Trials evaluating nicorandil renoprotection against contrast-induced nephropathy after coronary angiography or percutaneous coronary intervention: a systematic review and meta-analysis
Nestor Lemos Ferreira, Débora Regina Aguiar, Sachin G. Nair, Mohamed Ashraf Shehab, Abiodun Bamidele Adelowo, Mohammad Rafi Damirchi, Dan Jones, Krishna Rathod, Zahid Khan

TL;DR
This study finds that nicorandil may help protect kidneys during heart procedures, but more research is needed.
Contribution
The study provides new evidence on nicorandil's dose-dependent renoprotective effect against contrast-induced nephropathy.
Findings
Nicorandil reduced contrast-induced nephropathy occurrence from 13.15% to 5.14% compared to placebo.
Double-dose nicorandil further reduced CIN incidence to 3.9% compared to 8.4% with standard dose.
No significant protective effect was found against major adverse cardiovascular or kidney events.
Abstract
Ischaemic heart disease (IHD) is a leading cause of mortality and morbidity globally. Coronary angioplasty has a vital role in treating coronary artery disease. However, this is associated with a small risk of serious side effects, including contrast-induced nephropathy, vascular complications and arrhythmia. Contrast-induced nephropathy (CIN) is a serious and common complication of coronary angioplasty that can lead to renal failure and major adverse cardiac and renal outcomes. We conducted a systematic review and meta-analysis by searching multiple databases, including PubMed, Scopus, Embase, Google Scholar, and ScienceDirect, as well as other sources. The inclusion and exclusion criteria are described in detail later in this article. Two independent reviewers performed the literature search in September 2024 and identified 282 articles. The study was conducted following the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
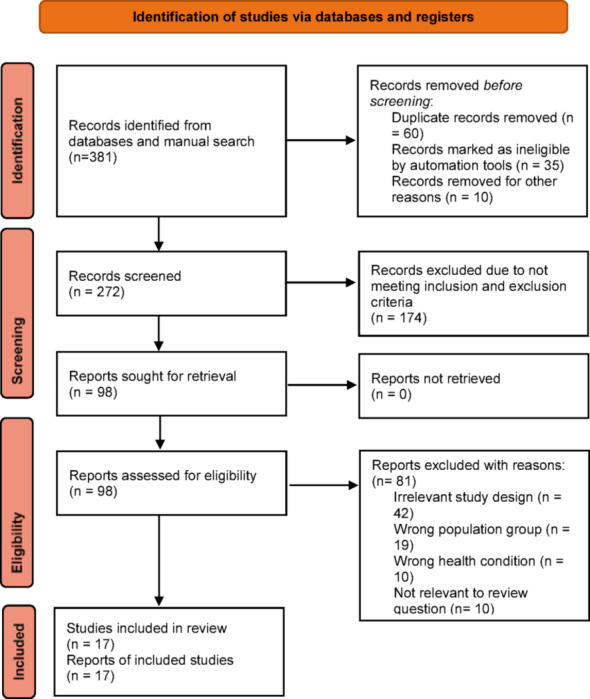 Figure 1
Figure 1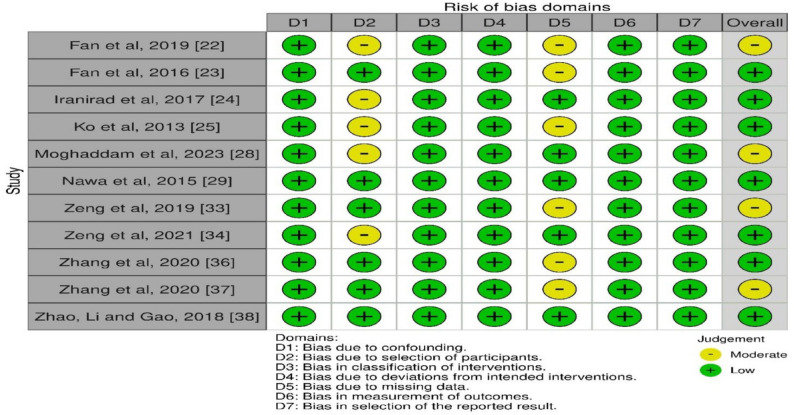 Figure 2
Figure 2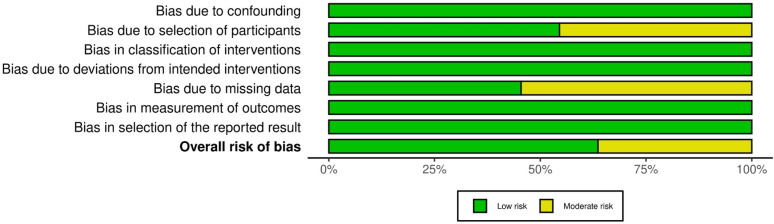 Figure 3
Figure 3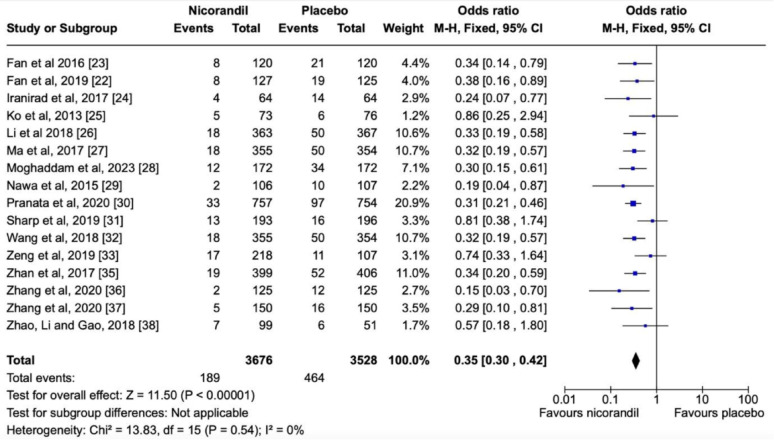 Figure 4
Figure 4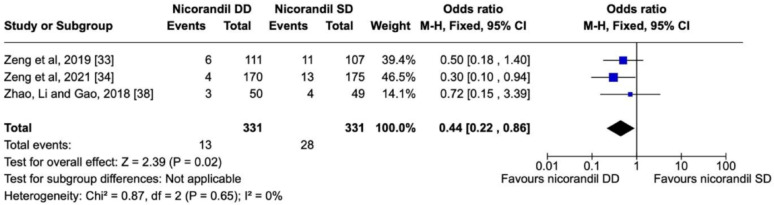 Figure 5
