Shaping Breast Cancer Treatment in Resource-Limited Settings: Influence of AMAROS and ACOSOG Z0011 Trials in a Follow-up Audit
Ammarah Afzal, Muhammad H Nasrullah, Farooq A Rana, Muhammad Saud Iqbal, Najam Us Sahar Hasan, Muhammmad Jawad Haider

TL;DR
This study examines how breast cancer treatment practices have evolved in a resource-limited setting following influential clinical trials.
Contribution
It shows increased adoption of less invasive surgeries and guideline-aligned practices despite limited resources.
Findings
Early-stage diagnoses increased from 14.2% to 27.9% over the study period.
Breast-conserving surgery rose from 6% to 20.3% between 2022 and 2024.
AMAROS and ACOSOG Z0011 guidelines influenced reduced use of axillary lymph node dissection in early-stage cases.
Abstract
Introduction Trials like AMAROS and ACOSOG Z0011 have modified the approach to sentinel lymph node biopsy (SLNB) in node-positive and node-negative breast cancer. This study evaluates evolving surgical trends in breast cancer management at a resource-limited setting with respect to such trials. Methods A follow-up retrospective audit of breast cancer surgeries performed over a three-year period was conducted and compared with the first cycle of audit in the 2017-2021 period. Formal approval was taken from the Ethical Review Board (ERB) of Allama Iqbal Medical College/Jinnah Hospital, Lahore, in its 179th meeting, dated 23-12-2024, with Ref No: ERB179/5(i)/23-12-2024/S1 ERB. Operative records of 273 breast cancer patients treated between 2022 and 2024 were reviewed. Data on age, stage at presentation, and type of surgery were extracted. Surgical procedures included modified radical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
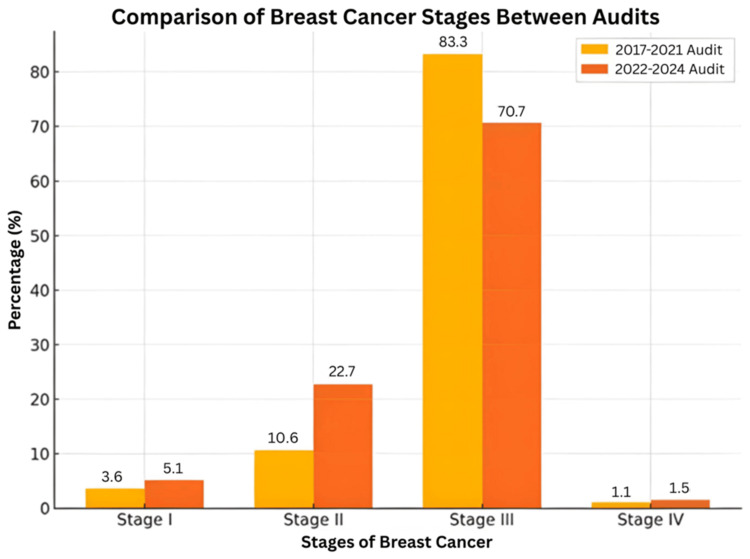 Figure 1
Figure 1 Figure 2
Figure 2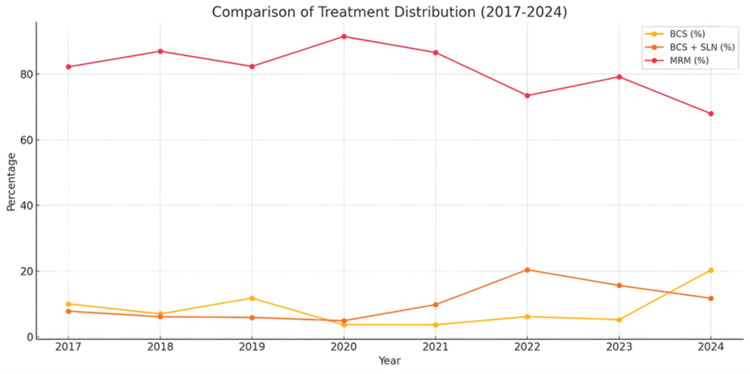 Figure 3
Figure 3| Age (years) | I | II | III | IV | Total |
| <30 | 3 | 18 | 14 | 1 | 36 |
| 31-40 | 5 | 13 | 33 | 3 | 54 |
| 41-50 | 3 | 14 | 64 | 1 | 82 |
| 51-60 | 3 | 10 | 58 | 2 | 72 |
| ≥61 | 0 | 7 | 24 | 0 | 31 |
| Total | 14 | 62 | 193 | 7 | 273 |
| STAGE | BCS¹ | BCS + SLN² | MRM | Total | |
| Axillary Clearance Done | Axillary Clearance Not Done | ||||
| I | 10 | 3 | 1 | 0 | 14 |
| II | 24 | 25 | 11 | 1 | 61 |
| III | 0 | 0 | 0 | 191 | 191 |
| IV | 0 | 0 | 0 | 7 | 7 |
| Total | 34 | 28 | 12 | 199 | 273 |
| Year | Treatment Given | Total | ||
| BCS | BCS + SLN | MRM | ||
| 2022 | 3 | 10 | 36 | 49 |
| 2023 | 5 | 15 | 76 | 96 |
| 2024 | 26 | 15 | 87 | 128 |
| Total | 34 | 40 | 199 | 273 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · Breast Cancer Treatment Studies · Cancer Genomics and Diagnostics
Introduction
Breast cancer remains a major global health challenge, representing the most commonly diagnosed cancer among women and a leading cause of cancer-related mortality. In 2020, approximately 2.3 million new cases and over 685,000 deaths were reported worldwide [1]. Despite medical advancements, significant disparities persist, with nearly 80% of breast cancer-related deaths occurring in low- and middle-income countries (LMICs), primarily due to limited healthcare infrastructure and delays in diagnosis and treatment [2].
