Integrating Safety Culture and Quality Improvement in Paediatric Emergency Departments: Evidence From a Systematic Review
Wiaam Noureldin Birima Noureldin, Hammam Noureldin, Enas Noureldin

TL;DR
This paper reviews how combining safety culture and quality improvement in pediatric emergency departments improves patient safety and care quality.
Contribution
It provides new insights into integrating safety culture with quality improvement strategies in PEDs through a systematic review.
Findings
Integration of safety culture and QI reduced unnecessary interventions and procedure times.
Key facilitators included PDSA cycles, stakeholder engagement, and clinical champions.
Barriers included workflow resistance and challenges in maintaining adherence.
Abstract
Patient safety and quality improvement (QI) are critical pillars in paediatric emergency departments (PEDs), where high-stakes care increases vulnerability to errors. While fostering a strong safety culture is recognised as essential, its practical integration with QI initiatives is not fully understood. This systematic review aimed to synthesise evidence on how safety culture principles and QI strategies are integrated within PEDs and to assess their impact on patient safety and care quality. This review was conducted following the PRISMA 2020 guidelines. A comprehensive search of PubMed, Scopus, Web of Science, Embase, and CINAHL was performed for studies published between 2020 and 2024. Eligible studies described initiatives integrating safety culture and QI in PEDs. Data on study characteristics, interventions, outcomes, and implementation factors were extracted. The methodological…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
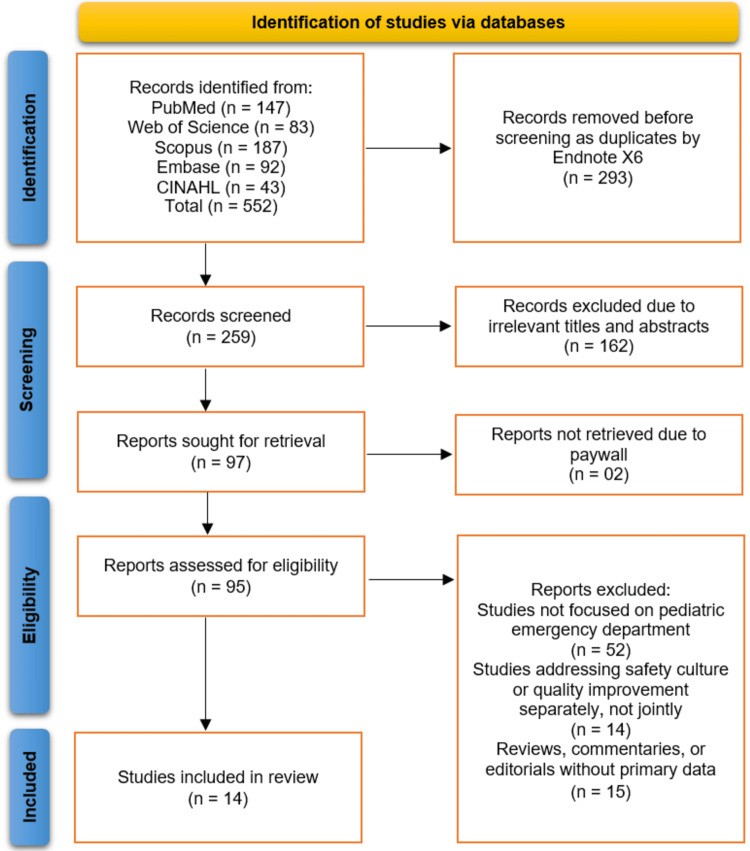 Figure 1
Figure 1| PICOS Element | Description |
| Population (P) | Pediatric patients (aged 0–18 years) receiving care in hospital-based or standalone pediatric emergency departments. |
| Intervention (I) | Interventions or initiatives integrating safety culture and QI strategies aimed at improving patient safety, communication, teamwork, or clinical outcomes. |
| Comparison (C) | Studies comparing pre- and post-intervention outcomes, or between departments/units with varying levels of safety culture or QI implementation. |
| Outcomes (O) | Outcomes related to safety culture improvements, error reduction, staff perceptions, patient outcomes, or QI process effectiveness. |
| Study Design (S) | Quantitative, qualitative, and mixed-methods studies published in peer-reviewed journals between January 2020 and October 2025 to ensure inclusion of the most recent and relevant evidence. Reviews, editorials, and conference abstracts were excluded. |
| Author (Year) | Country / Setting | Study Design | Sample Size / Population | Intervention or Focus | Safety Culture Dimension | Quality Improvement Strategy | Outcome Measures | Main Findings |
| Akcan Yildiz et al., [ | Turkey | QI initiative | Children with croup; pediatric residents | Education on croup care with reminders | Evidence-based, safe care practices | Staff training, reminders, audit-feedback | ↓ NE use, ↓ X-rays, ↑ dexamethasone, ↓ antibiotics/labs, ↓ LOS, same revisit rate | NE: 80.2%→36.3%; X-rays: 37.4%→17.1%; ↑ dexamethasone; ↓ antibiotics/tests; shorter LOS; revisits unchanged |
| Park et al., [ | USA / Single academic, quaternary-care pediatric ED | Quality Improvement Initiative | 818 ED encounters (292 pre, 526 post) | Standardizing bladder filling process for TPUS | Process efficiency, patient safety | Plan-Do-Study-Act cycles; new electronic order set; bladder scan by nurses; IV fluid optimization | Time to TPUS, ED length of stay, repeat TPUS rate | Time to TPUS decreased (138→120 min), ED LOS decreased (372→335 min), repeat TPUS decreased (18%→4%) |
| Paluck et al., [ | Canada | QI / Interventional | Children 6–24 mo | Urine bag UTI screening | Staff engagement, leadership support | PDSA cycles, interprofessional team | Catheterization rate, urine cultures, ED LOS, RVs | Catheterizations ↓ 73.3%→37.7%; urine cultures ↓ 79.8%→40.7%; LOS ↑ 17 min; RVs unchanged |
| Nucci et al., [ | Italy | Quasi-experimental, uncontrolled before-after | 885 children with forearm fractures | BST-PSA course to enable PSA in PED | Staff competence and procedural safety | Training-based QI intervention | PSA usage rate, hospitalization rate, adverse events, cost savings | PSA use increased from 37% to 85.3%; hospitalizations decreased from 68.2% to 31.8%; cost savings €370,714; no serious adverse events |
| Mullan et al., [ | USA / Children's Hospital ED & inpatient | Pre-post | ≤18 y, MBH pts, 494 alerts | MBH Clinical Debriefing | Teamwork, standards | Debrief after events | 2PR rate, ED PR duration, ED PR time, LOS, MMV, themes | ED 2PR ↓67%, ED PR duration ↓112→71 min, ED PR time ↓82%, LOS & MMV ↑, themes: teamwork 23%, standards 14%, inpatient outcomes unchanged |