Figure 5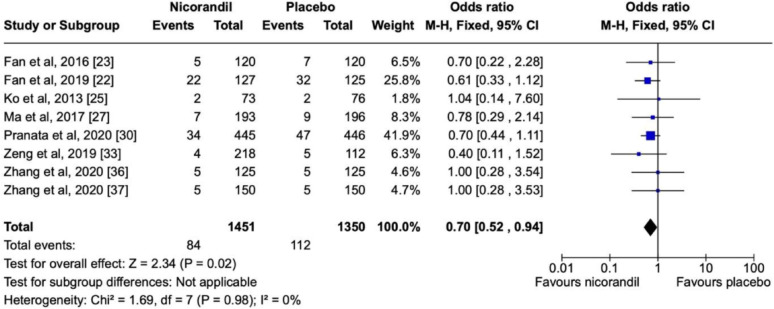 Figure 6
Figure 6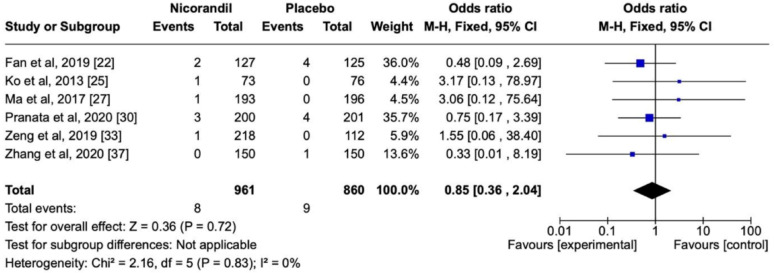 Figure 7
Figure 7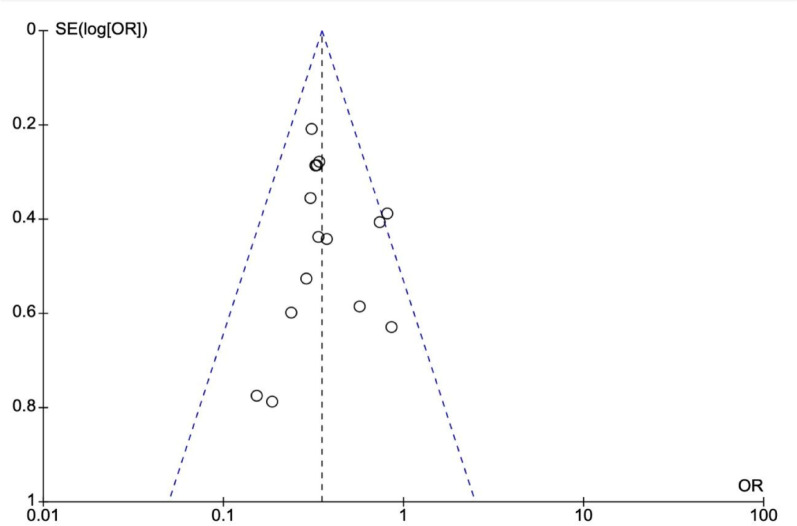 Figure 8
Figure 8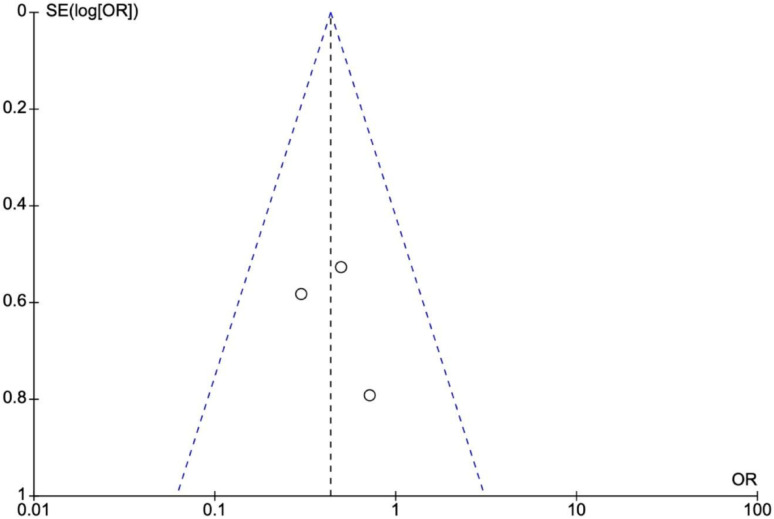 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Kidney Injury Research · Renal and Vascular Pathologies · Nitric Oxide and Endothelin Effects
Introduction
Ischaemic heart disease (IHD), also known as coronary artery disease (CAD), is the most prevalent cardiovascular disease and the leading cause of disability and mortality globally 9 [1–3]. It accounted for more than 180 million Disability-Adjusted Life Years (DALYs) in 2019 [4], approximately 720,000 cases, and over 9 million deaths globally every year [5]. Despite advances in medical care, the burden of IHD is increasing globally, thus making it a significant threat to global public health and attracting a large percentage of annual global healthcare expenditure [4, 5].
Prompt treatment of IHD with coronary angioplasty reduce the risk of patient’s mortality and comorbidity resulting in improved quality of life [6, 7]. Nevertheless, coronary angioplasty also has complications and some of these complications are related to the contrast media such as iodine and gadolinium used during coronary angioplasty. These media are also used in diagnostic tests such as computed tomography myocardial perfusion imaging (CT-MPI), coronary CT angiography (CCTA), coronary angiography (CAG), or percutaneous coronary intervention (PCI) [5, 8–11].
Contrast media induced nephropathy, allergic reaction, anaphylaxis, renal replacement therapy, major adverse cardiovascular and renal outcomes are some of the serious side effects observed in patients [8, 9]. Certain patients’ characteristics such as anemia, chronic kidney disease, diabetes mellitus, dehydration, volume of contrast used, advanced age, heart failure, multiple myeloma, hypoalbuminemia, liver cirrhosis, concomitant use of nephrotoxic drugs is more likely to predispose patients to CIN [5, 12, 13].
