; Tiwari et al., 2022). However, robust evidence from RCTs evaluating the augmentation of a low-dose propranolol regimen with intralesional bleomycin is still limited.
We hypothesized that a synergistic effect could be achieved; propranolol’s systemic anti-angiogenic action may sensitize the proliferating endothelial cells, making them more susceptible to the potent, localized cytotoxic effects of intralesional bleomycin, thereby accelerating regression and improving final cosmetic outcomes even with a lower systemic propranolol dose. The primary objective of this study was therefore not to challenge the efficacy of standard-dose propranolol, but to determine if a low-dose regimen (1 mg/kg/day) could be significantly augmented by adjuvant intralesional bleomycin to achieve superior efficacy compared to low-dose monotherapy alone.
Methods
Study design and oversight
This study was a prospective, randomized, controlled, open-label trial with blinded outcome assessment conducted at Wuhan Children’s Hospital, China. The trial was designed and reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement (Schulz et al., 2010). The study protocol was approved by the Institutional Ethics Committee of Wuhan Children’s Hospital. All parents or legal guardians provided written informed consent.
Study participants
Infants with IH were recruited from our hospital between 1 January 2024, and 1 January 2025. All diagnoses were made clinically by two experienced dermatologists. High-frequency ultrasound was used in all cases to confirm the diagnosis, measure tumor dimensions, and rule out other underlying structures, ensuring a homogenous study population.
Inclusion Criteria: (1) age 3–11 months; (2) diagnosed IH requiring treatment (e.g., rapid growth, high-risk location, risk of functional impairment, ulceration, or significant cosmetic concern); (3) no prior treatment for IH; (4) guardians provided informed consent.
Exclusion Criteria: (1) known hypersensitivity to propranolol or bleomycin; (2) congenital or mixed hemangiomas; (3) significant cardiopulmonary, hepatic, or renal dysfunction; (4) other severe systemic diseases; (5) PHACE syndrome or major congenital anomalies.
Randomization, allocation concealment, and blinding
Eligible participants were randomly assigned (1:1) to either the combination therapy group or the propranolol monotherapy group using a computer-generated random number sequence. Allocation concealment was ensured using sequentially numbered, sealed, opaque envelopes. Due to the nature of the interventions, participants and treating physicians were not blinded. However, outcome assessors and data analysts were blinded to the treatment assignments.
Interventions
Monotherapy Group (n = 130): Participants received oral propranolol hydrochloride solution at a dose of 1 mg/kg/day, administered in two divided doses for 6 months.
Combination Group (n = 130): Participants received the same oral propranolol regimen plus monthly intralesional injections of bleomycin (1 mg/mL solution) for up to 6 months. The total dose did not exceed 1 mg/kg per session. The dose per injection site was standardized based on tumor volume: lesions <2 cm^3^ received 0.2 mg; lesions 2–5 cm^3^ received 0.3–0.4 mg; and lesions >5 cm^3^ received 0.5 mg, with multiple sites injected as needed. Injections were performed under local anesthesia using a topical lidocaine-prilocaine cream by an experienced dermatologist.
All participants underwent baseline cardiac evaluation (ECG, echocardiogram) and regular monitoring.
Outcomes and assessments
Follow-up was conducted at baseline, monthly for 6 months, and at the end of treatment. The primary outcome was the excellent clinical therapeutic effect at 6 months.
Primary Endpoint: Tumor dimensions were measured by ultrasound to calculate volume (Volume = length × width × height × 0.52). Therapeutic effect was categorized as: Complete Regression (>95% volume reduction), Marked Effectiveness (≥75%–95%), Moderate Effectiveness (30% to <75%), or Ineffective (<30%). The primary endpoint was the combined rate of “Complete Regression” and “Marked Effectiveness”.
Secondary Endpoints: 1) Early Tumor Surface Response (at 24 h), graded as Obvious Atrophy, Mild Atrophy, or No Obvious Change. 2) Hemangioma Color Evaluation using a 4-point Likert scale (0–3). 3) Scar Assessment using the Vancouver Scar Scale (VSS) at 6 months. We chose the VSS over other scales like the Hemangioma Severity Scale (HSS) because our focus was specifically on the long-term cosmetic outcome and residual skin quality after treatment, for which the VSS is the gold standard. 4) Adverse Events (AEs), graded via CTCAE v5.0.
Statistical analysis
Sample size was estimated based on an expected excellent response rate of 75% in the combination group and 55% in the monotherapy group (α = 0.05, power = 80%), requiring 127 participants per group. We enrolled 130 per group to account for dropouts. Data were analyzed using R software (version 4.2.1). Continuous variables were compared using t-tests or Mann-Whitney U tests. Categorical variables were compared using Chi-square tests, or Fisher’s exact test when expected cell counts were less than 5, such as for the adverse event analysis. Relative risk (RR) and 95% confidence intervals (CI) were calculated. P < 0.05 was considered significant. Analysis was on an intention-to-treat (ITT) basis.
