Management of a Foreign Body in the Throat: Should Awareness of Channelled Flexible Nasendoscopes Be Encouraged Among Junior ENT Doctors?
Siddharth Kotikalapudi, Atanu Maity, Amro Hassaan

TL;DR
A case study shows that using a flexible nasendoscope with a working channel can help remove throat foreign bodies without general anesthesia, potentially reducing risks and costs.
Contribution
Demonstrates the potential utility of channeled flexible nasendoscopes in foreign body removal by junior ENT doctors, suggesting a need for broader training.
Findings
A fish bone was successfully removed using a channeled flexible nasendoscope without general anesthesia.
The patient was discharged the same day with no complications.
The case highlights the potential for reducing GA use and hospital admissions with this technique.
Abstract
Ingested foreign bodies in the upper aero-digestive tract are a common ENT emergency. Initial assessment and management by a junior ENT doctor involves removal of the foreign body under direct visualisation, with escalation to removal under general anaesthesia (GA) if unsuccessful. However, removal under general GA carries procedural risks, anaesthetic risks, and a higher cost profile. An adult female presented to our unit with a fish bone lodged in the right pyriform fossa. Initial removal with instruments and direct visualisation with a flexible nasendoscope (without a working channel) was attempted but was unsuccessful. She was scheduled for removal under GA. At morning handover, an alternative approach was suggested (a method not routinely familiar to the on-call junior doctor team) and trialled using a single-use flexible nasendoscope with a working channel. Following topical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
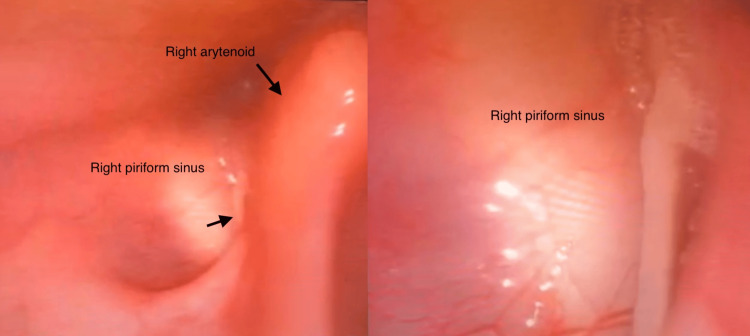 Figure 1
Figure 1 Figure 2
Figure 2| Factor | GA retrieval | Single-use flexible endoscope retrieval |
| Theatre cost | £840–£1,260 (60–90 minutes) | N/A |
| Admission cost | £350–£587 per day (pre/postoperative + overnight stay) | Admission normally not required |
| Equipment cost | A reusable rigid scope which requires reprocessing and potential repair can lead to high life cycle costs (£104.92 to £209.84 per endoscope) [ | £179 (excluding VAT). Single use biopsy forceps: £9.22–12.50 (variable between different manufactures) |
| Anaesthesia risk | Complications from GA are applicable | N/A; only a local anaesthetic is used |
| Staffing demands | All theatre staff (anaesthetist surgeon, scrub nurse, ODP, etc.) | ENT specialist and an assistant |
| Recovery time | Monitoring after GA, admission, and monitoring | Same-day discharge |
| Cross-contamination risk | Present in reusable scopes | None present in single-use scopes |
| Scenario | FNE cost (£) | GA total cost (£) | Savings (£) |
| FNE success – lower estimate | 191.50 | 1,190.50 | 998.50 |
| FNE success – upper estimate | 191.50 | 1,847 | 1,655.50 |
| FNE failure → GA | 191.50 + GA cost (1,190.5/1,847) | 1,190.50–1,847 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Airway Management and Intubation Techniques · Restraint-Related Deaths
Introduction
Ingested foreign bodies within the upper aero-digestive tract are a common ENT emergency presentation, accounting for up to 20% of ENT emergency presentations [1]. In the adult population, fish bones account for a large proportion of these presentations [2]. Emergency referrals are commonly managed by a junior ENT doctor of varying experience; as a result, an unnecessary number of patients are examined under general anaesthesia, with a reported 20% of patients undergoing a theatre procedure where no foreign body is found [1]. Initial management, after it is deemed that there are no airway concerns, is the removal of the foreign body under direct visualisation (single-use flexible endoscope with no working channel). Failure of this method results in escalation for removal of the foreign body under general anaesthesia (GA), which inherently carries its own set of risks [3]. This case study highlights the importance of awareness of a flexible endoscopy with a working channel to remove the foreign body.
