Interrelationship Between the Morning-to-Evening Changes in Home Blood Pressure and Pulse Rate
Jia-Bo Zhu, Qian-Hui Guo, Yi Zhou, Wen-Yuan-Yue Wang, Yuan-Yuan Kang, Xiao-Fei Ye, Xin-Yu Wang, Ming-Xuan Li, Yan Li, Ji-Guang Wang

TL;DR
This study found that blood pressure decreases while pulse rate increases from morning to evening in older adults with hypertension, and these changes are linked.
Contribution
The study reveals a novel interrelationship between morning-to-evening changes in home blood pressure and pulse rate in hypertensive patients.
Findings
Systolic and diastolic blood pressure decreased from morning to evening, while pulse rate increased.
Changes in pulse rate were negatively associated with changes in both systolic and diastolic blood pressure.
Higher evening pulse rate changes were linked to lower blood pressure control rates in patients.
Abstract
We investigated the morning-to-evening changes in home blood pressure (BP) and pulse rate for demographic and clinical determinants, interrelationship, and association with BP control in treated patients with hypertension. We performed a cross-sectional analysis in patients (≥55 years of age) with hypertension, enrolled in a China nationwide registry on home BP monitoring between 2020 and 2025. Home BP was measured three times consecutively in the morning and evening, respectively, for seven consecutive days. The change was calculated by subtracting the BP and pulse rate values in the morning from those in the evening. The 4,787 participants had a mean (±SD) age of 66.1 (±7.5) years, and included 2,366 (49.4%) men. Overall, systolic/diastolic BP decreased from 129.1/80.6 mmHg in the morning to 127.2/78.7 mmHg in the evening by a mean change of −1.9 ± 7.8/−1.8 ± 4.7 mmHg. Pulse rate,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
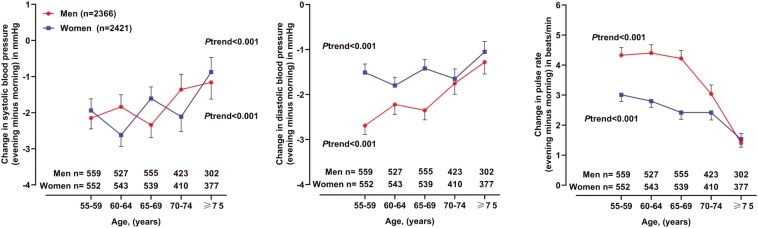 Figure 1
Figure 1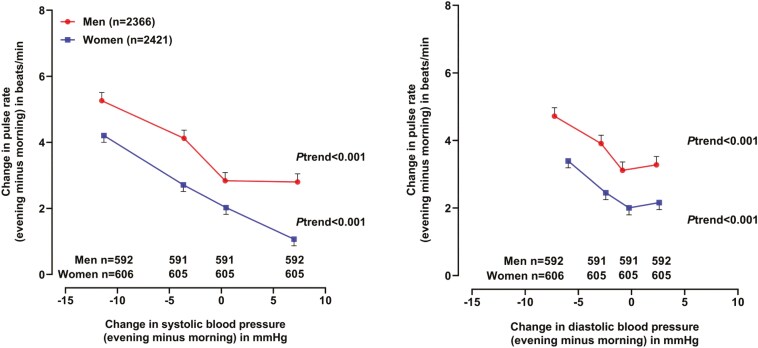 Figure 2
Figure 2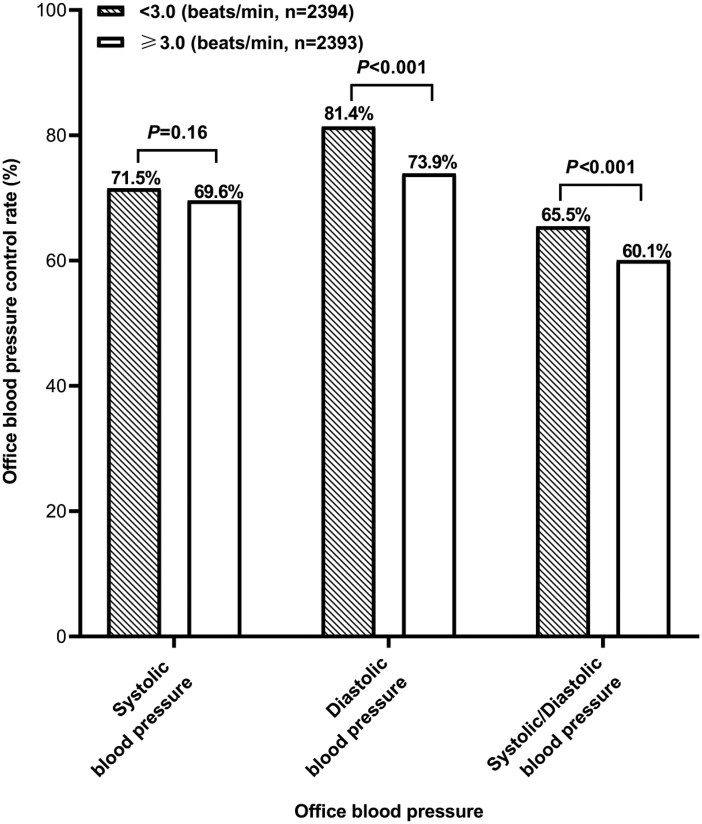 Figure 3
Figure 3| Characteristic | Men | Women |
|
|---|---|---|---|
| ( | ( | ||
| Age, years | 65.9 ± 7.3 | 66.3 ± 7.7 | 0.067 |
| Body mass index, kg/m2 | 25.4 ± 3.0 | 24.9 ± 3.3 | <0.001 |
| Current smoking, | 743 (31.4) | 15 (0.6) | <0.001 |
| Alcohol intake, | 793 (33.5) | 20 (0.8) | <0.001 |
| Hypertension duration, years | 11.9 ± 9.4 | 10.5 ± 9.4 | <0.001 |