| McKinley et al., [ | USA, New York City, large urban academic pediatric ED | Simulation study (based on prospective and retrospective data) | Children with cancer and central venous catheters presenting with fever | Time-specific protocol to decrease time to antibiotic delivery | System flow resilience | Discrete event simulation to test QI protocol | WT, LOS | Protocol had no significant impact on patient flow; system showed resilience, with WT increase only at high protocol uptake |
| Lipshaw et al., [ | USA / Large urban pediatric tertiary care center | Prospective QI project | Patients with constipation | Standardized evaluation & management algorithm, EMR integration, educational conferences, discharge instructions | Teamwork, learning culture, standardization | Key driver diagram, statistical process control charts, educational interventions | AXR utilization, length-of-stay, 7-day return visits, inpatient admissions | AXR utilization decreased from 49.6% to 37.1%; length-of-stay, return visits, and admissions unchanged |
| Katz-Dana et al., [ | Canada | Prospective QI study | 29 (“POCUS-first” group), 70 (non-POCUS group); children with ileocolic intussusception | Implementation of a “POCUS-first” pathway for intussusception | Streamlined workflow; timely assessment | POCUS-first pathway; physician training, education, PDSA | Physician assessment to reduction time, ED length of stay | “POCUS-first” pathway reduced assessment to reduction time and ED length of stay compared to standard care |
| Furmick et al., [ | USA (Children’s ED) | Uncontrolled before-and-after study | 215 children (118 before, 97 after) | Implementation of a point-of-care urinalysis pathway | NR | Pathway-driven point-of-care urine testing to guide treatment and disposition | Time from urinalysis order to discharge order, ED length of stay, rate of delayed treatment | Point-of-care urine testing reduced median time from urinalysis order to discharge by 30 minutes and ED length of stay by 36 minutes; no delayed treatment occurred |
| Foster et al., [ | USA / Pediatric ED & Hospital Medicine | Pre-post QI study | 168 encounters (65 baseline, 103 intervention) | CPG for febrile infants | Team collaboration | Education, audit/feedback, electronic orderset | Risk stratification, length of stay | Improved risk stratification; inappropriate admissions ↓14.8%→10.8%; high-risk LOS ↓49.4→38.2 hrs |
| De Leon et al., [ | USA / Pediatric Level I Trauma Center | Historical control, posttest | 180 patients (90/90) | Alternate care site for surge | Patient flow, timely care | Activate alternate care site | Census, LOS (admit/discharge), LWBS, hours per visit, patient satisfaction | Reduced wait times, LOS, LWBS; hours per visit and satisfaction unchanged |
| Carney et al., [ | USA | QI / Lean Implementation | 70,088 | Redesign of ED front-end processes: Flow Nurse/EMT roles, quick registration, direct-bedding, physician-led Intake | Teamwork, Communication, Process Awareness | Lean methodology, Quality Improvement | Door-to-provider time, LWBS rate, % patients seen <30 min, ED length-of-stay, patient satisfaction, 72-hour return rate | Median door-to-provider time ↓ 49% (25 min), LWBS ↓ 56%, % seen <30 min ↑, overall ED LOS ↓, patient satisfaction ↑, no worsening in 72-hour returns |
| Bram et al., [ | USA / Pediatric Emergency Department of a tertiary care children’s hospital | QI initiative | 1052 and 2204 | Implementation of sterile blood culture collection process with nursing education and individualized feedback | Teamwork, accountability, adherence to safe clinical practices | Process standardization, staff education, performance feedback | Primary: % of contaminated blood cultures; Process: nurse adherence to sterile steps; Balancing: antibiotic administration time and ED stay | Contamination reduced from 6.7% to 2.1%; 98% nurses adhered to ≥75% of sterile steps; no delay in antibiotic administration or ED stay |
| Baumer-Mouradian et al., [ | USA (Pediatric Emergency Department) | QI study using PDSA cycles | 33,311 pediatric patients | Implementation of influenza vaccination program including vaccine screening, protocol creation, staff education, pharmacy workflow revision, and weekly feedback | Teamwork, communication, staff engagement, patient safety | PDSA cycles, process mapping, staff education, protocol standardization, feedback loops | % patients screened, # vaccines administered, ED LOS, vaccine waste, financial impact | Screening improved from 0% to 90%; 1,323 vaccines administered; no increase in LOS or financial loss; program was efficient and cost-effective |
| Author (Year) | Integration Approach | Measurement Tools Used | Barriers Identified | Facilitators / Enablers |
| Akcan Yildiz et al., [ | Education + reminders for residents to reduce over-testing | NE use, X-rays, dexamethasone, antibiotics, labs, LOS | High rates of unnecessary interventions remain | Education, reminders, protocols, monitoring |