CIN can be defined as an increase in serum creatinine by ≥ 0.5 mg/dL (44 µmol/L) or by >25% from baseline within 48 h after the administration of radiocontrast media (RCM), without any other attributable causes [12, 14, 15]. CIN is the third most common cause of hospital-acquired ARI, responsible for approximately 12% of ARI cases, although the incidence may be as high as 24%, depending on the risk factors [15]. Various proposed mechanisms responsible for CIN included enhanced cellular damager due to reactive oxygen species, reduced intramedullary renal blood flow due to renal vasoconstriction caused by imbalance of local vasoactive mediators such as adenosine, nitrous oxide, endothelin, prostaglandin and reactive oxygen species that are released by the vascular endothelium in response to the contrast media induced cytotoxicity. The vasoconstriction effect seems to be more common in patients with chronic kidney disease [14–16].
Some of the recommended measures to reduce the risk of CIN include pre-hydration mainly in patients with chronic kidney disease (CKD), low-osmolar iodinated contrast media (ICM), and the use of prophylactic statins, low volume of contrast, stopping nephrotoxic drugs such as metformin before coronary angioplasty and reassessing renal function tests in one week post procedure [14]. Certain agents such as Nicorandil, nitrates and nitrates, ascorbic acid, theophylline, N-acetyl cysteine, high dose statins, and Prostaglandin E1 have been used to minimize the risk of CIN [17–20]. Nicorandil is an anti-anginal medicine owing to its ability to dilate blood vessels through potassium channel activation and its nitrate moiety [21]. This meta-analysis aimed at determining whether nicorandil can prevent CIN.
Objectives
The primary endpoint was to evaluate whether nicorandil exerted nephroprotection against CIN in patients undergoing CAG or PCI. The secondary endpoint was to identify major adverse events (MAE) and major adverse kidney events (MAKE) associated with CAG or PCI.
Methodology and material
This systematic review and meta-analysis were conducted using the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the PICO framework (Table 1). The study is registered with PROSPERO under registration number CRD42024567009.
