Economic impact of multiple recurrent Clostridioides difficile infection in a community teaching hospital
Joseph Reilly, Gemma Downham, Manish Trivedi

TL;DR
This study shows that repeated Clostridioides difficile infections caused a significant financial loss for a community teaching hospital.
Contribution
The study quantifies the economic burden of multiple recurrent Clostridioides difficile infections in a community hospital setting.
Findings
29 patients with multiple Clostridioides difficile infections were studied over 4 years.
The hospital experienced an estimated net loss of $2,232,997 due to these infections.
Abstract
A retrospective study evaluating the economic impact on a community teaching hospital of 29 patients with multiple Clostridioides difficile infection admissions in a 4-year period showed an estimated net loss of $2,232,997, posing a substantial economic impact on the hospital.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
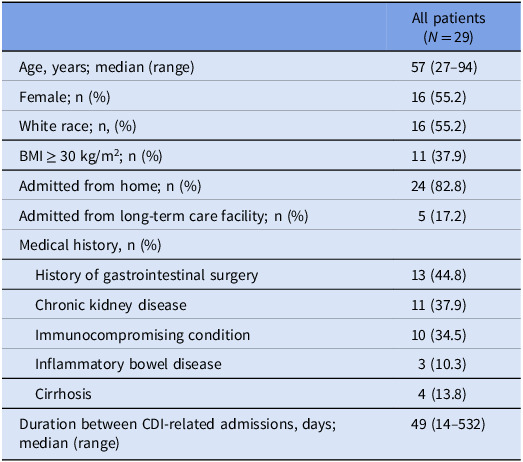 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Nosocomial Infections in ICU · Antibiotic Use and Resistance
Introduction
Clostridioides difficile infection (CDI) is a major burden to patients and the healthcare system, with approximately 500,000 cases per year in the United States and 30,000 annual deaths directly attributable to CDI.^ 1–3 ^
Roughly 20–35% of patients with an initial CDI case experience a recurrence, and 50–65% of patients who have a first recurrent CDI (rCDI) case experience a second or subsequent rCDI.^ 3 ^ Rates of rCDI have been increasing in recent years, and the disease is considered a major public health threat.^ 3,4 ^ Multiple recurrent CDI (mrCDI; ≥2 rCDI cases) poses a significant burden.^ 5 ^ Compared to an initial CDI case, healthcare costs for rCDI are notably higher, with an additional all-cause economic burden of 60,000.^ 6 ^
There are few data available on the net economic impact of repeat CDI admissions at the level of a single hospital or healthcare system. This study evaluated the economic impact on a community teaching hospital of repeat admission of patients with multiple CDI admissions.
Methods
Study design
A retrospective cohort study of patient medical records at AtlantiCare Regional Medical Center (Pomona, NJ) was conducted for the period of January 2017 through December 2020, using clinical software (TheraDoc®, Premier Inc.). This study was approved by the AtlantiCare Regional Medical Center Institutional Review Board.
Eligibility criteria
Patients were included if they had ≥3 inpatient admissions due to CDI (primary diagnosis) and tested positive for CDI between January 2017 and December 2020. Admissions for CDI occurring ≥ 8 weeks after the completion of treatment for a previous CDI case were included to provide a real-world assessment of disease impact in a clinical setting, regardless of whether it is defined as “recurrence” or “reinfection” by standard definitions. CDI was identified by two positive sequential tests: a nucleic acid amplification test for toxigenic strains of C. difficile and an enzyme immunoassay for glutamate dehydrogenase. Patients who tested positive for CDI but did not display clinical signs and symptoms of infection were excluded. Admissions for reasons other than CDI were excluded.
Data extraction
Information collected included: demographics; comorbid conditions and immune status; length of hospital stay for each CDI-related admission; acuity of care; CDI severity; mortality; utilization of antimicrobials; laboratory parameters; and time between admissions. Sepsis was recorded in the patient’s medical record and determined by hospital criteria including one sign of organ dysfunction and ≥ 2 indicators for systemic inflammatory response syndrome.
Immunocompromised was defined as: diagnosis of HIV/AIDS; receiving chemotherapy or radiation therapy (concomitant or within 3 months of admission); prior organ transplant; chronic corticosteroid use (≥10 mg daily prednisone or equivalent); autoimmune disorder; or treatment with an immune suppressing medication.
For CDI severity, non-fulminant, non-severe disease was defined as concomitant WBC count <15,000 cells/mL and serum creatinine (sCr) <1.5 mg/dL. Non-fulminant, severe disease was concomitant WBC count ≥15,000 cells/mL and sCr ≥1.5 mg/dL. Fulminant disease was the presence of hypotension or shock, ileus, or megacolon.^ 7,8 ^
Patient data analysis
Investigators reviewed the extracted data and assessed for factors potentially contributing to developing CDI. Demographic characteristics and healthcare utilization were summarized with descriptive statistics.
Economic analysis
The net economic impact of CDI-related hospitalizations for multiple CDI was estimated for the hospital. The cost of one inpatient day in 2020 at our non-profit hospital in Southern New Jersey was set at 3200.^ [9](#ref9) ^ The cost of one day in the intensive care unit (ICU) was set at 5000 (adjusting available figures from 2010 to 2020 using the Medical Care component of the Consumer Price Index).^ 10,11 ^ The estimated reimbursement for a hospitalization with a primary diagnosis code of CDI (ICD9-CM code: 008.45; ICD 10-CM codes: A04.7, A04.71 or A04.72) was set at 15,670 for fulminant CDI cases, taking into account published literature, Centers for Medicare and Medicaid reimbursement rates, and current hospital data.^ 12,13 ^ Costs were adjusted to 2020 US dollars.