| Park et al., [ | Standardizing bladder filling process using sequential PDSA cycles | Statistical process control charts; monthly mean time to TPUS; ED length of stay; percentage of repeat TPUS | Time-consuming bladder filling leading to delays, poor visualization, prolonged ED LOS | New electronic order set; bladder scan by ED nurses; sequential PDSA cycles; iterative process improvements |
| Paluck et al., [ | Urine bag screening with POC urinalysis using PDSA cycles | Catheterization rate, urine culture rate, ED LOS, return visits | Slight LOS increase, workflow change | Nursing champion, stakeholder engagement, strategic alignment, provider buy-in |
| Nucci et al., [ | Implementation of a BST-PSA course to enable PSA use in Pediatric Emergency Department | Historical control and prospective analysis; Statistical tests: Fisher exact test, Pearson χ² test | NR | Training program; Improved patient flow; Increased PSA use; Reduced hospitalizations; Cost savings; Safety maintained with no serious adverse events |
| Mullan et al., [ | MBH clinical debriefing after behavioral events | 2PR rate, ED PR duration, LOS, MMV, qualitative themes | Limited inpatient impact and partial adoption | Team cooperation and adherence to clinical standards |
| McKinley et al., [ | Time-specific antibiotic protocol | Simulation model, ED data | Increased WT for some patients | System resilience, safe testing |
| Lipshaw et al., [ | Standardized algorithm, EMR integration, educational sessions | Statistical process control chart | NR | Multidisciplinary team, QI methods, standardized interventions |
| Katz-Dana et al., [ | Implementation of a “POCUS-first” pathway in Pediatric ED for suspected intussusception | Time from physician initial assessment to radiology-performed US; time from physician initial assessment to reduction; ED LOS | Implicit barriers include reliance on radiology-performed ultrasound, potential training gaps, workflow delays | Pediatric emergency medicine physician training, education, pathway dissemination, continuous improvement via PDSA cycles |
| Furmick et al., [ | Implementation of a point-of-care urine testing pathway to guide UTI management in pediatric ED | Point-of-care urinalysis; comparison with urine microscopy; outcome measures included time from urinalysis order to discharge order, overall ED length of stay, and rate of delayed treatment | No major barriers explicitly reported; potential implicit barrier could be change in workflow from standard urine microscopy | Reduced length of stay and faster treatment decisions; pathway-driven decision-making; prospective evaluation supporting adoption |
| Foster et al., [ | CPG implementation via Model for Improvement; collaboration between pediatric emergency and hospital medicine; interventions: education, audit/feedback, electronic orderset | Statistical process control charts | NR | Collaboration across specialties; structured interventions; quality improvement methodology |
| De Leon et al., [ | Alternate care site to manage patient surges | Census, LOS (admissions/discharges), left without being seen, patient satisfaction, process metrics | Limited generalizability, seasonal activation | Quick setup, low cost, proximity to ED, maintained patient flow and satisfaction |
| Carney et al., [ | Lean QI redesign of ED front-end, new roles, quick registration, direct-bedding, physician-led Intake | Door-to-provider time, LWBS rate, ED LOS, patient satisfaction, 72-hr return | NR | Inter-professional team, Lean methodology, novel Intake system |
| Bram et al., [ | Sterile blood culture collection integrated with nursing education and feedback to improve safety and quality in the pediatric ED. | Audit cards, contamination rate monitoring, antibiotic timing, and ED stay duration. | Inconsistent adherence to sterile steps; reliance on self-reporting. | Ongoing training, feedback, standardized process, and staff engagement. |
| Baumer-Mouradian et al., [ | Influenza vaccination integrated into pediatric ED workflow using PDSA cycles. | Process mapping, vaccination screening rate, vaccines administered, ED LOS, and cost impact. | Workflow gaps, limited staff training, and possible ED flow disruption. | Team collaboration, clear protocol, staff education, revised pharmacy steps, and regular feedback. |
| QI-MQCS Domain | Akcan Yildiz et al., [ | Park et al., [ | Paluck et al., [ | Nucci et al., [ | Mullan et al., [ | McKinley et al., [ | Lipshaw et al., [ | Katz-Dana et al., [ | Furmick et al., [ | Foster et al., [ | De Leon et al., [ | Carney et al., [ | Bram et al., [ | Baumer-Mouradian et al., [ |
| 1. Organizational Motivation | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 2. Intervention Rationale | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 3. Intervention Description | Yes | Yes | Yes | Yes | Yes | Partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4. Organisational Characteristics | Partial | Yes | Partial | Partial | Yes | Partial | Yes | Partial | Yes | Yes | Yes | Yes | Yes | Yes |