Table 1. Population, intervention, comparison, and outcome (PICO) frameworkVariablesDefinitionPopulationPatients undergoing CAG or PCIInterventionAdministration of NicorandilComparison/ControlControl group on placebo treatmentOutcomeReduction of CIN events and evidence of renal protection
Data source and search strategy
The search was performed across the PubMed, Scopus, Embase, Google Scholar, and ScienceDirect databases. Some of the searched items included Nicorandil, Contrast-Induced Nephropathy, Acute Renal Injury, chronic kidney disease, impaired renal function, renal insufficiency, renoprotection, ischaemic heart disease, cardiac catheterisation, computed tomography, myocardial perfusion imaging (CT-MPI), coronary CT angiography (CCTA), coronary angiography (CAG), and percutaneous coronary intervention (PCI). The search was performed in September 2024 by two independent reviewers, identifying two hundred eighty-two (282) related articles. The articles were reduced to 49 after duplicate analyses were performed using the Rayyan App. After applying the inclusion and exclusion criteria, 17 articles were included in the study, as shown in the PRISMA chart (Fig. 1). All included articles were published between 2011 and 2023. All discrepancies were resolved through consensus.
Fig. 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram showing included studies in this meta-analysis
Inclusion criteria
The inclusion criteria were as follows: randomised controlled trials (RCTs), observational studies, case-control studies, cohort studies, systematic reviews, and meta-analyses; full articles; articles written in the English language; and articles on adult human populations regarding the effect of nicorandil, compared to placebo, on preventing CIN nephropathy after CAG/PCI.
Exclusion criteria
The exclusion criteria were as follows: guidelines, case reports, qualitative research, and letters to the editor, commentaries, conference proceedings, gray literature, opinions, policy papers, and case series.
Data collection process and data items
The literature search was performed by two reviewers and extracted data was recorded in a standardised data abstraction form (Microsoft Excel^®^). Duplicates were removed using the Rayyan software. The data collected included title, authors, year of publication, study population, intervention group, control group, follow-up period after the procedure, results in terms of CIN events comparing nicorandil and placebo, as well as nicorandil double dose (DD) and nicorandil standard dose (SD), and the analysis of nicorandil regarding MAE, which were considered as follows: nonfatal MI, revascularization, stroke, coronary artery bypass graft surgery, congestive heart failure, worsening of heart failure, pulmonary oedema, ventricular fibrillation, cardiac death, and gastrointestinal bleeding. End-stage kidney disease and temporary renal replacement therapy were the circumstances encompassed by MAKE.
Statistical analysis
Due to low heterogeneity among studies, statistical analysis was performed using the Cochrane Review Manager (RevMan) 5.3 (The Cochrane Collaboration, Copenhagen) with dichotomous data and the fixed-effect model. Having said that, this analysis mitigated the risk of assigning greater weight to the results of small-sample research. The Risk of Bias evaluation was conducted using the Cochrane Risk of Bias 2 (RoB) tool (Figs. 2 and 3), and publication bias was assessed using funnel plots. The AMSTAR-2 tool was used to determine the quality of the systematic reviews and meta-analyses in this study, categorising them as low, moderate, or high quality (Table 2).
Fig. 2. Risk of bias assessment for the studies included in this systematic review and meta-analysis
Table 2A measurement tool to assess systematic reviews 2 (AMSTAR 2) tool for assessing the risk of bias in systematic reviews and meta-analysisStudyScoreDate of analysisLi et al., [26]High quality12/25/2024Ma et al., [27]Low quality12/25/2024Pranata et al., [30]Low quality12/25/2024Sharp et al., [31]Moderate quality12/25/2024Wang et al., [32]Low quality12/25/2024Zhan et al., [35]High quality12/25/2024
Fig. 3. Risk of bias assessment plot
Table 2 presents the AMSTAR-2 tool for assessing risk of bias in systematic reviews and meta-analyses.
Results
Selected studies are shown in Table 3 and their respective forest and funnel plots in the following sequence, as per the assessed primary and secondary endpoints. Overall, the analysis showed no significant heterogeneity among the studies included. Concerning the prevention of CIN, nicorandil showed a significant protective effect in comparison with the control in terms of the overall effect (P < 0.00001) (Fig. 4) in a dose-dependent manner (P = 0.02) (Fig. 5). There was also a dose-dependent pattern in the occurrence of Major Adverse Events (MAE) (P = 0.02), as indicated by the Chi-Square test (Fig. 6). However, concerning the prevention of Major Adverse Kidney Events (MAKE), no robust findings contradicted the null hypothesis (P = 0.72) (Fig. 7). Thus, there was no significant association between MAKE and the use of nicorandil in this study.
