Brodie's Abscess of the Tibia Presenting as Bilateral Hip Pain: A Diagnostic Challenge
Suleiman Sbeih, Yazan Ahmad, Mohammed Boji, Asma Mahajnah, Fawzi Abunejma, Mohammad Alashqar

TL;DR
A tibial infection can cause hip pain in children, making it hard to diagnose and requiring MRI for accurate detection.
Contribution
Highlights the diagnostic challenge of Brodie's abscess presenting as hip pain in children.
Findings
Brodie's abscess of the tibia can present as referred bilateral hip pain in children.
MRI is crucial for accurate diagnosis and guiding treatment in such cases.
Abstract
Referred hip pain in a child could mask Brodie's abscess of the tibia. Recognition of this unusual presentation and prompt MRI assessment are very important to avoid misdiagnosis and to appropriately guide surgical and antibiotic management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
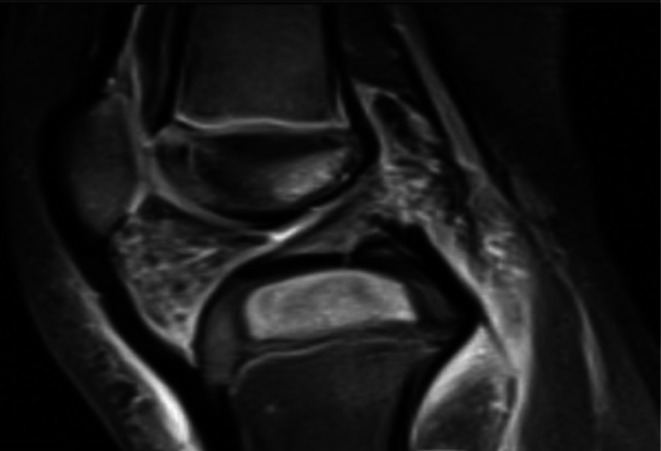 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2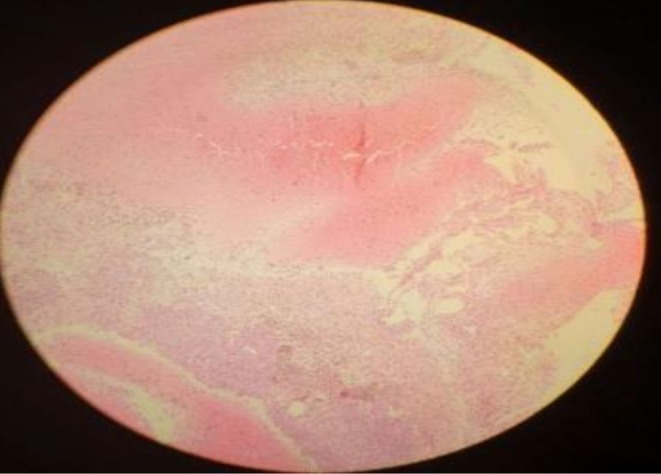 FIGURE 3
FIGURE 3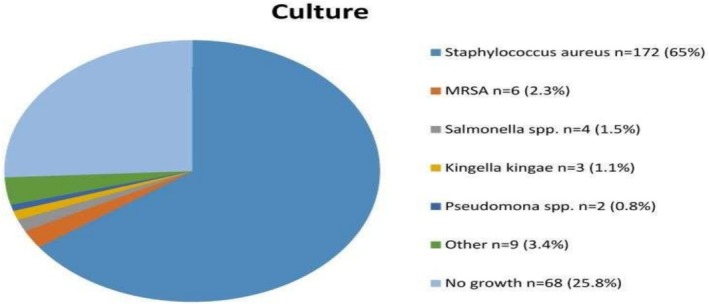 FIGURE 4
FIGURE 4| Test | Result (at admission) | Interpretation | Result (on follow‐up) |
|---|---|---|---|
| Leukocyte count | 8.3 × 109/L | Normal | 8.3 × 109/L |
| ESR | 37 mm/h | Slightly elevated | 5 mm/h |
| C‐reactive protein | 23 mg/L | Slightly elevated | 9 mg/L |
| Creatinine | 0.6 | Normal | N/A |
| BUN | 12 | Normal | N/A |
| ALT | 35 | Normal | N/A |
| AST | 30 | Normal | N/A |
| Sodium | 139 | Normal | N/A |
| Chloride | 105 | Normal | N/A |
| Potassium | 4 | Normal | N/A |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Bone fractures and treatments · Infectious Diseases and Tuberculosis
Introduction
1
Brodie's abscess is a subacute form of osteomyelitis manifesting as a pus collection within the bone, frequently with insidious onset [1, 2]. It was identified in 1832 by Sir Benjamin Brodie [3]. Brodie's abscesses occur in males more than females and typically occur in patients under the age of 25 [1], when subacute or chronic osteomyelitis affects the metaphysis of long bones (tibia, fibula and radius). It typically results from hematogenous spread, though trauma can also precipitate infection [4]. The most common pathogen is * Staphylococcus aureus*; other gram‐positive and gram‐negative bacteria, including Pseudomonas aeruginosa , Klebsiella and other gram‐negative rods may be seen. However, cultures may be sterile in up to half of cases [5].
Brodie's abscess patient typically presented with insidious onset of mild to moderate pain lasting for several weeks to months, with or without fever [6]. Diagnosis of Brodie abscess is challenging as patients may present with minor symptoms and unrevealing laboratory studies [7]. Biopsy for culture and histologic examination is often needed in addition to radiography to confirm the diagnosis [8]. The preferred method of treatment is surgical debridement followed by a prolonged course of parenteral antibiotics, and the results are typically favorable [9]. The common presentation of Brodie's abscess is