| 5. Implementation Strategy | Yes | Yes | Yes | Yes | Yes | Partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 6. Study Design | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 7. Comparator Description | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 8. Data Source | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 9. Timing | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 10. Adherence/Fidelity | Partial | Yes | Yes | No | Partial | N/A | Partial | Partial | Yes | Partial | Partial | Partial | Yes | Yes |
| 11. Health Outcomes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 12. Organizational Readiness | No | Partial | Yes | No | Partial | No | Partial | No | Partial | Partial | Partial | Partial | Partial | Yes |
| 13. Penetration/Reach | Yes | Yes | Yes | Yes | Yes | Partial | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 14. Sustainability | No | Partial | No | Partial | No | No | Partial | No | No | No | Partial | Partial | Partial | Partial |
| 15. Spread | No | No | No | No | No | No | No | No | No | No | No | No | No | No |
| 16. Limitations | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPatient Safety and Medication Errors · Clinical Reasoning and Diagnostic Skills · Simulation-Based Education in Healthcare
Introduction and background
Patient safety and quality improvement (QI) have emerged as fundamental pillars in healthcare systems worldwide, particularly within paediatric emergency departments (PEDs), where the complexity and urgency of care can heighten the risk of medical errors [1]. Paediatric patients present unique challenges due to age-specific physiological differences, communication barriers, and reliance on caregivers, making the emergency setting inherently vulnerable to adverse events [2]. Therefore, fostering a strong safety culture, defined as the shared values, attitudes, and behaviours that prioritise safety, has become an essential strategy to enhance patient outcomes and optimise care delivery in paediatric emergency settings [3].
Safety culture encompasses various dimensions, including teamwork, communication openness, leadership support, and error reporting, all of which are instrumental in shaping how healthcare professionals perceive and respond to risks [4]. In PEDs, where rapid [5] and interdisciplinary coordination are critical, a positive safety culture not only mitigates harm but also supports continuous learning and system resilience. However, the translation of safety culture principles into practical and sustainable quality improvement initiatives remains a significant challenge for many institutions.
Quality improvement frameworks, such as plan-do-study-act (PDSA) cycles, lean methodologies, and Six Sigma, have been increasingly adopted in paediatric emergency care to streamline workflows, reduce variability, and improve safety outcomes [6]. When effectively integrated with safety culture interventions, these approaches can create a synergistic effect, empowering frontline staff, enhancing accountability, and promoting data-driven improvements [7]. Despite this potential, the degree and mechanisms through which safety culture integration influences the success of QI initiatives in PEDs remain inconsistently reported across the literature.
Recent studies have highlighted that organisational leadership, staff engagement, and measurement tools such as the Safety Attitudes Questionnaire (SAQ) or Hospital Survey on Patient Safety Culture (HSOPSC) play pivotal roles in determining the effectiveness of such integrations [8]. Yet, variations in study designs, outcomes, and contextual factors make it difficult to generalise findings or establish best practices. A comprehensive synthesis of available evidence is therefore essential to understand how safety culture and QI strategies intersect to improve patient safety in paediatric emergency care.
This systematic review aims to critically evaluate and synthesise the existing literature on the integration of safety culture and quality improvement initiatives within paediatric emergency departments. Specifically, it seeks to identify common approaches, measurement tools, barriers, and facilitators associated with implementation and to assess their impact on patient safety outcomes. Beyond summarising current evidence, this review is expected to generate actionable insights that can inform evidence-based strategies to strengthen organisational culture, enhance team communication, and reduce preventable adverse events in paediatric emergency settings. The findings will be particularly valuable for healthcare leaders, clinicians, and policymakers seeking to translate safety culture principles into measurable quality improvement practices, ultimately contributing to safer, more reliable, and child-centred emergency care.