While high-income regions have seen increasing breast cancer prevalence, they have also benefited from declining age-standardized mortality rates, largely attributed to improvements in early detection, screening programs, and evolving therapeutic approaches [3]. In contrast, many low-resource settings continue to rely on modified radical mastectomy (MRM) as the mainstay of treatment, often followed by chest wall and regional nodal irradiation [4]. When feasible, breast-conserving surgery (BCS) with negative margins and acceptable cosmetic outcomes should be considered, followed by adjuvant radiotherapy [5]. In this context, periodic institutional audits play a crucial role in evaluating not only treatment patterns but also the degree of progression toward internationally endorsed guideline-based practices.
Over recent decades, management strategies for early-stage breast cancer have increasingly shifted toward less radical and more individualized treatment. Landmark trials such as AMAROS [6] and ACOSOG Z0011 [7] have significantly influenced this paradigm shift, particularly regarding axillary management. The AMAROS trial [6] demonstrated that axillary radiotherapy offers comparable regional control and survival outcomes to axillary dissection, with a lower risk of complications such as lymphedema. Similarly, the ACOSOG Z0011 trial [7] established the safety of omitting axillary lymph node dissection (ALND) in selected patients undergoing BCS, provided only limited sentinel lymph node (SLN) involvement is detected.
Subsequent cohorts have supported these findings, reporting that omitting ALND in patients with ≤2 positive sentinel nodes is both safe and associated with fewer complications, including reduced lymphedema and better arm mobility. The decision to omit ALND may be guided by individual risk profiles, with or without the addition of axillary radiotherapy (ART) [8].
This study aims to conduct a retrospective audit of breast cancer surgeries performed at Jinnah Hospital, Lahore, Pakistan, and compare the findings with a prior audit conducted between 2017 and 2021 [9]. The objective is to assess surgical trends, adherence to evidence-based guidelines, and the influence of institutional practices and resource limitations on treatment decisions. By analyzing three years of surgical data, the study seeks to identify areas of progress and gaps in care, with the goal of informing future strategies for optimizing breast cancer management in resource-constrained environments.
Materials and methods
A retrospective follow-up study was conducted across all four surgical units of the Department of Surgery at Jinnah Hospital, Lahore, Pakistan. Ethical approval was obtained from the Ethical Review Board (ERB) of Allama Iqbal Medical College / Jinnah Hospital, Lahore, in its 179th meeting held on December 23, 2024 (Ref No: ERB179/5(i)/23-12-2024/S1 ERB).
The study included operative records of breast cancer patients treated surgically between January 1, 2022, and November 1, 2024. All patients with a confirmed diagnosis of breast cancer who underwent surgical intervention during this period were included, regardless of age or clinical stage at presentation. Exclusion criteria comprised incomplete medical or operative records and any history of prior breast surgery before the index admission. This audit involved retrospective analysis of anonymized data. In accordance with institutional ethics policy, no identifiable patient information was used. The Institutional Review Board granted a waiver of individual informed consent due to the non-interventional nature of the study.