| Number of antihypertensive medications, | 1.7 ± 0.9 | 1.5 ± 0.8 | <0.001 |
| Office blood pressure measurement | |||
| Systolic blood pressure, mmHg | 133.1 ± 17.1 | 130.2 ± 17.3 | <0.001 |
| Diastolic blood pressure, mmHg | 83.4 ± 10.6 | 80.0 ± 10.5 | <0.001 |
| Pulse rate, beats/min | 75.0 ± 11.0 | 74.4 ± 10.2 | 0.029 |
| Home blood pressure measurement | |||
| Morning systolic blood pressure, mmHg | 130.3 ± 13.6 | 127.9 ± 13.7 | <0.001 |
| Morning diastolic blood pressure, mmHg | 82.3 ± 8.8 | 78.9 ± 8.6 | <0.001 |
| Morning pulse rate, beats/min | 70.8 ± 9.5 | 70.3 ± 8.6 | 0.025 |
| Evening systolic blood pressure, mmHg | 128.4 ± 13.3 | 126.0 ± 13.2 | <0.001 |
| Evening diastolic blood pressure, mmHg | 80.2 ± 8.3 | 77.4 ± 8.4 | <0.001 |
| Evening pulse rate, beats/min | 74.6 ± 9.7 | 72.8 ± 8.6 | <0.001 |
| Double product (mmHg·beats/min) | |||
| Office | 9,975 ± 1,919 | 9,666 ± 1,772 | <0.001 |
| Home morning | 9,216 ± 1,497 | 8,973 ± 1,386 | <0.001 |
| Home evening | 9,571 ± 1,551 | 9,164 ± 1,418 | <0.001 |
| Blood biochemistry | |||
| Plasma fasting glucose, mmol/L | 6.1 ± 1.9 | 6.0 ± 1.8 | 0.030 |
| Serum total cholesterol, mmol/L | 4.5 ± 1.1 | 5.0 ± 1.2 | <0.001 |
| Serum triglycerides, mmol/L | 1.7 ± 1.1 | 1.7 ± 1.1 | 0.238 |
| Serum high-density lipoprotein cholesterol, mmol/L | 1.3 ± 0.4 | 1.4 ± 0.5 | <0.001 |
| Serum low-density lipoprotein cholesterol, mmol/L | 2.6 ± 0.9 | 2.8 ± 0.9 | <0.001 |
| Serum creatinine, μmol/L | 82.3 ± 35.9 | 65.7 ± 27.0 | <0.001 |
| Serum uric acid, μmol/L | 355.3 ± 93.2 | 298.6 ± 82.8 | <0.001 |
| Diabetes mellitus, | 733 (31.0) | 637 (26.3) | 0.001 |
| Dyslipidemia, | 1,340 (56.6) | 1,353 (55.9) | 0.620 |
| Cardiovascular disease, | 518 (21.9) | 403 (16.6) | <0.001 |
| Variable | Change in SBP, mmHg | Change in DBP, mmHg | Change in pulse rate, beats/min | |||
|---|---|---|---|---|---|---|
| β ± SE |
| β ± SE |
| β ± SE |
| |
| Model | ||||||
| Age, + 5 years | 0.23 ± 0.08 | 0.003 | 0.16 ± 0.05 | <0.001 | −0.21 ± 0.06 | <0.001 |
| Male sex | 0.28 ± 0.26 | 0.279 | −0.22 ± 0.16 | 0.171 | 0.39 ± 0.19 | 0.038 |
| Body mass index, kg/m2 | - | - | −0.05 ± 0.02 | 0.029 | 0.21 ± 0.03 | <0.001 |
| Current smoking (yes vs. no) | 1.93 ± 0.35 | <0.001 | 0.80 ± 0.21 | <0.001 | 1.25 ± 0.25 | <0.001 |
| Alcohol intake (yes vs. no) | −2.11 ± 0.34 | <0.001 | −1.52 ± 0.21 | <0.001 | 1.30 ± 0.25 | <0.001 |