Review
Methodology
Study Design and Protocol
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines to ensure transparency and methodological rigour [9]. The review protocol was developed a priori to outline the search strategy, inclusion criteria, data extraction process, and quality assessment approach. The primary objective was to synthesise existing evidence on the integration of safety culture and QI strategies in PEDs, focusing on their implementation, measurement tools, barriers, facilitators, and outcomes related to patient safety and care quality.
Eligibility Criteria (PICOS Framework)
The eligibility criteria for study selection were defined according to the PICOS framework (population, intervention, comparison, outcomes, and study design) (Table 1).
Information Sources and Search Strategy
A comprehensive literature search was conducted across four major databases: PubMed, Scopus, Web of Science, and Embase. These databases were selected for their broad coverage of biomedical and healthcare research. The search strategy combined Medical Subject Headings (MeSH) and free-text terms using Boolean operators (AND, OR) to capture studies related to “safety culture”, “quality improvement”, and “paediatric emergency department.” Search strings were tailored for each database to optimise sensitivity and specificity. The search was limited to studies published in English between 2020 and 2025 to capture contemporary developments and implementation trends in safety and quality improvement practices. Reference lists of all included studies were manually screened to identify additional relevant publications. The detailed search strategy for each database is provided in the Appendix, Table 5.
Study Selection
All retrieved references were imported into EndNote X9 (Clarivate Analytics) for efficient management and removal of duplicates. Following de-duplication, two independent reviewers screened the titles and abstracts based on the predefined eligibility criteria. Full-text articles were subsequently assessed for final inclusion. Disagreements between reviewers were resolved through discussion or by consultation with a third reviewer to ensure unbiased selection.
Data Extraction
A standardised data extraction form was developed to ensure consistency in data collection. Extracted information included author details, year of publication, country/setting, study design, sample characteristics, intervention type, safety culture dimension, quality improvement strategy, outcome measures, and key findings. Additional information regarding barriers, facilitators, and implementation frameworks was also captured where available. The extracted data were cross-verified by a second reviewer to ensure accuracy and completeness.
Risk of Bias and Quality Assessment
The methodological quality and risk of bias of included studies were assessed using the quality improvement minimum quality criteria set (QI-MQCS) tool [10]. This validated instrument evaluates QI-focused studies across 16 domains, including intervention description, study design, data source, outcomes, and sustainability. Each study was independently appraised by two reviewers, with disagreements resolved through consensus. Studies were categorised as high, moderate, or low quality based on their cumulative QI-MQCS scores.
Data Synthesis
Given the expected methodological heterogeneity among studies, in terms of study design, intervention type, outcome measures, and assessment tools, a meta-analysis was not performed. Instead, a narrative synthesis approach was used to qualitatively integrate findings across studies. This approach allowed for the exploration of patterns, themes, and contextual factors influencing the integration of safety culture and QI interventions in paediatric emergency settings. The decision to forego meta-analysis was justified by the diverse nature of the included studies, which precluded statistical pooling without compromising validity or interpretability.
Ethical Considerations
As this study synthesised data from previously published research, ethical approval was not required. However, all included studies were assumed to have obtained ethical clearance from their respective institutional review boards.
Results
Study Selection Process
The study selection process is detailed in the PRISMA flowchart (Figure 1). A total of 552 records were identified through initial searches of electronic databases (PubMed: n=147, Web of Science: n=83, Scopus: n=187, Embase: n=92, CINAHL: n=43). After the removal of 293 duplicate records, 259 unique records were screened based on their titles and abstracts. This screening led to the exclusion of 162 records that were deemed irrelevant to the review's focus. The full text of the remaining 97 reports was sought for retrieval, of which 95 were successfully accessed; two reports could not be retrieved due to paywall restrictions. A detailed eligibility assessment of these 95 full-text articles was performed, resulting in the exclusion of 81 studies. The reasons for exclusion were as follows: 52 studies were not focused on the paediatric emergency department setting, 14 studies addressed either safety culture or quality improvement in isolation but not their integration, and 15 reviewed articles, commentaries, or editorials that did not present primary data. Ultimately, 14 studies met all inclusion criteria and were incorporated into the systematic review [11-24] (Figure 1).
Studies selection process illustrated on PRISMA flowchartThis diagram illustrates the systematic process of study identification, screening, eligibility assessment, and inclusion for the systematic review, detailing the number of records sourced from each database and the reasons for exclusion at each stage.