Results
Demographics and baseline characteristics
Twenty-nine patients were included in this analysis, with a mean (SD) age of 58.9 (14.3) years; 55% of patients were female (Table 1). All 29 patients received CDI-related antimicrobials (63.9% received oral vancomycin, 36.1% received fidaxomicin) during admission(s). Sepsis was reported during 36 admissions (33.3%), and 31 (28.7%) were fulminant CDI cases. Many patients had ≥1 comorbid conditions that are known risk factors for (r)CDI (Table 1).
Table 1.Patient characteristicsAll patients (N = 29)Age, years; median (range)57 (27–94)Female; n (%)16 (55.2)White race; n, (%)16 (55.2)BMI ≥ 30 kg/m^2^; n (%)11 (37.9)Admitted from home; n (%)24 (82.8)Admitted from long-term care facility; n (%)5 (17.2)Medical history, n (%) History of gastrointestinal surgery13 (44.8) Chronic kidney disease11 (37.9) Immunocompromising condition10 (34.5) Inflammatory bowel disease3 (10.3) Cirrhosis4 (13.8)Duration between CDI-related admissions, days; median (range)49 (14–532)BMI, body mass index
Healthcare utilization
A total of 108 admissions due to CDI in 29 patients were identified over the study period of 4 years; 1006 inpatient hospital days were attributed to a CDI diagnosis in this sample, including 74 days in the ICU. Five additional CDI cases were excluded from the analysis because CDI developed during a hospitalization and not as an admitting diagnosis.
Patients had a median (range) number of admissions of 3 (3–6) per patient. The median (range) length of stay per admission was 7 (1–69) days. The median (range) duration between admissions was 49 (14–532) days. Most admissions were for CDI recurring within 8 weeks of the previous case. In addition, all 29 patients in the sample had ≥2 non-CDI-related admissions during the study period, which totaled 78 non-CDI-related admissions.
Economic outcomes
Total hospitalization costs for the 29 patients over the 4-year study period were estimated to be 1,119,403.
Thus, we estimated that the community teaching hospital had a net loss of 77,000 over the 4-year study period.
Patient outcomes
One patient died within the study period, due to respiratory failure, with hepatic encephalopathy, colitis, and toxic megacolon.
Discussion
Few data exist on multiple CDI-attributable hospitalization costs and resource utilization. A single-center study estimated the hospitalization costs for rCDI-related admissions to be 30,122 per patient in the 1-year study period (2016 US dollars).^ [14](#ref14) ^ More recent estimates from a systematic literature review and a component-based cost synthesis estimated rCDI-attributable hospitalization costs to be an average of 45,000–52,000 per patient per year.^ [3](#ref3) ^ Here, we estimated an average cost of multiple CDI-related hospitalizations to be 28,900 per patient, per year. Our economic analysis for CDI may underestimate the true financial losses incurred that are attributable to multiple CDI. Full reimbursement for every CDI admission was assumed, which may not be the case with multiple CDI if a readmission occurs within 30 days of the previous discharge.
All patients in this group had ≥2 non-CDI–related admissions during the study. These admissions pose greater possible financial losses for the hospital.
Limitations of this analysis include small sample size, lack of a comparator group, findings that may not be generalizable to other types of hospitals or healthcare systems, and outcomes that may differ for payors other than Medicare, which may have higher reimbursement rates for hospitalizations with a primary diagnosis of CDI that could result in an underestimate of the reimbursement and an overestimate of the net losses in this analysis. The more flexible definition of multiple CDI cases used in this manuscript may overestimate the economic impact of rCDI.
Our findings indicate that there is an ongoing cycle of CDI admissions among a subset of patients who experience CDI, which poses a substantial economic impact on the hospital.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Guh AY , Mu Y , Winston LG , et al. Trends in U.S. burden of Clostridioides difficile infection and outcomes. N Engl J Med 2020;382:1320–1330 32242357 10.1056/NEJ Moa 1910215 PMC 7861882 · doi ↗ · pubmed ↗
- 2Finn E , Andersson FL , Madin-Warburton M. Burden of Clostridioides difficile infection (CDI)—a systematic review of the epidemiology of primary and recurrent CDI. BMC Infect Dis 2021;21:456 34016040 10.1186/s 12879-021-06147-y PMC 8135979 · doi ↗ · pubmed ↗
- 3Feuerstadt P , Theriault N , Tillotson G. The burden of CDI in the United States: a multifactorial challenge. BMC Infect Dis 2023;23:132 36882700 10.1186/s 12879-023-08096-0PMC 9990004 · doi ↗ · pubmed ↗
- 4Centers for Disease Control and Prevention. Antibiotic resistance threats in the united states, 2019; 2019
- 5Ma GK , Brensinger CM , Wu Q , Lewis JD. Increasing incidence of multiply recurrent Clostridium difficile infection in the United States. Ann Intern Med 2017;167:152–158 28672282 10.7326/M 16-2733 · doi ↗ · pubmed ↗
- 6Malone DC , Armstrong EP , Gratie D , Pham S V , Amin A. A systematic review of real-world healthcare resource use and costs of Clostridioides difficile infections. Antimicrob Stewardship Healthc Epidemiol 2023;3:e 17 10.1017/ash.2022.369PMC 987986836714290 · doi ↗ · pubmed ↗
- 7Johnson S , Lavergne V , Skinner AM , et al. Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of Clostridioides difficile infection in adults. Clin Infect Dis 2021;73:e 1029–e 1044 10.1093/cid/ciab 54934164674 · doi ↗ · pubmed ↗
- 8Mc Donald LC , Gerding DN , Johnson S , et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis 2018;66:e 1–e 48 10.1093/cid/cix 1085 PMC 601898329462280 · doi ↗ · pubmed ↗