Case presentation
Presentation
A patient had presented overnight with a sensation of a foreign body in her throat, after having dinner involving fish. Upon initial assessment and examination, she was found to be able to eat and drink and did not have any difficulty in breathing. However, she reported a stinging sensation within her throat whenever she swallowed and felt it localise to the right side of her neck (level 2/3). She presented to her local A&E within an hour of the initial onset of these symptoms.
There were no immediate concerns for an airway emergency, and the remaining vital signs were normal (SpO_2_, 98%; unremarkable respiratory rate, heart rate, and blood pressure). A flexible nasendoscopy was performed, which visualised a fish bone within the right piriform fossa (see Figure 1) and removal was attempted under direct visualisation by the on-call SHO. However, this was unsuccessful as the fish bone was small (roughly 2 cm) and was in an unfavourable position for removal with Tilley’s or Dennis-Brown forceps under direct visualisation. The patient’s case was discussed with the on-call registrar, who had advised admission and removal under GA in the emergency theatre on the next day.
Fish bone in the right pyriform fossa.(a) View of the fish bone from a distance. (b) A close-up view of the fish bone.
Management
This presentation was discussed during our morning meeting, and a decision was made by the on-call ENT consultant to attempt removal under direct visualisation again. However, we used a flexible nasendoscope (AmbuScope) with an accessory channel, which would allow for the introduction of biopsy forceps. The larger nasendoscope was introduced after instilling a co-phenylcaine spray via the nostrils. However, despite the local anaesthetic, the larger scope was proving to be difficult to pass through the nasal passage as the patient found this to be quite uncomfortable (complaining of pain, rated 5/10). The scope was alternatively passed via the oral cavity (after further sprays of co-phenylcaine), which the patient was able to tolerate better, and the foreign body was identified in the right pyriform fossa. Biopsy forceps were then introduced via the accessory channel, and the fish bone was removed. The length of the procedure was approximately 20-25 minutes, and she was observed for a further hour until the effects of the spray had worn off. She was monitored for airway compromise, bleeding, or persistent discomfort, and no deterioration was noted during this observation period. She was discharged home with safety netting for any symptoms suggestive of complications. The patient was further followed up with a telephone appointment to discuss her aftercare and return to normal life. She did not report any complications and reported that she returned to her usual routine on the same day, although she voiced that she was cautious of eating fish. Thus, an examination under GA was prevented, and the patient did not require an extended stay in the hospital.
Discussion
Fish bones are a common ingested foreign body in adults, particularly in populations with high fish consumption [4]. Complications occur when a lodged fish bone or sharp fragment becomes impacted, potentially leading to infection, ulceration, or perforation. In rare cases, patients can present with a retropharyngeal abscess or mediastinitis, which carries significant morbidity and mortality [5].
Initial assessment of a patient with a suspected foreign body in the throat involves excluding airway compromise. Once a safe airway is confirmed, flexible nasendoscopy is the most reliable modality to confirm the presence of a foreign body [6], as radiographs often lack sufficient sensitivity for radiolucent fish bones [7,8]. If a foreign body is not identified on flexible nasendoscopy or radiographs, and symptoms persist, CT imaging of the neck is warranted.
If initial removal attempts fail, a further attempt using a larger endoscope with an accessory channel may be considered. This approach can prevent hospital admission and avoid examination under GA with rigid oesophagoscopy or laryngoscopy, which carry inherent risks, including mucosal tears, bleeding, oesophageal perforation, and mediastinitis [9]. Additional risks include perioperative complications and prolonged recovery, particularly in comorbid or elderly patients [9]. Anaesthetic risks, such as airway manipulation, intubation complications, and drug-related adverse effects, must also be considered, with rarer risks including laryngospasm, aspiration, or difficult intubation [10,11].