Data collection was carried out through manual review of patient records by two trained audit team members over a three-month period, from December 23, 2024, to March 14, 2025. A standardized proforma was used to extract data from the operation theatre registry, supplemented by information retrieved through the hospital’s electronic medical record system (HMIS).
A consecutive sampling technique was employed, whereby all eligible cases within the specified time frame were included. The variables collected included patient age, gender, year of presentation, clinical stage of breast cancer (as documented in medical records), and the type of surgery performed such as MRM, BCS, or sentinel lymph node biopsy (SLNB) with or without ALND. These specific data points were selected as they directly reflect surgical decision-making patterns and guideline adherence, which were the primary quality indicators defined for this audit cycle.
Data were entered and analyzed using IBM SPSS Statistics for Windows, Version 27 (Released 2020; IBM Corp., Armonk, New York, United States). Descriptive statistics were used to summarize demographic and treatment-related variables. Chi-square tests were applied to assess differences in stage distribution and treatment modalities between the two audit cycles. Cochran-Armitage trend tests were employed (see Supplementary Data for analysis tables) to evaluate trends in BCS uptake over time. A p-value <0.05 was considered statistically significant. No pharmaceutical agents or chemical interventions were involved while conducting this study.
Results
A three-year retrospective analysis of breast cancer surgeries at Jinnah Hospital Lahore identified 273 patients, all of whom were included in the final audit analysis. An additional 24 patients were identified during screening but were not included due to incomplete medical records or a history of prior breast surgery. The most frequent age group was 41-50 years, accounting for 30% (n=82) of the total cohort. Table 1 presents the distribution of clinical stage across different age groups. Notably, a majority of patients presenting with Stage III disease were between 41 and 60 years of age.
Regarding disease staging at diagnosis, Stage III was most common, observed in 70.7% (n=193) of cases. Stage II accounted for 22.7% (n=62), while early-stage disease (Stages I and II combined) constituted 27.9% (n=76). Advanced-stage presentations (Stages III and IV) made up 73.3% (n=200) of the cohort.
MRM remained the predominant surgical procedure, performed in 72.9% (n=199) of patients. BCS alone was conducted in 12.5% (n=34), while 14.7% (n=40) underwent BCS combined with SLNB. Among patients undergoing BCS + SLN, 70% (n=28) received axillary clearance, whereas 30% (n=12) were managed without axillary dissection in accordance with AMAROS [6] and ACOSOG Z0011 [7] recommendations. Surgical modalities by stage are summarized in Table 2.
All Stage III cases (n=191) were managed with MRM. In contrast, early-stage cases were more frequently treated with BCS or BCS + SLN, with subsequent axillary clearance or radiotherapy as clinically indicated.
An increasing trend in surgical volume was observed over the study period: 49 surgeries in 2022, 96 in 2023, and 128 in 2024. A corresponding increase in the rate of breast-conserving procedures was also noted, with BCS alone (excluding BCS+SLN cases) accounting for 6% (n=3) in 2022 and rising to 20.3% (n=26) in 2024. These trends are detailed in Table 3.
Table 3: Annual Surgical Trends in Breast Cancer ManagementNote the statistically significant increasing trend in BCS uptake from 2022 to 2024, Cochran-Armitage Trend test (Linear-by-linear association): Z ≈ 3.97, p < 0.001BCS: Breast-conserving surgery; SLN: sentinel lymph node; MRM: modified radical mastectomy
A gradual increase in guideline-aligned breast-conserving procedures was noted across the audit period, indicating progressive institutional adherence to AMAROS and ACOSOG Z0011 recommendations rather than a change driven solely by surgical volume.
Discussion
The comparison between the 2017 and 2021 [9] and 2022 and 2024 audit cycles reveals notable improvements in breast cancer detection and treatment strategies at our institution. As shown in Figure 1, there has been a shift toward earlier-stage diagnosis. The proportion of patients presenting with Stage I disease increased from 3.6% (n=17) to 5.1% (n=14), and Stage II cases rose from 10.6% (n=50) to 22.7% (n=61). A significant difference was observed in cancer staging between the two audit cycles (χ²=31.2, p<0.001), with a shift toward earlier-stage diagnoses in the 2022-2024 cycle. These trends suggest the positive impact of improved screening practices, greater public awareness, and increased access to diagnostic services. However, systemic barriers persist. Studies have shown that challenges such as limited geographic access, diagnostic delays, and long waiting times continue to hinder timely breast cancer care, particularly in LMICs in Asia [10]. Addressing these issues requires targeted investment in healthcare infrastructure, better training of healthcare providers, and expanded diagnostic capacity.
