Adjuvant treatment preferences in high-risk upper tract urothelial carcinoma: the perspective of Portuguese medical oncologists
Guilherme Vilhais, Mário Fontes-Sousa

TL;DR
Portuguese medical oncologists prefer platinum-based chemotherapy for high-risk upper tract urothelial carcinoma, even when PD-L1 status varies.
Contribution
This study reveals adjuvant treatment preferences of Portuguese oncologists for high-risk UTUC based on PD-L1 status and cisplatin eligibility.
Findings
Cisplatin plus gemcitabine is the preferred regimen for cisplatin-eligible patients regardless of PD-L1 status.
In cisplatin-ineligible PD-L1-positive patients, carboplatin plus gemcitabine is preferred over immune checkpoint inhibitors.
Preferences reflect reliance on UTUC-specific evidence and limited perceived benefit from ICIs in this subgroup.
Abstract
Although upper tract urothelial carcinoma (UTUC) and bladder urothelial carcinoma (BUC) share histological features, they differ in clinical behavior and management. Valid adjuvant options include surveillance, platinum-based chemotherapy, and immune checkpoint inhibitors (ICIs). To assess real-world practice, we conducted a survey among Portuguese medical oncologists dedicated to genitourinary malignancies, exploring their preferences for adjuvant therapy in high-risk UTUC (illustrated as pT2N1M0) across three clinical scenarios that differed by PD-L1 status and renal function. Among 34 respondents, cisplatin plus gemcitabine was the preferred regimen in cisplatin-eligible patients, regardless of PD-L1 status (94% in PD-L1-negative and 85% in PD-L1-positive tumors). In PD-L1-positive, cisplatin-ineligible patients, carboplatin plus gemcitabine was preferred (47%), followed by ICIs…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
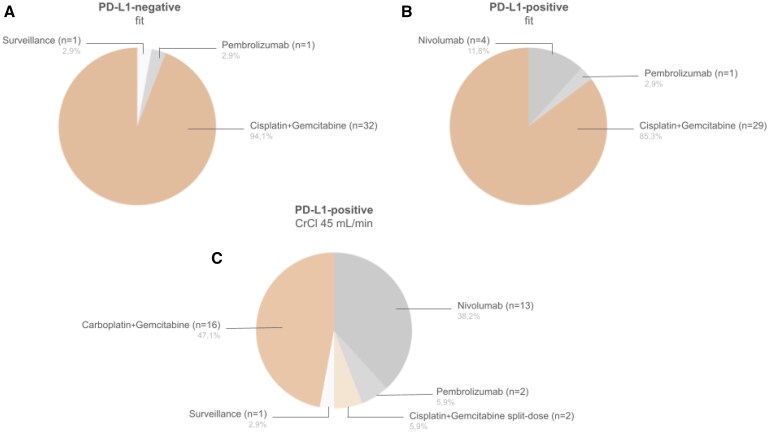 Figure 1
Figure 1| Trial | Intervention/Comparator | Population | UTUC % | Primary endpoint(s) | DFS in ITT | DFS in UTUC | OS |
|---|---|---|---|---|---|---|---|
|
| Platinum ChT vs. Observation | pT2-pT4 and/or pN+ | 100 | DFS | HR = 0.45, 95% CI 0.30-0.68; | same as ITT |
HR = 0.68; 95% CI: 0.46-1.00; |
|
| Atezolizumab vs. Observation |
ypT2-T4 and/or ypN+ pT3-T4 and/or pN+ | 7 | DFS | HR = 0.89, 95% CI 0.74-1.08; | HR = 1.25, 95% CI 0.57-2.74 |
HR 0.91, 95% CI 0.73-1.13 |
|
| Nivolumab vs. Placebo |
ypT2-T4a and/or ypN+ pT3-T4a and/or pN+ | 21 |
DFS in ITT population DFS in PD-L1 ≥ 1% |
HR = 0.70, 98.22% CI 0.55-0.90; HR = 0.55, 98.72% CI 0.35-0.85; |
HR = 1.23, 95% CI 0.67-2.23
HR = 1.56, 95% CI 0.70-3.48 |
HR 0.76, 95% CI 0.61-0.96 HR 0.56, 95% CI 0.36-0.86 |
|
| Pembrolizumab vs. Observation |
≥ypT2 and/or ypN+ and/or R1 ≥pT3 or N+ and/or R1 | 21.9 |
DFS OS | HR = 0.73, 95% CI 0.59-0.90; |
HR = 1.96, 95% CI 0.92-4.17
HR = 1.56, 95% CI 0.77-2.02 |
HR = 0.98, 95% CI 0.76-1.26 |
- —CUF Academic Center
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Renal cell carcinoma treatment · Cancer Immunotherapy and Biomarkers
Background
Upper tract urothelial carcinomas (UTUC) are uncommon malignancies of the renal pelvis or ureter, with an estimated incidence of approximately 2 cases per 100 000 individuals annually.1 Although UTUC and Bladder Urothelial Carcinoma (BUC) share histological features, they differ significantly in their epidemiological, clinical, pathological, and molecular profiles.2^,^3 Unlike BUC, where neoadjuvant systemic therapy is the standard of care, neoadjuvant treatment is generally not the preferred approach in UTUC due to lacking prospective data, emphasizing the importance of adjuvant strategies.4
Given that 90%-95% of urothelial carcinomas (UC) originate in the bladder, most pivotal clinical trials that granted treatment approvals have included few UTUC patients, and treatment recommendations are frequently extrapolated from BUC evidence.