| Hypertension duration, + 5 years | −0.17 ± 0.06 | 0.007 | −0.08 ± 0.04 | 0.047 | −0.15 ± 0.05 | 0.001 |
| Serum HDL cholesterol, + 0.1 mmol/L | - | - | 0.38 ± 0.15 | 0.013 | - | - |
| Serum triglycerides, + 0.1 mmol/L | - | - | - | - | 0.21 ± 0.07 | 0.004 |
| ACEIs use (yes vs. no) | −1.39 ± 0.49 | 0.004 | −0.78 ± 0.29 | 0.007 | - | - |
| ARBs use (yes vs. no) | −1.11 ± 0.26 | <0.001 | −0.77 ± 0.16 | <0.001 | 0.60 ± 0.16 | <0.001 |
| α-blockers use (yes vs. no) | - | - | - | - | −2.87 ± 0.66 | <0.001 |
| β-blockers use (yes vs. no) | - | - | −0.57 ± 0.18 | 0.002 | −0.62 ± 0.22 | 0.005 |
| CCBs use (yes vs. no) | −0.57 ± 0.27 | 0.033 | −0.41 ± 0.16 | 0.011 | - | - |
- —National Natural Science Foundation of China10.13039/501100001809
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Sodium Intake and Health · Circadian rhythm and melatonin
Current hypertension guidelines recommend the use of home blood pressure monitoring (HBPM) for the management of hypertension.^1–4^ As one of the out-of-office blood pressure measurement techniques, HBPM may improve prognostic assessment for hypertension-mediated organ damage and cardiovascular clinical outcomes. In addition, it is complementary to ambulatory blood pressure monitoring in the differentiation of white-coat from sustained hypertension and identification of masked hypertension from true normotension.^5–9^
HBPM usually requires 2–3 blood pressure measurements in the morning and evening for seven consecutive days. The evening measurements can be performed either before or after supper, depending on the time of supper. Regardless of whether the evening measurements are performed before supper, such as in Europe or United States,^1,2,10^ or after super in Asia,^3,4,11,12^ there is a morning-to-evening blood pressure difference. There is evidence that a big difference, for instance, greater than 20 mmHg, is associated with unfavorable clinical outcomes.^13–15^ However, few studies have ever investigated the determinants of the morning-to-evening blood pressure difference, especially with regard to its relationship with the possible changes in pulse rate. In the present study, we investigated the morning-to-evening changes in home blood pressure and pulse rate, and their association with office blood pressure control.