Table 3. Patient demographic and characteristics dataAuthorType of ResearchPopulationNicorandil groupControl groupFollow-up period after procedureOccurrence of CIN eventsOccurrence of MAEOccurrence of MAKEFan et al., [22]Prospective, open- labelled, RCTCKD patients undergoing elective coronary proceduren = 127n = 1253d-1y8 events out of 127 in the nicorandil group22 out of 127 in the nicorandil group2 among 127 patients in the nicorandil group19 out of 125 compared to control32 out of 125 in the control group4 among 125 in the control groupFan et al., [23]Double blind, parallel RCTPatients with impaired renal function undergoing elective PCIn = 120n = 1203d-1 m8 events out of 120 patients in the nicorandil group5 events out of 120 patients in the nicorandil groupN/A21 events out of 120 patients in the control group7 events out of 120 patients in the control groupIranirad et al., [24]Prospective, open-label, RCTHigh-risk patients for CIN undergoing cardiac catheterisationn = 64 (10 mg nicorandil)n = 64 (saline hydration)3d4 events out of 64 patients in the nicorandil groupN/AN/A14 events out of 64 patients in the control groupKo et al., [25]Investigator- initiated, prospective, open-label, multicenter RCTPatients with renal dysfunction undergoing CAGn = 73n = 761d-2d5 events out of 73 patients in the nicorandil group2 events out of 73 patients in the nicorandil group1 event among 73 patients in the nicorandil group6 76 patients in the control group2 events out of 76 patients in the control groupNo MAKE event among 76 patients in the control groupLi et al., [26]MA of RCTsNicorandil effect on CIN prevention in patients undergoing coronary catheterisationn = 363n = 3672d-3d18 events out of 363 patients in the nicorandil groupN/AN/A50 events out 367 patients in the control group1 event out 193 patients in the nicorandil groupMa et al., [27]MA of RCTsPatients who underwent eligible CAG or PCI with increased risk for CINn = 355n = 3542d18 events out of 355 patients in the nicorandil group7 events out of 193 patients in the nicorandil group50 events out of 354 patients in the control group9 events out of 196 patients in the control groupNo MAKE event among 196 in the control groupMoghaddam et al., [28]Open-labelled RCTPatients at high- risk for CIN who underwent PCIn = 172n = 1722d12 events out of 172 patients in the nicorandil groupN/AN/A34 events out of 172 patients in the control groupNawa et al., [29]Single- center, RCTPatients with impaired renal function who underwent PCIn = 106n = 1071d2 events out of 106 patients in the nicorandil groupN/AN/A10 events out of 107 patients in the control groupPranata et al., [30]SM/MA of RCTsNicorandil effect on CIN prevention in patients undergoing coronary catheterisationn = 757n = 7542d-1y33 events out of 757 patients in the nicorandil group34 out of 445 patients in the nicorandil group3 events out of 200 patients on the nicorandil group97 events out of 754 patients in the control group47 events out of 446 patients in the control group4 events among 201 patients in the control groupSharp et al., [31]SM/MA of RCTsPharmacological CIN prevention in patients undergoing cardiac catheterisationn = 193n = 196Not mentioned13 events out of 193 patients in the nicorandil groupN/AN/A16 out of 196 patients in the control groupWang et al., [32]MA of RCTsNicorandil nephroprotection against CINn = 355n = 3541d-3d18 events out of 355 patients in the nicorandil groupN/AN/A50 events out of 354 patients in the control groupZeng et al., [33]RCTPatients who underwent cardiac catheterizationn = 111 (DD nicorandil: 30 mg/day)n = 112 (hydration)2d-14d6 events out of 111 patients in the DD group2 events out of 111 patients in the DD groupNo MAKE event in the DD groupn = 107 (SD nicorandil: 15 mg/day)11 events out of 107 patients in the SD group2 events out of 107 patients in the SD group1 event among 107 patients in the SD group16 events out of 112 patients in the control group5 events out of 112 patients in the control groupNo MAKE event in the control groupZeng et al., [34]Single- center, prospective, randomized, single-CAD patients undergoing elective coronary proceduren = 170 (DD nicorandil)n = 175 (SD nicorandil)3d4 events out of 170 patients in the nicorandil groupN/AN/Ablinded study13 events out of 175 patients in the control groupZhan et al., [35]MA of RCTsComparison between Nicorandil, ranolazoine and controln = 399n = 4061d-3d19 events out of 399 patients in the nicorandil groupN/AN/A52 events out of 406 patients in the control groupZhang et al., [36]RCTPatients with moderate renal insufficiency undergoing PCIn = 125n = 1253d2 events out of 125 patients in the nicorandil group5 events out of 125 patients in the nicorandil groupN/A12 events out of 125 patients in the control group6 events out of 125 patients in the control groupZhang et al., [37]RCTCAD patients who underwent PCIn = 150n = 1502d-14d5 events out of 150 patients in the nicorandil group5 events out of 150 patients in the nicorandil groupNo MAKE occurrence in the nicorandil group16 event out of 150 patients in control group5 events out of 150 patients in control group1 event out of 150 patients in control groupZhao, Li and Gao, [38]RCTT2DM patients who underwent CAG(n = 49) SD Nicorandil: 5 mgn = 513d3 events out of 50 patients in the DD groupN/AN/A(n = 50) DD nicorandil: 10 mg4 out of 49 patients in the SD group6 events out of 51 patients in the control groupSelected studies concerning type of research, assessed population, intervention and control administrations, follow-up period, the occurrence of CIN, MAE and MAKECIN contrast-induced nephropathy,* MAE* major adverse event,* MAKE* major adverse kidney event,* CAD* coronary artery disease,* T2DM* type 2 diabetes mellitus,* DD* double dose,* SD* standard dose,* MA* meta-analysis,* RCT* randomised controlled trial,* PCI* percutaneous coronary intervention,* CAG* coronary angiography
Fig. 4. Forest plot showing the protective effect of nicorandil versus placebo against CIN
Fig. 5. Forest plot showing positive dose dependent effect of nicorandil versus placebo against CIN
Fig. 6. Forest plot showing statistically non-significant protective effects of Nicorandil versus placebo effect against MACE
Fig. 7. Forest plot showing non-significant protective effect of Nicorandil versus placebo against MAKE
Effect of nicorandil on CIN
For this assessment, a total of 7,204 patients out of 16 papers with low heterogeneity (< 30%) (P < 0.00001; I2 = 0%) evaluating the effect of nicorandil on CIN showed a meaningful statistical difference in favor of the intervention group, as the occurrence of CIN was 5,14% in the nicorandil group, in contrast with 13.15% in the control group. Thus, the respective forest plot also confirmed the superior results of the intervention drug regarding CIN (Fig. 4).