The POUT trial remains the only phase III randomized study specifically designed for UTUC.5 In this trial, 261 patients with high-risk UTUC post-radical nephroureterectomy (RNU) were randomized to receive adjuvant platinum-based chemotherapy (ChT) or surveillance. A statistically significant improvement in disease-free survival (DFS), the primary endpoint, was observed in the ChT arm (Table 1). Importantly, the benefit was fairly consistent across subgroups, including those receiving carboplatin+gemcitabine—a relevant finding, given the reduced cisplatin eligibility post-RNU. Although not adequately powered for Overall Survival (OS) analysis, a positive trend was observed.6
Given the success of immune checkpoint inhibitors (ICIs) in metastatic BUC, their efficacy has also been assessed in the adjuvant setting. The phase III CheckMate 274 trial randomized 709 patients with high-risk UC following radical surgery to receive adjuvant nivolumab or placebo for 1 year.7 The trial met its dual primary endpoints, demonstrating a DFS benefit in the intention-to-treat population and in patients with PD-L1 expression ≥1%. Nivolumab was subsequently approved in this setting by the European Medicines Agency for PD-L1 positive tumors and the U.S. Food and Drug Administration, regardless of PD-L1 status. UTUC patients comprised 21% of the study population—higher than typically observed—but subgroup analysis suggested limited benefit compared to BUC (Table 1).
The AMBASSADOR (KEYNOTE-123) trial randomized 739 patients with high-risk UC to receive adjuvant pembrolizumab for 1 year or observation.8 DFS was improved in the pembrolizumab arm, independently of PD-L1 expression. Final OS data are pending, but preliminary analyses have not shown a clear benefit. Of note, the approval of nivolumab during trial enrollment may have led to treatment crossover, potentially confounding OS interpretation. This trial also included 21.9% UTUC patients, and, as with CheckMate 274, subgroup analysis did not indicate a significant benefit in this subgroup (Table 1).
Atezolizumab was also evaluated in this setting, but the trial did not meet its primary endpoint of improved DFS (Table 1).9
Current evidence highlights the uncertainty surrounding the optimal adjuvant approach in high-risk localized UTUC, which accounts for approximately 40%-50% of all patients with UTUC.10 Platinum-based ChT demonstrated a DFS benefit (and OS trend) in a UTUC-specific trial, whereas ICIs showed a DFS benefit (and OS with nivolumab) in broader UC populations that appears to be driven primarily by BUC. The reasons behind the apparently reduced benefit of ICIs in UTUC remain unclear, despite the higher prevalence of Lynch syndrome and microsatellite instability-high (MSI-H) tumors in UTUC, which are generally predictive of ICI responsiveness.
Real-world survey results and discussion
In order to explore current clinical practice preferences, we conducted a national real-world anonymous survey (Supplement 1) among Portuguese medical oncologists dedicated to genitourinary malignancies. Of 50 personally invited oncologists, 34 responded (68%), with balanced geographic representation and predominant practice in public institutions. Most respondents (67.6%) had been practicing medical oncology for fewer than 10 years, likely reflecting the national oncology workforce; however, potential selection bias cannot be excluded. Regarding UTUC caseload, 41.2% reported treating more than 5 patients with localized UTUC annually, 44.1% reported treating 3-5, and 14.7% fewer than 3, representing a substantial proportion of the national UTUC incidence (Table S1).
As neoadjuvant chemotherapy (NAC) may influence subsequent adjuvant strategies, respondents were first asked about its role. A majority (58.8%) considered NAC appropriate in selected cases, while 32.4% reported NAC as their preferred approach, likely reflecting concerns regarding post-RNU cisplatin ineligibility. A minority (8.8%) never considers NAC appropriate, possibly due to the lack of prospective data.