characterized by the presence of localized pain over the involved bone, but there have been reports of atypical presentations with referred pain, although these are still rare occurrences, especially among young children [1, 6]. For instance, van der Naald et al. [6], Vishwakarma et al. [10], and Chen et al. [9] have presented cases where the localization of the pain was misleading and not the actual site of infection, which resulted in delays in diagnosis. Our case adds an unusual case of Brodie's abscess of the tibia being primarily expressed as bilateral hip pain, thus highlighting the diagnostic difficulty of referred pain in children.
Case History/Examination
2
A 3‐year‐old male patient presented to the pediatric ward with a 2‐weeks history of bilateral hip pain mainly at night. One week later he developed a left‐sided limp that fluctuated in severity from barely noticeable to hardly being able to bear weight. Three days prior to admission, the patient started complaining of fever and vomiting after each feeding, associated with poor oral intake. Twelve days prior to his admission the parents sought medical advice from an outpatient doctor who in turn gave him Augmentin 75 mg/kg and Ibuprofen 10 mg/kg with no improvement.
Methods (Differential Diagnosis, Investigations and Treatment)
2.1
Upon examination the patient was afebrile; his left knee (infrapatellar) was severely tender, hot and there was limitation in active and passive range of motion with no redness or any skin changes. The patient was able to walk but had a mild left‐sided limp, in which he could not bear his weight on the left leg. Hip examination was unremarkable, showing full active and passive range of motion with a negative FABER test and no signs of inflammation. The remainder of the physical examination was normal. Depending on the full musculoskeletal exam, there was a high suspicion of tibial pathology. The patient's leukocyte count was normal, with mildly elevated inflammatory markers, including erythrocyte sedimentation rate (ESR) and C‐reactive protein (CRP). Other laboratory parameters, including kidney and liver function tests, and electrolytes, were unremarkable (Table 1).
The patient was admitted to the hospital for further management and comprehensive evaluation by both orthopedic and rheumatology specialists. Upon admission, a bilateral hip and knee x‐ray was done which showed soft tissue swelling on the left knee; otherwise, it was unremarkable. A left knee ultrasound was done and showed that there were mild subcutaneous focal inflammatory changes seen in the anteroinferior aspect of the infra‐patellar region without significant joint effusion. A hip ultrasound was done and showed widening in the joint space with no effusion or collection which has no significance. Cefazolin was started while waiting for the MRI results, which were requested. MRI revealed a 2.5 cm × 1.8 cm × 1 cm oval, mass‐like lesion with heterogeneous signal intensity and enhancement located within the epiphysis of the proximal tibia (tibial plateau) (Figure 1).