Existing evidence supports flexible endoscopy as an effective alternative to rigid endoscopy. A meta-analysis of 1,402 patients reported equivalent success rates for flexible endoscopy and rigid endoscopy (pooled odds ratio (OR) = 1.00, 95% confidence interval (CI) = 0.48-2.06), with low overall complication rates; the pooled estimate suggested a higher, though not statistically significant, risk of perforation with rigid endoscopy [9]. These data suggest that flexible endoscopy with appropriate instrumentation may serve as a safe and cost-effective first-line or intermediate approach in selected patients, potentially avoiding GA in many cases. However, as the meta-analysis primarily evaluated oesophageal impactions, extrapolation to pharyngeal or hypopharyngeal foreign bodies must be done cautiously. There remains a lack of direct comparative data between rigid and flexible techniques for pharyngeal or hypopharyngeal retrievals, and current clinical guidelines do not differentiate between standard flexible nasendoscopy and larger flexible nasendoscopy with a working channel [12]. This underscores the need for further research and structured evaluation of flexible endoscopy in these anatomical regions.
Patients undergoing foreign body retrieval under local anaesthetic generally do not require extended observation or hospital admission. Procedures are typically less invasive, with lower risk profiles, and patients can often be discharged on the same day with appropriate safety netting [9-11]. Nonetheless, without larger series or control groups, these benefits remain observational.
Flexible endoscopy with a working channel does require at least two experienced clinicians. Patient discomfort during transnasal endoscopy may reduce cooperation and success rates, and adequate topical anaesthesia may not fully alleviate this [13,14]. In our case, passing the endoscope orally was trialled and was successful; however, this is less common and should be undertaken only by experienced clinicians. Current literature on transoral applications of single-use Ambu® aScope™ devices is limited, indicating a need for further research and clinical evaluation before widespread adoption.
This approach is unsuitable for foreign bodies that have passed into the oesophagus, which typically require GA and rigid endoscopy. Success also depends on patient tolerance, anatomical factors such as narrow nasal passages, and the size of the foreign body. In these scenarios, escalation to GA remains the safest approach.
The cost-benefit analysis of foreign body retrieval under local anaesthesia compared to foreign body retrieval under GA must be considered. The unit price of a single-use endoscope with a working channel is £179 (excluding VAT) [15] and can avoid admission or an overnight stay in the hospital, if the procedure is successful. It also avoids assessment and workup from the anaesthetic team and theatre occupation, which allows for other urgent presentations that require GA and eliminates reprocessing, repair, and cross-contamination risk of space and equipment [14]. Table 1 presents a comparison of the benefits and risks associated with the removal under GA and removal with a single-use endoscope.
Direct costs of admission for removal of foreign body under general anaesthesia are as follows: (1) these cases are often booked for a typical theatre time of 60-90 minutes (including anaesthetic time, setup, and turnover); the cost would range from £840-1,260 (£14/minute) [16,17]; (2) the cost of admission into hospital, including pre- and postoperative waiting time: £350-£587 per day [18,19]; and (3) displacement of other emergency cases, which can have large system costs [16]. Figure 2 presents a representative image of the single-use Ambu® aScope™ device.
Ambu A/S (Ambu® aScope™ 4 RhinoLaryngo Intervention).Image courtesy of Ambu A/S. Used in accordance with Ambu’s media policy [19].
Therefore, any case that occupies the theatre for more than 13 minutes has a higher cost than the use of a single-use channelled scope. Therefore, savings per successful removal with a single-use endoscope can range from £998.50 to £1,655.50 (Table 2).
Case selection is vital in these presentations as in patients with airway compromise, foreign bodies in unfavourable positions (such as oesophagus) will likely require GA and rigid endoscopy [1,4]. The use of single-use endoscopes for retrieval in these cases is unsafe and can double the costs when they are required to go to the theatre. The cost analysis from this case study suggests that a successful retrieval with a flexible endoscope can be economically beneficial, but these estimates assume procedural success. Failed attempts requiring escalation will double the costs. A sensitivity analysis and an audit of larger case series are needed to validate the cost-effectiveness.