Results
Participant disposition and baseline characteristics
From January 2024 to January 2025, 300 infants were assessed for eligibility. Forty were excluded (details in Table 1), and 260 were randomized (130 per group). All 260 randomized participants completed the 6-month follow-up and were included in the analysis (Figure 1). Baseline demographic and clinical characteristics were well-balanced between the two groups (Table 2).
CONSORT 2010 flow diagram of participant enrollment, allocation, follow-up, and analysis.
Primary endpoint: clinical therapeutic efficacy at 6 months
The combination therapy demonstrated markedly superior efficacy after 6 months of treatment (Table 3; Figure 2A). The proportion of patients achieving an excellent therapeutic response was significantly higher in the combination group than in the monotherapy group (77.69% vs. 50.00%; RR, 1.55; 95% CI, 1.25 to 1.93; P < 0.001). This was driven by a significantly higher rate of complete regression in the combination group (33.07% vs. 15.38%; P = 0.001). Consequently, treatment was deemed ineffective in a significantly smaller percentage of patients in the combination group (3.85% vs. 17.69%; P < 0.001).
*Comparison of primary and key secondary efficacy outcomes at 6 months. (A) Distribution of clinical therapeutic effects, showing a higher proportion of excellent responses in the combination group. (B) Boxplot showing tumor volume (cm3) at baseline and 6 months. (C) Boxplot showing hemangioma color scores at baseline and 6 months. Boxplots display the median, interquartile range, and whiskers. ***P < 0.0001 based on Chi-square test for (A) and independent t-test for (B,C) comparisons at 6 months.
Secondary endpoints
Early tumor surface response within 24 hours
An early therapeutic response was observed in both groups, but the effect was more rapid and pronounced in the combination group (Table 4). While a majority of infants in both groups showed some improvement, and the overall proportion showing any response (obvious or mild atrophy) was not statistically different (79.23% in the combination group vs. 74.61% in the monotherapy group; P = 0.377), the key difference was in the degree of response. A significantly greater proportion of patients in the combination group exhibited “Obvious Atrophy” (40.00% vs. 14.61%; P < 0.001), indicating a more potent initial effect of the combination therapy.
Tumor volume and color score reduction
After 6 months, the combination group showed significantly greater improvement in both tumor volume and color (Table 5). The mean tumor volume was approximately half that of the monotherapy group (1.63 ± 0.70 cm^3^ vs. 3.27 ± 1.06 cm^3^; P < 0.001) (Figure 2B). Similarly, the hemangioma color score improved more significantly, indicating more complete color fading (mean score at 6 months, 0.43 ± 0.29 vs. 1.25 ± 0.41; P < 0.001) (Figure 2C).
Residual scarring assessment
At the 6-month follow-up, the combination group had a superior cosmetic outcome with less residual scarring (Table 6; Figure 3). The mean total VSS score was significantly lower compared to the monotherapy group (3.68 ± 0.37 vs. 5.75 ± 0.64; P < 0.001). Significant improvements were seen in all VSS subscales (all P < 0.001).
*Assessment of residual scarring using the Vancouver Scar Scale (VSS) at 6 months. The bar chart displays the mean ± SD for each VSS component and the total score. ****P < 0.0001, *P < 0.01 based on independent t-test. The combination group showed significantly lower scores, indicating a better cosmetic outcome.
Safety and adverse events
The overall incidence of AEs was low and comparable between groups (Table 7). Local, transient redness and pain at the injection site were reported in 11/130 participants (8.46%) in the combination group. Systemic AEs possibly related to propranolol were infrequent and occurred at similar rates. No serious AEs (Grade ≥3) necessitating treatment discontinuation were reported.
Discussion
This RCT demonstrates that augmenting a low-dose oral propranolol regimen (1 mg/kg/day) with monthly intralesional bleomycin is significantly more effective than low-dose monotherapy for treating IH in infants. The combination therapy resulted in a higher rate of excellent clinical response, faster tumor atrophy, greater improvement in color and volume, and less residual scarring, all with a comparable safety profile.
The enhanced efficacy likely stems from synergistic actions. Propranolol exerts systemic effects, while intralesional bleomycin acts locally as a sclerosing agent (Muir et al., 2004; Kumar et al., 2021). Our finding of a more pronounced tumor response within 24 h supports the rapid, potent local action of bleomycin. Beyond their independent actions, a deeper synergy may exist at the cellular level. Propranolol’s inhibition of VEGF signaling not only curtails angiogenesis but may also normalize the tumor microenvironment, potentially making the aberrant endothelial cells more susceptible to bleomycin-induced DNA damage and apoptosis (Mungunsukh et al., 2010). This concept of cellular sensitization, where β-blockers enhance chemotherapy efficacy, has been explored in other oncologic contexts and may explain the accelerated regression we observed (Filippi et al., 2020; Puzderova et al., 2023).