Comparison of Breast Cancer Stages Between AuditsThe bar graph shows the percentage distribution of breast cancer stages in the 2017–2021 (yellow) and 2022– 2024 (orange) audits. The statistically significant difference in stage distribution between audit cycles indicates a shift toward earlier-stage diagnosis. Chi-square test result: χ²(3) ≈ 31.2, p < 0.001
There was a corresponding decline in Stage III cases from 84.5% (n=398) to 70.7% (n=191), which is encouraging. However, a slight rise in Stage IV presentations from 1.3% (n=6) to 2.6% (n=7) highlights the continued need to reach populations that may still be missing early detection opportunities.
Surgical trends also demonstrate a gradual move toward less invasive approaches. As shown in Figure 2, BCS in Stage I cases increased from 3% (n=14) in the 2017 to 2021 audit to 4% (n=10) in the 2022 to 2024 cycle. Additionally, BCS combined with SLN biopsy accounted for 2% (n=4). In Stage II, BCS rose from 5% (n=21) to 8% (n=24), while BCS plus SLN increased from 9% (n=29) to 12% (n=36). These changes are consistent with the findings of the AMAROS [6] and ACOSOG Z0011 [7] trials, which support conservative management in select patients. The AMAROS trial demonstrated that axillary radiotherapy can be an effective alternative to ALND in terms of survival and regional control. The ACOSOG Z0011 trial showed that ALND may be safely omitted in patients undergoing BCS who have up to two positive sentinel lymph nodes.
Comparison of Breast Cancer Treatment Percentages (2017– 2021 vs 2022–2024)Significant increase in breast-conserving procedures and corresponding decline in MRM over the years. Chi-square test result: χ²(2) ≈ 52.9, p < 0.001BCS: Breast-conserving surgery; SLN: sentinel lymph node; MRM: modified radical mastectomy
Clinical guidelines from St. Gallen, NCCN, and ASCO also recommend omitting ALND in patients who meet the ACOSOG Z0011 eligibility criteria [7]. This may extend to selected mastectomy patients with one or two positive sentinel nodes who require chest wall radiotherapy, in which case axillary radiotherapy may be offered in place of ALND [11]. Some studies suggest that applying Z0011-based criteria could reduce ALND rates by up to 20 percent [12]. Although MRM remains the most common treatment for Stage III disease, its use has declined from 85% (n=398) to 70% (n=191), indicating a broader acceptance of more conservative practices where appropriate. For Stage IV cases, a modest increase in MRM from 1.3% (n=6) to 2.6% (n=7) may reflect more aggressive treatment approaches in advanced disease. Overall, surgical management patterns showed a significant increase in breast-conserving procedures (BCS and BCS+SLN) and a reduction in MRM (χ²=52.9, p<0.001).
A year-by-year comparison, shown in Figure 3, demonstrates evolving trends in surgical practice. From 2017 to 2023, BCS rates remained low, ranging between 3% and 5% (n=8), while the use of BCS with SLN gradually increased, reaching 15.6% (n=15) in 2023. A notable shift occurred in 2024, when BCS alone increased to 20.3% (n=26). A year-wise trend analysis using the Cochran-Armitage Trend test (linear-by-linear association) from 2022 to 2024 demonstrated a statistically significant rise in BCS uptake (Z=3.97, p<0.001), reflecting progressive adaptation of conservative treatment approaches. This may reflect greater alignment with evidence-based protocols and institutional adoption of recommendations from trials such as AMAROS and ACOSOG Z0011. Despite this trend, MRM continues to dominate surgical treatment across all years. One contributing factor may be patient preference. Studies have shown that fear of recurrence is a common reason why women opt for mastectomy rather than breast conservation [13].
Comparison of Treatment Distribution (2017–2024)The line graph depicts trends in breast cancer treatment over time, showing the percentage of patients undergoing breast-conserving surgery (BCS), BCS with sentinel lymph node biopsy (BCS+SLN), and modified radical mastectomy (MRM). While MRM remains the predominant treatment, a gradual increase in BCS and BCS+SLN is observed, indicating a shift towards less invasive surgical approaches.