Nicorandil dose-dependent effect on CIN
The forest plot also confirmed the dose-dependent effect of nicorandil on CIN. Among 662 patients enrolled in three research types, 3,9% in the DD group presented with CIN, compared with 8,4% in the SD group. Despite the small sample size, the CI and low heterogeneity variables showed statistical reliability (P = 0.02; I2 = 0%) (Fig. 5).
Nicorandil effect on MACE
This meta-analysis showed that CIN was less in patients receiving nicorandil compared to placebo group and the incidence of MACE was 5.7% and 8.2% in the Nicorandil group and the control group respectively. This difference was however statistically non-significant (P = 0.02; I2 = 0%). Furthermore, three studies by Ko et al. 2013, Zhang et al. 202, Zhang et al. 2019, did not show any evidence of nicorandil providing higher protection versus placebo against MACE [25, 36, 37]. The odds ratio for the use of nicorandil versus placebo using fixed effect model was 0.70 (CI 0.52–0.94).
It is also noteworthy to mention that, although authors from study [33] assessed a dose-dependent effect of nicorandil on MACE, and there was no difference between the groups. The number of MACE in the nicorandil versus SD group was 2 out of 111 and 2 out of 107 respectively.
Nicorandil consequences in terms of MAKE
The cross-sectional presentation of the diamond in Fig. 8 indicates that nicorandil administration could not contradict the null hypothesis. In other words, this study could not state that episodes of MAKE would be reduced by nicorandil use (Fig. 7).
No apparent heterogeneity was observed in these studies, and the funnel plots (Figs. 8 and 9) did not indicate publication bias. Additionally, we performed sensitivity analysis by excluding one study at a time and this did not show any significant difference in the results confirming the robustness of data and analysis.
Fig. 8. Funnel plot demonstrating no publication bias for nicorandil versus placebo against CIN, MACE and MAKE
Fig. 9. Funnel plot showing small renoprotective dose dependent effect of nicorandil versus placebo against CIN
Discussion
This systematic review and meta-analysis, whose primary endpoint was to evaluate the efficacy of nicorandil as a nephroprotective agent against CIN in patients undergoing CAG or PCI, and the secondary endpoint was to identify the major adverse events (MAE) and major adverse kidney events (MAKE) associated with CAG or PCI after the use of nicorandil, revealed many interesting results.
In renal blood flow, only 10% of the arterial blood reaches the renal medulla, making the area more susceptible to ischaemic injury than the renal cortex upon exposure to contrast media [15]. Although the exact pathophysiological mechanism of CIN has not been fully elucidated, likely causes include contrast media-induced reduction in medullary blood flow, renal tubular cell apoptosis, and the generation of oxygen-free radicals [14, 15].
Considering that endothelial nitric oxide synthase inhibition, inflammation, and oxidative stress have all been shown to alter nitric oxide (NO) bioavailability by over 82%, it is reasonable to assume that any situation that causes an imbalance between NO and free radicals, as seen after the use of some contrast media (CM), may worsen renal cell damage [40]. Thus, antioxidants that scavenge reactive oxygen species (ROS) induced by exposure to contrast media and increase NO levels in the renal microcirculation play a critical role in preventing medullary hypoxaemia and volume depletion, and in lowering interstitial pressure [40]. Kidneys are particularly vulnerable to ischemic injury due to high metabolic and osmotic stress that can affect the intricate microvascular circulation susceptible to local and systemic hypoperfusion. This hypoperfusion or ischemia is most evident in the outer medullary region of the kidneys where the oxygen requirement is quite high. This renal ischemia risk is even higher in patients with CKD due to increased metabolic demands placed on the reduced nephron bed that also faced reduced microvascular and macrovascular circulation. It is believed that the likely pathogenesis for CIN included ischemia in the outer medullary region of kidneys exacerbated by a prolonged period of renal vasoconstriction that occurs due to imbalance of local vasoactive mediators such as adenosine, nitrous oxide, prostaglandin and reactive oxygen species, released by the vascular endothelium in response to contrast media toxicity. The resulting ischemia in tissues releasees further noxious mediators that leads to prolonged duration of vasoconstriction. Additionally, the increased viscosity of the admixture of CM and bloods plasma along with the hyperosmolality of the CM in the plasma results in further reduced blood flow, red cell distortion and aggregation contributing to significant hypoperfusion due to capillary obstruction. The combination of vasoconstriction, cytotoxicity and increased viscosity together causes significant medullary ischemic injury.