Characteristics of Included Studies
The systematic review included 14 studies [11-24] that investigated the integration of safety culture principles with QI methodologies in PEDs. The characteristics of these studies are detailed in Table 2. The included studies were published between 2020 and 2024 and were conducted in a range of countries, including the United States, Canada, Turkey, and Italy. All studies employed QI frameworks, with the PDSA cycle being the most frequently utilised methodology [12,13,18,19,24]. Other approaches included lean methodology [22], the model for improvement [20], and simulation modelling [16]. The interventions targeted a diverse array of clinical processes and safety concerns, such as the management of specific conditions (e.g., croup [11], intussusception [18], febrile infants [20]), procedural efficiency (e.g., time to ultrasound [12], procedural sedation [14]), and system-level challenges (e.g., patient flow [22], physical restraint use [15], vaccination rates [24]). Sample sizes varied considerably, ranging from focused studies with under 100 encounters [18,20] to large-scale initiatives encompassing over 70,000 patient visits [22,24].
Key Quality Improvement Interventions and Integration Approaches
The interventions implemented across the studies can be broadly categorised into several key integration approaches. A prominent strategy was the standardisation of clinical processes through the implementation of clinical pathways, algorithms, and order sets. For instance, studies successfully introduced standardised pathways for constipation management [17], urinary tract infection (UTI) diagnosis using point-of-care testing [19], and evaluation of ovarian torsion [12], all of which aimed to reduce unwarranted practice variation and promote evidence-based care.
Another common approach was education and training initiatives designed to enhance staff competence and adherence to best practices. These included structured education for residents on croup management [11], simulation-based training for procedural sedation and analgesia [14], and targeted training for nurses on sterile blood culture collection techniques [23]. Furthermore, several studies leveraged technological integration to support these efforts, such as the incorporation of "POCUS-first" pathways for intussusception into clinical workflow [18] and the development of electronic order sets to standardise bladder filling for pelvic ultrasounds [12].
System-level process redesign was also a significant theme. Studies like those by Carney et al. [22] and De Leon et al. [21] focused on reorganising the front-end operations of the PED and establishing alternate care sites, respectively, to improve patient flow and manage surges. Finally, structured team communication and feedback mechanisms were employed to foster a culture of safety and continuous learning. This was exemplified by the implementation of clinical debriefing processes following behavioural health emergencies to reduce physical restraint use [15] and the use of audit-and-feedback to reinforce sterile procedures and improve vaccination screening rates [23,24]. A summary of the integration approaches, along with the tools and contextual factors involved, is provided in Table 3.
Impact on Safety Culture Dimensions and Patient Outcomes
The integrated QI initiatives demonstrated a positive impact on various dimensions of safety culture and led to measurable improvements in patient care outcomes.
Teamwork and communication were explicitly enhanced in several studies. Mullan et al. [15] reported that post-event debriefing improved interdisciplinary cooperation, while Bram et al. [23] and Baumer-Mouradian et al. [24] highlighted that their successes were facilitated by strong team collaboration and engagement.
Evidence-based and standardised practices were significantly promoted, leading to a reduction in unnecessary and potentially harmful interventions. For example, Akcan Yildiz et al. [11] achieved a substantial decrease in the use of nebulised epinephrine and X-rays for croup, while Lipshaw et al. [17] reduced abdominal X-ray utilisation for constipation. Paluck et al. [13] successfully decreased invasive catheterisation for UTI screening, and Foster et al. [20] reduced inappropriate hospitalisations for febrile infants.
Patient safety and procedural efficiency were consistently improved. Multiple studies reported reductions in time to key interventions or diagnoses, such as time to pelvic ultrasound [12], time to antibiotic delivery [16], and time from assessment to reduction for intussusception [18]. This is often translated into a decreased ED LOS [12,19,22]. Importantly, initiatives also directly enhanced procedural safety, with Nucci et al. [14] increasing the use of procedural sedation without serious adverse events, and Bram et al. [23] dramatically reducing blood culture contamination rates.
Patient flow and system efficiency were key outcomes for several system-level interventions. Carney et al. [22] reported a 49% reduction in door-to-provider time and a 56% decrease in patients leaving without being seen following a front-end redesign. The use of an alternate care site during surges also effectively reduced wait times and maintained patient satisfaction [21].
Facilitators, Barriers, and Implementation Strategies
The successful implementation of these QI initiatives was supported by several key facilitators. As detailed in Table 2, iterative improvement methods like PDSA cycles were crucial for testing changes and refining interventions [12,13,19]. Stakeholder engagement and the presence of clinical champions were repeatedly cited as critical enablers, ensuring provider buy-in and sustaining momentum [13,24]. Furthermore, structured education for staff [11,14,18,23] and the use of audit and feedback mechanisms [11,20,23] were vital for embedding new practices into the clinical culture.
Common barriers included resistance to workflow changes [13,18], the challenge of achieving consistent staff adherence to new protocols [15,23], and potential disruptions to established ED workflows [16,24]. For instance, Katz-Dana et al. [18] noted implicit barriers such as a traditional reliance on radiology-performed ultrasounds, while McKinley et al. [16] found that a new antibiotic protocol could inadvertently increase wait times for some patients under high-uptake scenarios, illustrating the complex interplay of interventions within a dynamic system.