MRI showing an oval, heterogeneous enhancing lesion in the proximal tibial epiphysis.
The diagnosis of subacute osteomyelitis with Brodie's abscess was favored. However, malignancy could not be excluded based on the radiologic findings, and surgical drainage was therefore undertaken (Figure 2) with biopsy and culture.
Intraoperative image of surgical drainage.
Culture returns negative and the biopsy result was consistent with Brodie's abscess (Figure 3). Initially, the patient continued Cefazolin for 7 days; vancomycin 500 mg IV every 12 h was added empirically to provide coverage for possible methicillin‐resistant Staphylococcus aureus . Upon discharge the patient was maintained on vancomycin with a good range of motion, afebrile, clean wound, CRP negative and the last ESR was 30.
Histopathology confirming Brodie's abscess.
The patient is advised to do regular follow‐up for at least 6 months; the last visit to the pediatric clinic showed marked improvement with normal x‐ray and lab values (Table 1).
Conclusion and Results
3
We reported a case of Brodie's abscess in the metaphysis of the left proximal tibia with initial presentation of bilateral hip pain. Although it is very rare, Brodie's abscess can present with referred pain as initial presentation which was shown in our case. Depending on hip physical examination and laboratory findings the plan was to send the patient home. But due to a wide differential diagnosis, which includes malignancy, further evaluation was done, and it turned out that our patient needed surgical drainage due to Brodie's abscess which was diagnosed by MRI and confirmed by biopsy.
Discussion
4
Overview of Brodie's Abscess
4.1
Brodie's Abscess is a rare condition presenting as a subacute type of bone infection leading to localized pus collection [1]. It occurs when the host defenses and the germs are equally matched, resulting in a walled‐off abscess which is responsible for reducing the systemic reaction. Both direct local bacterial invasion and hematogenous transfer of organisms to bone can result in an intraosseous infection [1, 6]. The bacteria enter the bone through a damaged area elsewhere in the body, such as a skin pustule, furuncles, infected blisters, or they enter the bone as a result of an infection in another organ system. Also, it can be caused by routine activities such as brushing teeth [11]. Frequently, the infected focus remained undetected.
Epidemiology
4.2
According to a systemic review of reported cases comprising a total of 70 articles (including 407 patients), Brodie's Abscess is typically seen in a young population with a median age of 17 years with minimal incidence in adult populations [6]. Sex ratios vary but in general males are affected slightly more often than females (M: F, 2.1:1) [6].
Clinical Presentation
4.3
Localized Pain is the most common complaint in most patients 98% accompanied by swelling in 53% of patients. 84% of patients were afebrile [6, 12]. However, our patient complained of fever and vomiting, and the hip pain was referred pain.
Diagnostic Challenges and Imaging
4.4
Symptoms of subacute osteomyelitis are nonspecific; an accurate diagnosis is sually delayed (a median of 12 weeks before diagnosis was established). The tibia (48.6%) and femur (31.1%) were mostly involved. The result of all cultures is presented in (Figure 4) [6, 13]. Given the nonspecific feature of Brodie's abscess, a high suspicion index is required along with confirmatory biopsy and MRI which are the diagnostic modalities of choice for Brodie's abscess, while the inflammatory markers ESR, CRP, and CBC have a limited role in the diagnosis [13]. ESR (55.4%) and CRP (77.5%) were mostly normal or slightly elevated [6], as in our case. Our patient was diagnosed with Brodie's abscess according to the imaging modalities (x‐ray, MRI) and biopsy to rule out other differential diagnoses like malignancy.
Distribution of culture results.