An intriguing aspect of our findings is the superior scar outcome in the combination group, despite bleomycin’s fibrosing mechanism. We postulate that this is due to the nature of the induced fibrosis. The rapid and controlled involution promoted by the combination therapy may lead to a more organized, structured fibrosis and tissue remodeling, contrasting with the protracted inflammation and disorganized healing that can occur in large, slowly involuting hemangiomas treated with monotherapy (Luo, 2023). Thus, the therapy may replace a pathologic process with a more controlled wound-healing response, ultimately resulting in a better cosmetic appearance (Luo, 2023).
Our study has several strengths, including its randomized design, blinded outcome assessment, and use of an ITT analysis. However, limitations must be acknowledged. First, while we have now clarified the bleomycin dosing protocol, the dose was still titrated based on baseline volume rather than a fixed dose for all, which could introduce subtle variability. Second, we acknowledge the exceptional 100% follow-up rate and have addressed the likely contributing factors, though this may limit generalizability to settings with less intensive follow-up. The exceptional follow-up rate is attributed to a combination of factors including a highly motivated patient cohort, intensive follow-up coordination by a dedicated study nurse, and the provision of all treatments free of charge. Third, to minimize measurement variability in ultrasound, all assessments were performed by one of two senior radiologists, and a post hoc analysis revealed high inter-rater reliability [Intraclass Correlation Coefficient (ICC) = 0.96]. Finally, as a single-center study with a 6-month follow-up, generalizability is limited, and longer-term outcomes are unknown.
Conclusion
In conclusion, for infants with IH, augmenting a low-dose oral propranolol regimen (1 mg/kg/day) with monthly intralesional bleomycin is significantly more effective than low-dose propranolol monotherapy. This combination strategy accelerates tumor regression and yields superior cosmetic outcomes by reducing scarring, all while maintaining a comparable safety profile. This approach presents a valuable clinical option for optimizing treatment, particularly when seeking to enhance efficacy while utilizing a lower systemic dose of propranolol.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen T.Gudipudi R.Nguyen S. A.Carroll W.Clemmens C. (2023). Should propranolol remain the Gold standard for treatment of infantile hemangioma? A systematic review and meta-analysis of propranolol Versus atenolol. Ann. Otology, Rhinology, Laryngology 132 (3), 332–340. 10.1177/00034894221089758 35466712 · doi ↗ · pubmed ↗
- 2Chen Q.Rong H.Zhang L.Wang Y.Bian Q.Zheng J. (2024). KLF 2 orchestrates pathological progression of infantile Hemangioma through Hemangioma stem cell fate decisions. J. Investigative Dermatology 144 (8), 1850–64.e 9. 10.1016/j.jid.2024.01.029 38382868 · doi ↗ · pubmed ↗
- 3Filippi L.Bruno G.Domazetovic V.Favre C.Calvani M. (2020). Current therapies and new targets to fight melanoma: a promising role for the β3-Adrenoreceptor. Cancers 12 (6), 1415. 10.3390/cancers 12061415 32486190 PMC 7352170 · doi ↗ · pubmed ↗
- 4Guo L.Wang M.Song D.Sun J.Wang C.Li X. (2024). Additive value of single intralesional bleomycin injection to propranolol in the management of proliferative infantile hemangioma. Asian J. Surg. 47 (1), 154–157. 10.1016/j.asjsur.2023.05.170 37328380 · doi ↗ · pubmed ↗
- 5Hermans M. M.Schappin R.de Laat P. C. J.Mendels E. J.Breur J.Langeveld H. R. (2024). Mental health of school-aged children treated with propranolol or atenolol for infantile hemangioma and their parents. Dermatology 240 (2), 216–225. 10.1159/000536144 38228125 PMC 10997238 · doi ↗ · pubmed ↗
- 6Hoeger P. H.Harper J. I.Baselga E.Bonnet D.Boon L. M.Ciofi Degli Atti M. (2015). Treatment of infantile haemangiomas: recommendations of a European expert group. Eur. J. Pediatr. 174 (7), 855–865. 10.1007/s 00431-015-2570-0 26021855 · doi ↗ · pubmed ↗
- 7Horbach S. E. R.Rigter I. M.Smitt J. H. S.Reekers J. A.Spuls P. I.van der Horst C. (2016). Intralesional bleomycin injections for vascular malformations: a systematic review and meta-analysis. Plastic Reconstr. Surg. 137 (1), 244–256. 10.1097/PRS.0000000000001924 26710030 · doi ↗ · pubmed ↗
- 8Kiani I.Khalili M.Abdollahimajd F.Eshghi P.Khameneh Bagheri A. (2025). Ultrasound-guided percutaneous sclerotherapy with bleomycin for management of infantile subcutaneous hemangioma: a case report. Clin. Case Rep. 13 (2), e 70143. 10.1002/ccr 3.70143 39944862 PMC 11813699 · doi ↗ · pubmed ↗