Three clinical scenarios were presented, all involving high-risk UTUC (illustrated as pT2pN1M0) R0, of the renal pelvis post-RNU, and therefore eligible for POUT, CheckMate 274, and AMBASSADOR trials (Figure 1). They were then asked to select the most appropriate adjuvant strategy based on available evidence, irrespective of regulatory approvals. The scenarios varied by PD-L1 status and renal function:
Selected adjuvant strategies in high-risk localized UTUC for each clinical scenario by Portuguese medical oncologists that responded to the real-world survey. CrCl, creatinine clearance; PD-L1, programmed death ligand 1.
Case 1: PD-L1 negative, fit (no comorbidities) Case 2: PD-L1 positive, fit (no comorbidities) Case 3: PD-L1 positive, creatinine clearance (CrCl) 45 mL/min
Treatment options included surveillance, cisplatin+gemcitabine (with split-dose for case 3), carboplatin+gemcitabine, nivolumab and pembrolizumab.
In case 1, 94.1% selected cisplatin+gemcitabine as their preferred adjuvant choice, decreasing to 85.3% in case 2 (Figure 1A and B). In case 3, carboplatin+gemcitabine was slightly preferred (47.1%) over ICIs (44.1%), with only 5.9% choosing split-dose cisplatin (Figure 1C). These results suggest that platinum-based ChT remains the preferred adjuvant treatment, even in PD-L1-positive patients. In cisplatin-ineligible patients (CrCl < 60 mL/min),11 carboplatin+gemcitabine was slightly favored over ICIs, possibly reflecting awareness of the POUT subgroup data and the inconclusive benefit of ICIs in UTUC-specific subgroups. We attribute the low preference for split-dose cisplatin to the fact that it was not permitted in the POUT trial. This strategy was recently validated in UC in the NIAGARA trial (CrCl ≥ 40 mL/min); however, the trial did not include UTUC patients.12
Future directions
This survey highlights that respondent physicians tend to prioritize evidence from trials conducted specifically in UTUC, with platinum-based ChT remaining the mainstay adjuvant therapy, as recommended by guidelines.4 Choice of ICIs appears to be predominantly considered for PD-L1-positive cisplatin-ineligible patients.
Importantly, 97.1% of respondents indicated willingness to enroll patients in a randomized trial comparing adjuvant ChT to ICI monotherapy in high-risk localized UTUC. Such a trial could address whether UTUC are intrinsically less responsive to ICIs, and help identify subgroups (eg, MSI-H or Lynch syndrome) more likely to benefit. Future studies could also help define future lines of research/clinical trial development, namely with newer treatment combination regimens (eg, ICI+Antibody Drug Conjugate), as well as in selecting the most appropriate comparators and potentially identifying biomarkers for treatment selection.
Supplementary Material
oyaf365_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Siegel RL , Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7-33.35020204 10.3322/caac.21708 · doi ↗ · pubmed ↗
- 2Green DA , Rink M, Xylinas E, et al Urothelial carcinoma of the bladder and the upper tract: disparate twins. J Urol. 2013;189:1214-1221.23023150 10.1016/j.juro.2012.05.079 · doi ↗ · pubmed ↗
- 3Lefort F , Rhanine Y, Larroquette M, et al Clinical and biological differences between upper tract carcinoma and bladder urothelial cancer, including implications for clinical practice. Cancers (Basel). 2023;15:5558.38067262 10.3390/cancers 15235558 PMC 10705302 · doi ↗ · pubmed ↗
- 4Powles T , Bellmunt J, Comperat E, et al Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022;33:244-258.34861372 10.1016/j.annonc.2021.11.012 · doi ↗ · pubmed ↗
- 5Birtle A , Johnson M, Chester J, et al Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): a phase 3, open-label, randomised controlled trial. Lancet. 2020;395:1268-1277.32145825 10.1016/S 0140-6736(20)30415-3PMC 7181180 · doi ↗ · pubmed ↗
- 6Birtle AJ , Jones R, Chester J, et al Improved disease-free survival with adjuvant chemotherapy after nephroureterectomy for upper tract urothelial cancer: final results of the POUT trial. J Clin Oncol. 2024;42:1466-1471.38350047 10.1200/JCO.23.01659 PMC 11095877 · doi ↗ · pubmed ↗
- 7Bajorin DF , Witjes JA, Gschwend JE, et al Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384:2102-2114.34077643 10.1056/NEJ Moa 2034442 PMC 8215888 · doi ↗ · pubmed ↗
- 8Apolo AB , Ballman KV, Sonpavde GP, et al; Alliance for Clinical Trials in Oncology. AMBASSADOR Alliance A 031501: Phase III randomized adjuvant study of pembrolizumab in muscle-invasive and locally advanced urothelial carcinoma (MIUC) vs observation. JCO. 2024;42:LBA 531-LBA 531.