Management and Prognosis
4.5
The management of Brodie's abscess is still a controversial [6]; however, the treatment mainly involves a combination of surgical and antibiotic therapy [1]. The choice of surgery depends on tumor size and location [14]. Empirical coverage for Staphylococcus aureus is usually advised, and agents like cefazolin, oxacillin, or vancomycin are used when MRSA is diagnosed or suspected [15]. In the case of small, well‐localized abscesses with confirmed diagnosis and close follow‐up, the conservative management with antibiotics only option might be considered [1], but in such cases, higher recurrence rates are experienced. As a whole, the combined surgical and medical management leads to excellent prognosis and full functional recovery in most patients [6].
Author Contributions
Suleiman Sbeih: writing – original draft, writing – review and editing. Yazan Ahmad: writing – original draft, writing – review and editing. Mohammed Boji: writing – original draft, writing – review and editing. Asma Mahajnah: writing – original draft, writing – review and editing. Fawzi Abunejma: writing – original draft, writing – review and editing. Mohammad Alashqar: software, validation, writing – original draft, writing – review and editing.
Ethics Statement
Informed consent was obtained from the patient's parents. Our institution does not require ethical approval for case reports.
Consent
Written informed consent was obtained from the patient's parents for publication of this case report and the accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. Quintana‐Ortega , I. Rimbau Serrano , A. Remesal , S. Murias , J. Cabello , and C. Calvo , “Exclusively Oral Antibiotic Therapy for Brodie's Abscess in a Pediatric Patient,” Revista Colombiana de Reumatologia 30, no. 4 (2023): 352–355, 10.1016/j.rcreu.2021.10.002. · doi ↗
- 2B. Gabbott , G. Faria , G. Lawson , and K. Daly , “A Brodie's Abscess With Soft Tissue Collection‐Complicating an Already Difficult Diagnosis,” Journal of Surgical Case Reports 2018, no. 1 (2018): rjx 263, 10.1093/jscr/rjx 263.29383243 PMC 5786206 · doi ↗ · pubmed ↗
- 3M. L. Kanoun , A. Khorbi , C. Khmiri , et al., “Diagnosis and Treatment of Brodie's Abcess in Adults: About Twenty Cases,” La Tunisie Médicale 85, no. 10 (2007): 857–861.18236808 · pubmed ↗
- 4J. H. Calhoun , M. M. Manring , and M. Shirtliff , “Osteomyelitis of the Long Bones,” Seminars in Plastic Surgery 23, no. 2 (2009): 59–72, 10.1055/s-0029-1214158.20567728 PMC 2884908 · doi ↗ · pubmed ↗
- 5M. D'souza , J. Xu , E. John , and P. Parikh , “Brodie Abscess of the Jaw: An Unusual Presentation of a Rare Complication of Subacute Osteomyelitis,” Case Reports in Internal Medicine 4, no. 3 (2017): 75, 10.5430/crim.v 4n 3p 75. · doi ↗
- 6N. van der Naald , D. P. J. Smeeing , R. M. Houwert , F. Hietbrink , G. A. M. Govaert , and D. van der Velde , “Brodie's Abscess: A Systematic Review of Reported Cases,” Journal of Bone and Joint Infection 4, no. 1 (2019): 33–39, 10.7150/jbji.31843.30755846 PMC 6367194 · doi ↗ · pubmed ↗
- 7J. Chin , T. Naito , K. Hon , and C. Lomiguen , “Challenges in the Diagnosis of Brodie's Abscess in Subacute Osteomyelitis,” Journal of Orthopaedic Case Reports 10, no. 3 (2020): 1–4, 10.13107/jocr.2020.v 10.i 03.1722.PMC 805158133954124 · doi ↗ · pubmed ↗
- 8S. Kamio , M. Arai , S. Matsumoto , M. Saito , N. Asano , and R. Nakayama , “Radiological Changes in the Formation of Brodie's Abscess by Sequential Magnetic Resonance Imaging: A Case Report,” Radiology Case Reports 16, no. 10 (2021): 2993–2997, 10.1016/j.radcr.2021.07.001.34401040 PMC 8353412 · doi ↗ · pubmed ↗