Risk of Bias (Quality) Assessment of Included Studies
The methodological quality of the 14 included quality improvement studies [11-24] was assessed using the QI-MQCS. Overall, the studies demonstrated strong reporting in foundational domains: all studies clearly articulated their organisational motivation and intervention rationale [11-24], utilised an appropriate QI study design with a well-described comparator [11-24], and consistently reported on relevant health outcomes and limitations [11-24]. However, several key areas exhibited common reporting weaknesses. Specifically, measurement and reporting of implementation fidelity and adherence were variable, with only five studies [12,13,19,23,24] providing substantial evidence, while others reported this only partially [11,15,17,18,20-22] or not at all [14]. Furthermore, assessments of organisational readiness prior to implementation were often absent [11,14,16,18] or only partially described [12,13,15,17,19-23], and while most studies documented the penetration of their intervention [11-15,17-24], evidence of sustainability beyond the study period was limited, with no study providing strong evidence and the majority reporting none [11,13,15,16,18-20] or only partial evidence [12,14,17,21-24]. Crucially, no study reported on the spread of the intervention to other units or contexts [11-24] (Table 4).
Discussion
This systematic review synthesised evidence from 14 QI studies to elucidate the strategies and outcomes associated with integrating safety culture principles into QI initiatives within PEDs. The findings collectively demonstrate that a deliberate focus on core safety culture components, such as teamwork, standardised processes, staff engagement, and continuous learning, is not merely complementary but foundational to the success of QI efforts aimed at enhancing patient care. The included studies, despite their heterogeneity in clinical focus, consistently reveal that successful interventions are those that move beyond a purely technical fix and embed change within the social and cultural fabric of the ED. For instance, the most impactful initiatives, such as the clinical debriefing process implemented by Mullan et al. [15] to reduce physical restraints, explicitly targeted psychological safety and interdisciplinary communication, thereby addressing the underlying cultural norms that permit restrictive practices. Similarly, the successes of Bram et al. [23] in reducing blood culture contamination and Baumer-Mouradian et al. [24] in launching an ED vaccination programme were critically dependent on fostering accountability and collective ownership among nursing staff, underscoring that procedural adherence is a cultural artefact as much as a technical skill.
The efficacy of standardised pathways and protocols, as seen in the management of constipation [17], febrile infants [20], and suspected intussusception [18], underscores a central theme: reducing unwarranted clinical variation is a potent mechanism for enhancing both safety and efficiency. These findings align strongly with the broader literature on clinical standardisation. For example, a seminal study by Alessandrini et al. [25] on implementing a paediatric asthma clinical pathway also demonstrated significant reductions in ED length of stay and improved adherence to evidence-based therapies, mirroring the outcomes achieved by Foster et al. [20] and Lipshaw et al. [17]. Our review extends this understanding by highlighting that the integration of these pathways, through EMR order sets, staff education, and audit-and-feedback, is what activates their potential. This resonates with the work of Grol & Grimshaw [26], who long asserted that the effectiveness of guidelines is determined by the strategies used to implement them. The "POCUS-first" pathway by Katz-Dana et al. [18] is a prime example, where streamlining workflow and providing physician training were as crucial as the pathway itself, leading to significant reductions in time to diagnosis and treatment.
Furthermore, the role of iterative, data-driven QI methodologies, particularly the PDSA cycle, emerged as a critical facilitator across multiple studies [12,13,19,24]. This approach allows for rapid-cycle testing and adaptation, which is essential in the dynamic and high-stakes environment of the PED. The work of Park et al. [12] in standardising the bladder-filling process for pelvic ultrasounds exemplifies this; through sequential PDSA cycles, they were able to refine their intervention, leading to sustained reductions in time to ultrasound and ED length of stay. This aligns with the Model for Improvement, popularised by Langley et al. [27], which has been widely adopted in healthcare to facilitate incremental, sustainable change. Our findings corroborate the value of this model, as used by Foster et al. [20], and suggest that its flexibility is particularly well-suited to cultivating a safety culture, as it empowers frontline staff to identify problems and test solutions, thereby fostering a sense of ownership and a culture of continuous learning.
The impact on specific safety culture dimensions was palpable across the reviewed studies. Teamwork and communication were repeatedly cited as both a target and a facilitator of success. The reduction in physical restraints through debriefing [15] and the improvement in sterile technique through nursing education and feedback [23] are direct reflections of enhanced team coordination and psychological safety. These findings are consistent with earlier research linking safety culture to patient outcomes. A study by Huang et al. [28] in a general ED setting found that higher scores on safety culture surveys, particularly in the domains of teamwork and communication openness, were associated with lower rates of reported medication errors. Our review provides concrete, QI-driven examples that affirm this relationship in paediatrics, demonstrating that cultural elements can be actively cultivated through structured interventions. Moreover, the focus on staff engagement and leadership support in studies like Paluck et al. [13] and Baumer-Mouradian et al. [24] reinforces the findings of Singer et al. [29], who identified leadership commitment and staff involvement as critical predictors of a positive safety culture in hospitals.