Systemic limitations affect the potential adoption of using channelled flexible endoscopes among junior doctors. Lack of access and knowledge of the equipment affects junior doctors’ confidence and competency in challenging endoscopic manipulation. Limited training and access may increase failed attempts, leading to GA escalation and higher risk and cost. Implementing structured training programs for junior ENT doctors can enhance proficiency in flexible endoscopy techniques and increase awareness of the different types of endoscopes available. Regular audits of procedural outcomes, once these techniques are in routine use, will help identify areas for improvement and ensure appropriate and effective application. However, there is currently a lack of national survey data assessing junior doctors’ familiarity and use of working-channel flexible endoscopes. Robust national data are required to inform the need and design of future training programmes.
Conclusions
This case study helps illustrate that a working-channel flexible endoscopy can be used to safely retrieve foreign bodies under topical anaesthesia. Examination under anaesthesia, admission, and retrieval of the foreign body in controlled settings, such as a theatre, can be avoided. However, as a single-case observation, the findings cannot be extrapolated. Success depends on patient selection, anatomical considerations, and clinician familiarity with such techniques. This highlights the potential value of structured training programs, competency assessments, and regular audits for junior doctors. Further prospective studies and cost-benefit analysis are warranted to guide broader adoption and protocol development. Current literature comparing flexible and rigid endoscopy removal specifically in the pharynx or hypo-pharynx is limited, and current guidelines do not differentiate between standard and working-channel flexible nasendoscopy, which raises the question of whether they should be differentiated in future guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The management of foreign bodies in the pharynx and oesophagus using transnasal flexible laryngooesophagoscopy (TNFLO)Ann R Coll Surg Engl Bennett A Sharma A Price T Montgomery P 1316902008 https://pmc.ncbi.nlm.nih.gov/articles/PMC 2216707/1820149110.1308/003588408 X 242114 PMC 2216707 · doi ↗ · pubmed ↗
- 2Fish bone foreign body: the role of imaging Int Arch Otorhinolaryngol Klein A Ovnat-Tamir S Marom T Gluck O Rabinovics N Shemesh S 110115232019 https://pubmed.ncbi.nlm.nih.gov/30647794/3064779410.1055/s-0038-1673631 PMC 6331292 · doi ↗ · pubmed ↗
- 3Removal of foreign-bodies under general anaesthesia. A review of rigid endoscopy for foreign-bodies of the hypopharynx and oesophagus Med J Malaysia Revadi G Philip R Gurdeep S 143145652010 https://www.e-mjm.org/2010/v 65n 2/Rigid_Oesophagoscopy.pdf 23756800 · pubmed ↗
- 4Clinical presentation, diagnosis and management of aerodigestive tract foreign bodies in the adult population: part 1SA J Radiol Mathew RP Sarasamma S Jose M Toms A Jayaram V Patel V Low G 2022252021 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 8063768/3393679410.4102/sajr.v 25i 1.2022 PMC 8063768 · doi ↗ · pubmed ↗
- 5Fish bone migration: complications, diagnostic challenges, and treatment strategies World J Emerg Surg Li D Zeng W Chen J 35202025 https://wjes.biomedcentral.com/articles/10.1186/s 13017-025-00611-94026993910.1186/s 13017-025-00611-9PMC 12016485 · doi ↗ · pubmed ↗
- 6Investigative strategies for fish bone foreign bodies during the coronavirus disease 2019 pandemic: an analysis of ENT UK guidelines J Laryngol Otol Michaels J Orji C Green F Nogueira C 2502541352021 https://pubmed.ncbi.nlm.nih.gov/33632367/3363236710.1017/S 0022215121000669 PMC 7948105 · doi ↗ · pubmed ↗
- 7Our experience of fish bone foreign bodies in the upper aerodigestive tract: diagnostic indicators and examination modalities Aust J Otolaryngol Rankin A Dhambagolla I Johnston J Vokes D 2082025 https://www.theajo.com/article/view/4925/html
- 8Fish bone as a foreign body J Laryngol Otol Kumar M Joseph G Kumar S Clayton M 5685691172003 https://pubmed.ncbi.nlm.nih.gov/12901817/1290181710.1258/002221503322113058 · doi ↗ · pubmed ↗