METHODS
Study Population
We performed cross-sectional analysis in treated patients (≥55 years of age) with hypertension, enrolled in an ongoing China nationwide registry on HBPM (Action of Controlling Home Blood Pressure to Target in Ten Thousand Patients). For inclusion, outpatients seen in a hospital or a community health center had to be ≥55 years, and had been treated with antihypertensive drugs. We excluded hospitalized patients and those newly diagnosed and untreated hypertensive patients. The study protocol was approved by the ethics committee of Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China. All study participants gave informed written consent.
Office and Home Blood Pressure Measurements
Office blood pressure was measured three times consecutively with a 1-minute interval using a validated, automated upper arm cuff device (HEM-9200T Omron Healthcare, Kyoto, Japan),^16^ after resting for at least 5 minutes in the sitting position. An appropriately sized cuff was used. These three readings of blood pressure and pulse rate were averaged for analysis.
All participants were instructed for standardized HBPM,^4^ especially for placing an appropriately sized cuff around his or her non-dominant arm. HBPM was performed using the same model of automated blood pressure monitor (Omron HEM-9200T) for seven consecutive days. Blood pressure was measured three times consecutively with a 1-minute interval after resting for at least 5 minutes in the sitting position. Blood pressure in the morning was measured within 1 hour of waking up, before drug intake and breakfast, and after urination, without vigorous exercise. Blood pressure in the evening was measured after super and a shower or bath and before going to sleep.^4^ Blood pressure and pulse rate readings were automatically transmitted to a digital platform for storage, analysis, and reporting. All home blood pressure and pulse rate readings were averaged for analysis.
Questionnaire and Anthropometric and Biochemical Measurements
A standardized questionnaire was administered to collect information on medical history, lifestyle, and use of medications. Body weight was measured with light indoor clothing and without shoes. Body height was measured to the nearest 0.5 cm. Body mass index (BMI) was calculated as the body weight in kilograms divided by the body height in meters squared. Venous blood samples were drawn after overnight fasting for measurement of serum triglycerides, serum total, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, and serum creatinine and uric acid, and plasma glucose.
Diabetes mellitus was defined as a plasma glucose concentration ≥7.0 mmol/l, or use of antidiabetic drugs, or as a diagnosis self-reported or documented in practice or hospital records. Dyslipidemia included hypertriglyceridemia defined as a serum triglycerides concentration ≥2.30 mmol/l, hypercholesterolemia defined as a serum total cholesterol concentration ≥6.20 mmol/l or a serum LDL cholesterol concentration ≥4.10 mmol/l, a serum HDL cholesterol concentration <1.00 mmol/l, or the current use of lipid-lowering medications, or as a diagnosis self-reported or documented in practice or hospital records.^17^ Cardiovascular diseases refer to past medical history of cardiac, cerebrovascular, and peripheral arterial diseases according to the International Classification of Diseases, 9^th^ Revision (ICD-9, codes 391.001 to 448.901) or International Classification of Diseases, 10^th^ Revision (ICD-10, codes I01.001 to I98.801). The diagnosis of cardiovascular diseases was either documented in the practice or hospital medical records, self-reported, or based on the use of cardiovascular therapeutic agents.