However, the QI-MQCS assessment reveals a significant gap between achieving short-term, local success and demonstrating long-term, systemic transformation. The near-universal absence of reporting on sustainability and spread is a critical limitation of the current evidence base. While studies like those of Carney et al. [22] and Nucci et al. [14] showed impressive results in patient flow and cost savings, respectively, it remains unknown whether these improvements were maintained after the formal study period concluded or if they could be replicated in other settings. This is a common challenge in QI literature. A systematic review by Endalamaw et al. [30] on the sustainability of QI programmes in healthcare found that few studies report long-term outcomes, and even fewer describe the factors that promote sustainment. Our findings are congruent with this, highlighting a pervasive "projectification" of QI, where initiatives are treated as time-limited endeavours rather than permanent shifts in practice and culture. The failure to report on spread limits the generalisability and potential impact of these successful interventions. The work of Carney et al. [22] on front-end redesign, for example, represents a potentially transformative model for EDs globally, yet without documented efforts at dissemination and adoption in other contexts, its broader utility remains theoretical.
Limitations
This systematic review has several limitations. First, the included studies themselves possess methodological constraints, as identified by the QI-MQCS assessment. The prevalent use of pre-post designs without concurrent control groups limits the strength of causal inference, as secular trends or other concurrent changes in the PED could account for some of the observed effects. The general lack of long-term follow-up data on sustainability, as previously discussed, means the enduring impact of these interventions remains uncertain. Second, the search was limited to published, peer-reviewed literature, which may introduce publication bias, as successful QI initiatives are more likely to be written up and published than failed or inconclusive ones. Third, the definition and measurement of "safety culture" were not uniform across studies; while some explicitly measured dimensions like teamwork, others inferred cultural impact from process outcomes. This heterogeneity makes direct comparison and synthesis challenging. Finally, the review focused specifically on the PED context, and while the principles of integrating safety culture and QI are likely generalisable, the specific strategies and their effectiveness may differ in other clinical settings.
Conclusions
The integration of safety culture principles is a powerful catalyst for successful quality improvement in the paediatric emergency department. The synthesis of 14 studies demonstrates that interventions which standardise care, engage and educate frontline staff, leverage iterative improvement methods, and foster teamwork and communication are consistently associated with enhanced patient safety, improved clinical outcomes, and greater operational efficiency. These findings underscore that QI is not merely a technical or procedural exercise but a deeply socio-cultural one. The most meaningful and sustained improvements arise from initiatives that thoughtfully address the human elements of teamwork, psychological safety, and shared accountability. Moving forward, the field must advance beyond demonstrating initial success. Future QI initiatives and their publications must prioritise and rigorously evaluate the long-term sustainability of improvements and develop robust strategies for spreading effective interventions beyond single institutions. By doing so, the PED community can transform isolated successes into an enduring culture of safety and excellence that benefits all children seeking emergency care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The global challenges for quality improvement and patient safety Int J Qual Health Care Iqbal U Khan HA Li YJ 33202110.1093/intqhc/mzaa 04632484223 · doi ↗ · pubmed ↗
- 2Age-based challenges to type 1 diabetes management in the pediatric population Front Pediatr Lan YY Kovinthapillai R Kędzia A NiechciałE 14342761220243928645310.3389/fped.2024.1434276 PMC 11402681 · doi ↗ · pubmed ↗
- 3Barriers and facilitators of pain management in children: a scoping review BMC Anesthesiol Atefeh S 1482520254017013510.1186/s 12871-025-02941-2PMC 11963635 · doi ↗ · pubmed ↗
- 4The impact of leadership on fostering a safety-oriented organizational culture Safety-Centric Operations Research: Innovations and Integrative Approaches: A Multidisciplinary Approach to Managing Risk in Complex Systems Yazdi M 202510.1007/978-3-031-82934-5
- 5Decision-making in the pediatric emergency department-a survey of guidance strategies among residents Children (Basel) Gaus S Schmidt J Lüse P 9202210.3390/children 9081197 PMC 940632036010085 · doi ↗ · pubmed ↗
- 6Common quality improvement methodologies including the model for improvement, lean, and six sigma Clin Perinatol Coughlin K Posencheg MA 2853065020233720198210.1016/j.clp.2023.02.002 · doi ↗ · pubmed ↗
- 7The use of lean six sigma for improving availability of and access to emergency department data to facilitate patient flow Int J Environ Res Public Health Daly A Teeling SP Ward M 18202110.3390/ijerph 182111030 PMC 858267134769548 · doi ↗ · pubmed ↗
- 8Measuring patient safety culture Patient Safety Coaching: Transforming Healthcare Culture Knowles S 193217 Switzerland Springer, Cham 2024