Several institutional and contextual factors appear to have influenced the observed surgical shifts toward breast-conserving approaches in the current audit cycle. The increased adoption of guidelines from landmark trials such as AMAROS and ACOSOG Z0011 likely played a pivotal role in shaping clinical decisions, as reflected by the 30% omission rate of ALND among SLN-positive patients. Institutional learning from the previous audit may have enhanced awareness and confidence among surgeons regarding conservative management, while rising surgical volumes from 49 in 2022 to 128 in 2024 suggest improvements in surgical infrastructure and capacity. However, persistent resource limitations, including the need for radiotherapy facilities and longer operative times associated with BCS, continue to restrict its wider implementation, especially in Stage III disease. Cultural factors such as fear of recurrence may also lead patients to opt for MRM despite eligibility for BCS. Collectively, these factors indicate a gradual but meaningful transition influenced by evidence-based training, infrastructural adaptation, and evolving patient and provider preferences within the constraints of a low-resource healthcare setting.
These findings underscore the influence of institutional protocols, national awareness programs, and multidisciplinary approaches on surgical decision-making. Earlier diagnosis and conservative surgical options are associated with improved patient outcomes and reduced morbidity. Furthermore, in low-resource settings, the financial benefits of adopting AMAROS and Z0011 guidelines are significant, as they may reduce the need for more extensive procedures, lower complication rates, and decrease hospitalization costs [14]. For broader implementation, additional policy measures should support guideline dissemination and training.
However, this study has limitations. It lacks data on post-surgical complications, recurrence rates, and follow-up pathology. These limitations highlight the need for future prospective studies that evaluate long-term outcomes, complication rates, and compliance with follow-up protocols. Future research should also examine patient understanding of treatment options and address remaining disparities in early detection and access to care.
Lastly, upcoming reviews should integrate findings from recent trials involving patients with three or more positive lymph nodes [15], as these were not included in the original ACOSOG Z0011 trial population [7].
Conclusions
This audit highlights a positive transition in breast cancer management within a resource-limited setting, marked by earlier detection and increased adoption of breast-conserving procedures. The reduction in late-stage presentations and the rising use of SLN biopsy in selected patients indicate improved diagnostic capabilities and adherence to evidence-based surgical guidelines. While MRM remains the predominant approach, particularly for advanced disease, its declining frequency reflects a gradual shift toward less invasive strategies. However, persistent challenges such as limited healthcare access, delayed diagnosis, and patient apprehensions continue to affect treatment outcomes. Strengthening health systems, promoting timely diagnosis, and enhancing awareness of guideline-based options are essential steps toward equitable and improved breast cancer care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Current and future burden of breast cancer: global statistics for 2020 and 2040 Breast Arnold M Morgan E Rumgay H 15236620223608438410.1016/j.breast.2022.08.010PMC 9465273 · doi ↗ · pubmed ↗
- 2The global burden of breast cancer in women from 1990 to 2030: assessment and projection based on the global burden of disease study 2019 Front Oncol Zhang S Jin Z Bao L Shu P 13643971420243896606710.3389/fonc.2024.1364397 PMC 11222408 · doi ↗ · pubmed ↗
- 3Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A Bray F 2092497120213353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 4Breast cancer management in low resource countries (LR Cs): consensus statement from the Breast Health Global Initiative Breast El Saghir NS Adebamowo CA Anderson BO 01120 Suppl 2201110.1016/j.breast.2011.02.00621392996 · doi ↗ · pubmed ↗
- 5Society of Surgical Oncology-American Society for Radiation Oncology-American Society of Clinical Oncology Consensus Guideline on Margins for Breast-Conserving Surgery With Whole-Breast Irradiation in Ductal Carcinoma In Situ J Clin Oncol Morrow M Van Zee KJ Solin LJ 404040463420162752871910.1200/JCO.2016.68.3573 PMC 5477830 · doi ↗ · pubmed ↗
- 6Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer: 10-year results of the randomized controlled EORTC 10981-22023 AMAROS trial J Clin Oncol Bartels SA Donker M Poncet C 215921654120233638392610.1200/JCO.22.01565 · doi ↗ · pubmed ↗
- 7Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z 0011 (Alliance) randomized clinical trial JAMA Giuliano AE Ballman KV Mc Call L 91892631820172889837910.1001/jama.2017.11470 PMC 5672806 · doi ↗ · pubmed ↗
- 8The effect of omitting axillary dissection and the impact of radiotherapy on patients with breast cancer sentinel node macrometastases: a cohort study following the ACOSOG Z 0011 and AMAROS trials Breast Cancer Res Treat Ortega Expósito C Falo C Pernas S 11112018920213408911910.1007/s 10549-021-06274-9 · doi ↗ · pubmed ↗