Statistical Analysis
The SAS software version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for data management and statistical analysis. Means and proportions were compared using the student’s t-test and Fisher’s exact test, respectively. The morning-to-evening changes in blood pressure and pulse rate were calculated by subtracting the values in the morning from those in the evening. Negative values indicate a reduction from morning to evening. We performed univariate analysis and multiple stepwise linear regression analysis to investigate the determinants of the morning-to-evening changes in home blood pressure and pulse rate. In the multiple regression models, we forced age and sex and considered BMI, current smoking and alcohol intake, hypertension duration, history of cardiovascular disease, diabetes mellitus and dyslipidemia, serum triglycerides, serum total, HDL and LDL cholesterol, plasma fasting glucose, serum creatinine and uric acid and the use of angiotensin-converting enzyme inhibitor (ACEIs), angiotensin receptor blockers (ARBs), α-blockers, β-blockers, and calcium channel blockers (CCBs) as covariates to enter and stay at a significance level set at 0.05. Furthermore, we performed analyses of covariance according to the sex-specific quartile distributions to investigate the interrelationship between the morning-to-evening changes in home blood pressure and pulse rate, while accounting for sex, age and the determinants identified in the above multiple regression analyses. Finally, we performed analyses on the control of office blood pressure (<140/90 mm Hg) in relation to the morning-to-evening changes in home pulse rate at baseline. Double product was calculated by systolic blood pressure times pulse rate. P values < 0.05 were considered statistically significant.
RESULTS
Characteristics of the Study Participants
The 4,787 participants had a mean (±SD) age of 66.1 (±7.5) years and included 2,366 (49.4%) men. Men and women differed significantly in almost all characteristics (P ≤ 0.030, Table 1), except for age, serum triglycerides, and history of dyslipidemia. Men, compared with women, had a significantly higher office (133.1/83.4 vs. 130.2/80.0 mm/Hg) and home systolic/diastolic blood pressure (129.4/81.2 vs. 127.0/78.1 mm/Hg).
The median (interquartile range) number of days and readings of home blood pressure measurement was 7 (5–7) and 42 (39–48), respectively. The measurement time was between 06:00 and 08:00 and between 18:00 and 21:00 in the morning and evening, respectively (Supplementary Table 1**).**
Home systolic/diastolic blood pressure decreased from 129.0/80.6 mmHg in the morning to 127.2/78.7 mmHg in the evening by a mean change of −1.9 ± 7.8/−1.8 ± 4.7 mmHg. Home pulse rate increased from 70.5 beats/min in the morning to 73.7 beats/min in the evening by a mean change of +3.1 ± 5.8 beats/min. Home double product increased from 9,093 ± 1,447 in the morning to 9,365 ± 1,499 in the evening by a mean change of 272 ± 832. The morning-to-evening changes in blood pressure tended to be smaller with age advancing in both sexes (Ptrend < 0.001, Figure 1).
Morning-to-evening changes in home blood pressure and pulse rate by sex and age group. Symbols represent the mean value. Vertical lines denote standard error. The number of patients is given for each age subgroup at the bottom of the figure in men and women separately. The P value for trend is also given for men and women separately.
Determinants of the Morning-to-Evening Changes in Home Blood Pressure and Pulse Rate
In univariate analysis, the morning-to-evening changes in blood pressure and pulse rate were associated with several demographic and lifestyle factors and anthropometric and biochemical measurements (Supplementary Table 2). In multiple stepwise linear regression, the morning-to-evening changes in home blood pressure and pulse rate remained associated with most of the determinants identified in the above univariate analysis (Table 2).
Further adding pulse rate in the model for blood pressure did not materially change the associations for the above-identified determinants. However, further adding blood pressure in the model for pulse rate changed the association with male sex, although the associations for all the other above-identified determinants remained unchanged.
Interrelationship Between the Morning-to-Evening Changes in Home Blood Pressure and Pulse Rate
The morning-to-evening changes in home pulse rate were inversely associated with those in home systolic and diastolic blood pressure (r = −0.20 and −0.12, respectively, Figure 2). In the presence of a morning-to-evening decrease in systolic blood pressure, there was an increase in home pulse rate (+5.2 beats/min in men and +4.1 beats/min in women). In the presence of no change or an increase in blood pressure, there was still a smaller increase in home pulse rate in both men (+2.8 beats/min) and women (+1.0 beats/min). After adjustment for the above-identified factors for the morning-to-evening changes in pulse rate, the results were confirmatory.