Nicorandil exerts its anti-anginal effect via two primary mechanisms: the NO pathway and the potassium channel-opening pathway [21]. However, in the context of CIN, the formal mechanism appears to be a more rational justification for its use as a CIN prophylaxis/treatment agent, as the drug itself contains a nitrate moiety that, upon reaction with the sulfhydryl group, facilitates NO release [21].
Effect of nicorandil on contrast-induced nephropathy (CIN)
All included studies in this systematic review and meta-analysis demonstrated a significant nephroprotective effect of Nicorandil against CIN compared with controls, and the meta-analysis showed an overall nephroprotective impact of Nicorandil against CIN. The pooled OR on the effect of nicorandil in preventing CIN showed a strong statistically significant effect (Z = 11.17, p < 0.00001), where the odds of CIN were reduced by 64% with nicorandil use, implying it as a protective factor against CIN (OR – 0.36[0.30, 0.43]). Thus, oral nicorandil may be a promising adjunct to the standard hydration regimen for the at-risk population to prevent CIN. Results from similar studies supported this finding.
According to a recent study, the rate of arterial renal perfusion can independently predict the Congestive heart failure (CHF) outcomes in patients; thus, to balance the axis between the ‘total vascular organs’ (heart and kidney), the administration of intravenous infusion of Nicorandil was able to reduce the incidence of CIN [29]. However, the study noted that achieving a positive effect requires maintaining a stable nicorandil concentration in the blood during contrast exposure, as the latter has a longer half-life [29]. However, the study was limited to patients with early-stage kidney disease [29].
Route of administration and dosage of nicorandil in renoprotection
Most of the included studies in this systematic review and meta-analysis administered nicorandil orally at 10 mg TID. However, the best route of administration (IV vs. oral) for nicorandil has yet to be determined, and more studies are needed to reach a definitive conclusion [30]. A meta-analysis showed a favourable effect of oral Nicorandil on CIN prevention in Asian patients; however, the study included only 4 RCTs (2 per arm), had wider CIs for the IV Nicorandil, and was only of moderate design quality, limiting its impact [27]. One likely explanation for this higher renal protection offered by oral nicorandil is due to its prolonged effect or bioavailability resulting in longer vasodilatation and nephroprotection. The ‘PRINCIPLE study’ by Ko et al. inferred that intravenous administration of nicorandil did not significantly decrease the incidence of CIN [25].
Furthermore, this meta-analysis demonstrated that the nephroprotective effect of Nicorandil against CIN was dose-dependent (P = 0.02). The forest plot comparing single-dose (SD) vs. double-dose (DD) nicorandil in our study showed a statistically significant benefit for the latter, with a 55% reduction in the odds of CIN. This finding is supported by the results of a recent study, which observed that the periprocedural use of double dose (DD) nicorandil (30 mg) significantly reduced the incidence of CIN, rather than a single dose (SD), where only a slight improvement in Renal Function Test (RFT) was seen with SD [33]. In a subgroup analysis of the use of DD IV nicorandil in the referenced study, patients who received ≥ 140 ml of contrast dye showed a significant decrease in CIN incidence compared with the standard contrast dose [33]. Thus, until more studies are available, DD Nicorandil may be beneficial for renoprotection against CIN.
Major adverse events (MAE) and major adverse kidney events (MAKE) and the use of nicorandil
This study found that, in most studies, the occurrence of Major Adverse Events (MAE) after nicorandil use was dose-dependent and the overall result was statistically significant. Some of the MAEs that were observed with the use of nicorandil in the included studies, especially at high doses, were nonfatal MI, revascularisation, stroke, coronary artery bypass graft surgery, congestive heart failure, worsening of heart failure, pulmonary oedema, ventricular fibrillation, cardiac death, and gastrointestinal bleeding. However, this meta-analysis did not demonstrate a significant increase in Major Adverse Kidney Events (MAKE) with nicorandil use across the included studies. However, this result may be due to most of the included studies not including MAKE as an outcome. In addition, there is generally little data available on the effects of Nicorandil on MAKE. A few other studies have associated MAE, such as oral and gastrointestinal bleeding [41] and stroke [42], with the use of nicorandil. Thus, a cautious use and monitoring protocols for nicorandil should be initiated at any time for renoprotection against CIN or any other purpose.