Relationship between the morning-to-evening changes in home pulse rate and systolic (left panel) and diastolic blood pressure (right panel) by sex. Symbols represent mean value adjusted for age, body mass index, current smoking and alcohol intake, hypertension duration, serum low-density lipoprotein cholesterol, angiotensin receptor blocker use, α-blocker use, and β-blocker use. Vertical lines denote standard error. The P values for trend are given.
Relationship Between Morning-to-Evening Changes in Home Pulse Rate and Office Blood Pressure Control
At baseline, the control rate was lower for office diastolic blood pressure alone (73.9% vs. 81.4%, P < 0.001) and combined office systolic and diastolic blood pressure (60.1% vs. 65.5%, P=<0.001), but not office systolic blood pressure alone (69.6% vs. 71.5%, P = 0.16), in patients with a morning-to-evening change in pulse rate above the median (≥3.0 beats/min) than below the median (<3.0 beats/min, Figure 3).
Office blood pressure control rate at baseline in patients below (filled bar) or above (open bar) the median of the morning-to-evening changes in home pulse rate. The percentage is given along the bars. The P value is also given.
DISCUSSION
The key finding of our study was that there were interrelated morning-to-evening changes in home blood pressure and pulse rate, being on average a drop and rise, respectively. The size of these changes was associated with several demographic and lifestyle factors, and anthropometric and biochemical measurements, and the use of various antihypertensive drugs. In addition, patients with a greater increase in home pulse rate had a poor control status of office blood pressure.
Our observation on the lower blood pressure in the evening than in the morning is in line with the results of several previous studies in Asia^11,12,18–23^ but not those in Europe.^24,25^ Several large-scale studies in Asia, mainly Japan, reported the morning and evening home blood pressure and pulse rate values.^11,12,18–22,26^ In a recent study involving five Japanese general populations (n = 9,801), the mean systolic/diastolic blood pressures were 129.6/77.0 mmHg in the morning and 122.1/70.5 mmHg in the evening by a mean change of −7.5/−6.5 mmHg.^26^ In 3,400 treated patients enrolled in the J-HOME (The Japan Home versus Office Blood Pressure Measurement Evaluation) study, home morning and evening systolic/diastolic blood pressure changed from 139.6/81.7 mmHg in the morning to 133.7/76.9 mmHg in the evening by a mean change of −5.9/−4.8 mmHg.^19^ In 21,569 treated hypertensive patients enrolled in the HONEST (Home BP measurement with Olmesartan Naive patients to Establish Standard Target blood pressure) study, the corresponding values were 151.6/87.1, 150.1/86.6, and −1.5/−0.5 mmHg, respectively.^27^ Several large-scale studies in Europe also reported the morning and evening blood pressure and pulse rate values. In 1919, participants in the Finn-Home general population study, home systolic/diastolic blood pressure changed from 128.1/80.2 mmHg in the morning to 131.1/80.2 mmHg in the evening by a mean change of 3.0/0.0 mmHg.^24^ In 233 untreated hypertensive patients also from Finland, the corresponding values were 137.1/92.4, 140.8/93.4, and 3.7/1.0 mmHg, respectively. It is well-agreed that the measurement time after or before super has played a major role in the differentiation between the two ethnicities in the blood pressure changes from morning to evening.
Our findings on the morning-to-evening changes in home pulse rate may have straightforward explanations. The increase in pulse rate from morning to evening is rather a consequence than a cause of the decrease in blood pressure. Increasing pulse rate probably behaves as a compensating factor for the morning-to-evening drop in blood pressure, directly via increasing cardiac output^28^ and indirectly via various regulatory mechanisms associated with increasing pulse rate, such as the activation of sympathetic nervous system and renin-angiotensin-aldosterone system.^29^ In our present study, there was a possible morning-to evening increase in cardiac output as indicated by the observed slight increase in the double product that was calculated by systolic blood pressure times pulse rate, and can reflect cardiac output.^30,31^ In addition, our study participants were treated with various antihypertensive drugs, which may not only reduce blood pressure but also potentially influence the changes in blood pressure and pulse rate during day, especially β-blockers and ARBs.
The observation that the morning-to-evening changes in both blood pressure and pulse rate were associated with several demographic and lifestyle factors and anthropometric and biochemical measurements suggests that these changes might be related to physical activity, organ damage, decay of the regulatory system, use of various antihypertensive drugs, and so on.^32,33^ For instance, the smaller drop in blood pressure and rise in heart rate associated with older age might be attributable to decreased physical activity. For most of the patients, antihypertensive drugs were taken in the morning, and morning blood pressure and heart rate tended to increase before drug intake. The greater drop in blood pressure and rise in heart rate in patients with a greater BMI and in alcohol drinkers might be attributable to dysregulation of the nervous and hormonal systems.^34–37^ In addition, the morning-to-evening changes in systolic and diastolic blood pressure had similar determinants except that diastolic but not systolic changes were associated with BMI and serum HDL cholesterol. This finding is not entirely understood. It is possible that diastolic blood pressure, which is more reflective of peripheral vascular resistance and less influenced by arterial stiffness than systolic blood pressure,^38,39^ may be more sensitive to metabolic alterations, such as obesity and dyslipidemia.^40,41^
Our new finding on the poor blood pressure control in those patients with a greater increase in home pulse rate from morning to evening is not entirely understood. Because systolic blood pressure is less influenced by pulse rate than diastolic blood pressure, our observation on the stronger association of the morning-to-evening changes in pulse rate with diastolic than systolic blood pressure control might be pathophysiologically relevant.^15,42^ The greater increase in pulse rate from morning to evening, possibly induced by the blood pressure drop, might indicate severer organ damage and cardiovascular dysregulation. Nonetheless, in the Ohasama study, pulse rate in the morning (hazard ratio 1.17, 95% CI: 1.05–1.30) and evening (hazard ratio 1.16, 95% CI: 1.04–1.29) was similarly associated with the risk of cardiovascular mortality.^43^ In addition, in a recent analysis of the Hypertension Objective treatment based on Measurement by Electrical Devices of Blood Pressure (HOMED-BP) study, home pulse rate was superior to office pulse rate as a predictor of all-cause mortality, whether before (hazard ratio 1.52, 95% CI: 1.24–1.92) or after antihypertensive drug treatment (hazard ratio 1.70, 95% CI: 1.70–2.08).^44^ Taken together these previous results, our finding and recent Chinese^45^ and European^46^ guideline recommendations on faster pulse rate as a predictor or risk factor, there is a need of more research on home pulse rate in treated hypertension.
Our study should be interpreted within the context of its strengths and limitations. The same automated blood pressure measuring device was used for the office and home blood pressure measurements. The device difference was therefore minimal. Blood pressure was automatically transmitted to a digital platform. However, our registry was cross-sectional. Second, although a standardized protocol was applied for blood pressure measurement, there was still possible divergence in data collection between hospitals and community health centers. Third, we did not perform autonomic nervous system assessments, such as heart rate variability, which limits our ability to characterize the potential mechanisms underlying the observed compensatory responses to changes in blood pressure.
In conclusion, our cross-sectional study showed that treated Chinese patients with hypertension had interrelated morning-to-evening changes in home blood pressure and pulse rate, being on average a drop and rise, respectively. These changes might be clinically relevant in blood pressure control, and probably in cardiovascular prevention as well.