Limitations
None of the included studies reported the stages of chronic kidney disease (CKD) of the included patients, as this would have provided further insight into which patient category benefited most from the intervention. However, they included patients with e-GFR ˂60 ml/min. The volume and type of contrast dye used significantly affect the incidence of CIN, but most included studies failed to account for this by not providing this information. Also, the possible long-term MAE and MAKE in patients were not investigated in terms of hospital stay length, and the cost implications of using Nicorandil were not mentioned. All this information could affect the study’s outcomes.
Conclusion
A healthy kidney is much less susceptible to potential iatrogenic complications associated with contrast media use. However, the degree of contrast media-induced acute kidney injury (AKI) and the risk of CIN vary drastically based on the presence of different harmful factors, such as advanced age, heart failure, dehydration, hypoalbuminaemia, diabetes mellitus, and anaemia. This study demonstrated that the risk of CIN in patients undergoing CAG or PCI can be reduced if nicorandil is used as a prophylaxis in addition to the standard CIN prevention protocol. Nicorandil is an effective oral medication, and its renoprotective effects are enhanced if used as a double dose. In addition, the renoprotective effect of nicorandil in this study was dose-dependent, with higher doses associated with greater MAE. Thus, while available studies have demonstrated the renoprotective effects of nicorandil in patients undergoing CAG or PCI, necessary measures and protocols should be implemented to prevent potential MAE.
Only a few studies are available on the effects of nicorandil on CIN prevention. To further generalise the potential renoprotective effects of nicorandil in patients undergoing CAG or PCI, additional studies, particularly RCTs and systematic reviews/meta-analyses, are needed. There is also insufficient information on the optimal dosage and route of administration of nicorandil in the prevention and treatment of CIN. In addition, there are limited studies on the potential renoprotective effects of nicorandil in other control conditions, such as type 2 diabetes. In fact, during the literature search, only one study reported the beneficial effect of oral Nicorandil in patients with Type 2 diabetes mellitus. Therefore, further studies are required to determine the optimal dosage, the most effective route of administration, and the effects of Nicorandil in individuals with other comorbidities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khan MAB, Hashim MJ, Mustafa H, Baniyas MY et al (2020) Shaikha Khalid Buti Mohamad Al Suwaidi, Rana Al Katheeri, Fatmah Mohamed Khalfan Alblooshi,. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 12 (7): e 9349. 10.7759/cureus.934910.7759/cureus.9349 PMC 738470332742886 · doi ↗ · pubmed ↗
- 2Sakboonyarat B (2024) and Ram Rangsin. Hospital Admission and Mortality Rates for Ischemic Heart Disease in Thailand: 2012–2021. BMC Research Notes 17 (1). 10.1186/s 13104-024-06803-x 10.1186/s 13104-024-06803-x PMC 1110261338764092 · doi ↗ · pubmed ↗
- 3Wu P, Yu S, Wang J, Zou S, Yao D-S, and Xin Yuan (2023) Global Burden, Trends, and inequalities of ischemic heart disease among young adults from 1990 to 2019: A Population-Based study. Front Cardiovasc Med 10. 10.3389/fcvm.2023.127466310.3389/fcvm.2023.1274663 PMC 1070489738075966 · doi ↗ · pubmed ↗
- 4Boucher J-F (2024) The Benefits of Early Diagnosis for Heart Disease. Laval Cardiovascular Evaluation Center. March 7, 2024. https://www.centrecardiolaval.com/en/2024/03/06/the-benefits-of 039early-diagnosis-for-heart-disease/
- 5John Hopkins Medicine. (2019) Coronary Artery Disease: Prevention, Treatment and Research. Johns Hopkins Medicine. 2019. https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronary-artery-disease-prevention-treatment-and-research
- 6Gupta A, Neupane S, Basir M (2020) and Khaldoon Alaswad. Zero-Iodinated Contrast Retrograde Percutaneous Coronary Interventions of Chronic Total Occlusions Using Gadolinium and Imaging Guidance: A Case Report of a Patient with Severe Anaphylaxis to Iodinated Contrast. Edited by Parham Eshtehardi, Christoph Jensen, Romain Didier, Alice Wood, Carlos Minguito Carazo, and Peregrine Green. European Heart Journal - Case Reports 4 (3): 1–7. 10.1093/ehjcr/ytaa 09210.1093/ehjcr/ytaa 092PMC 731980332617458 · doi ↗ · pubmed ↗
- 7Scherer K, Hammel J, Sellerer T, Mechlem K, Renger B, Bähr A, Kupatt C et al (2019) Dynamic quantitative iodine myocardial perfusion imaging with Dual-Layer CT using a Porcine model. Sci Rep 9(1). 10.1038/s 41598-019-52458-110.1038/s 41598-019-52458-1PMC 683160931690759 · doi ↗ · pubmed ↗
- 8Assen M, van M, Vonder GJ, Pelgrim PL, Von Doeberitz K, Vliegenthart R (2020) Computed tomography for myocardial characterization in ischemic heart disease: A State-of-The-Art review. Eur Radiol Experimental 4(1). 10.1186/s 41747-020-00158-110.1186/s 41747-020-00158-1PMC 729792632548777 · doi ↗ · pubmed ↗