Supplementary Material
hpaf137_suppl_Supplementary_Materials_1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stergiou GS , Palatini P, Parati G, O’Brien E, Januszewicz A, Lurbe E, Persu A, Mancia G, Kreutz R, European Society of Hypertension C; the European Society of Hypertension Working Group on Blood Pressure M, Cardiovascular V. 2021 European Society of Hypertension practice guidelines for office and out-of-office blood pressure measurement. J Hypertens 2021; 39:1293–1302.33710173 10.1097/HJH.0000000000002843 · doi ↗ · pubmed ↗
- 2Muntner P , Shimbo D, Carey RM, Charleston JB, Gaillard T, Misra S, Myers MG, Ogedegbe G, Schwartz JE, Townsend RR, Urbina EM, Viera AJ, White WB, Wright JT Jr; on behalf of the American Heart Association Council on Hypertension; Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Cardiovascular Radiology and Intervention; Council on Clinical Cardiology; and Council on Quality of Care and Outcomes Research. Measurement of blood pressure in humans: a scienti · doi ↗ · pubmed ↗
- 3Umemura S , Arima H, Arima S, Asayama K, Dohi Y, Hirooka Y, Horio T, Hoshide S, Ikeda S, Ishimitsu T, Ito M, Ito S, Iwashima Y, Kai H, Kamide K, Kanno Y, Kashihara N, Kawano Y, Kikuchi T, Kitamura K, Kitazono T, Kohara K, Kudo M, Kumagai H, Matsumura K, Matsuura H, Miura K, Mukoyama M, Nakamura S, Ohkubo T, Ohya Y, Okura T, Rakugi H, Saitoh S, Shibata H, Shimosawa T, Suzuki H, Takahashi S, Tamura K, Tomiyama H, Tsuchihashi T, Ueda S, Uehara Y, Urata H, Hirawa N. The Japanese Society of Hypertension guidelines for the management of hyperte · doi ↗ · pubmed ↗
- 4Wang JG , Bu PL, Chen LY, Chen X, Chen YY, Cheng WL, Chu SL, Cui ZQ, Dai QY, Feng YQ, Jiang XJ, Jiang YN, Li WH, Li Y, Li Y, Lin JX, Liu J, Mu JJ, Peng YX, Song L, Sun NL, Wang Y, Xi Y, Xie LD, Xue H, Yu J, Yu W, Zhang YQ, Zhu ZM. 2019 Chinese Hypertension League guidelines on home blood pressure monitoring. J Clin Hypertens (Greenwich)2020; 22:378–383.31891454 10.1111/jch.13779 PMC 8029889 · doi ↗ · pubmed ↗
- 5Ward AM , Takahashi O, Stevens R, Heneghan C. Home measurement of blood pressure and cardiovascular disease: systematic review and meta-analysis of prospective studies. J Hypertens 2012; 30:449–456.22241136 10.1097/HJH.0b 013e 32834 e 4aed · doi ↗ · pubmed ↗
- 6Juhanoja EP , Niiranen TJ, Johansson JK, Puukka PJ, Thijs L, Asayama K, Langen VL, Hozawa A, Aparicio LS, Ohkubo T, Tsuji I, Imai Y, Stergiou GS, Jula AM, Staessen JA; International Database on Home Blood Pressure in Relation to Cardiovascular Outcome (IDHOCO) Investigators. Outcome-driven thresholds for increased home blood pressure variability. Hypertension 2017; 69:599–607.28193705 10.1161/HYPERTENSIONAHA.116.08603 · doi ↗ · pubmed ↗
- 7Guo QH , Cheng YB, Zhang DY, Wang Y, Huang QF, Sheng CS, Xu TY, Li Y, Wang JG. Comparison between home and ambulatory morning blood pressure and morning hypertension in their reproducibility and associations with vascular injury. Hypertension 2019; 74:137–144.31104566 10.1161/HYPERTENSIONAHA.119.12955 · doi ↗ · pubmed ↗
- 8Kario K , Hasebe N, Okumura K, Yamashita T, Akao M, Atarashi H, Ikeda T, Koretsune Y, Shimizu W, Suzuki S, Tsutsui H, Toyoda K, Hirayama A, Yasaka M, Yamaguchi T, Teramukai S, Kimura T, Morishima Y, Takita A, Inoue H. Home blood pressure can predict the risk for stroke/bleeding events in elderly patients with nonvalvular atrial fibrillation from the ANAFIE registry. Hypertension 2022; 79:2696–2705.36259381 10.1161/HYPERTENSIONAHA.122.19810 PMC 9640260 · doi ↗ · pubmed ↗