Corpus Callosum Diffusion Restriction in Neonatal Congenital Myotonic Dystrophy
Nanoha Sakatani, Hiroyuki Ikeda, Yuki Inami, Yasushi Noguchi, Katsunori Fujii

TL;DR
A neonate with congenital myotonic dystrophy showed corpus callosum diffusion restriction, possibly due to respiratory failure-related brain injury.
Contribution
This case is the first to report corpus callosum diffusion restriction in neonatal congenital myotonic dystrophy.
Findings
MRI showed restricted diffusion in the genu and splenium of the corpus callosum in a CDM neonate.
Follow-up imaging showed resolution of diffusion restriction but mild atrophy of the genu.
Genetic testing confirmed CDM with 1000-1150 CTG repeats.
Abstract
Congenital myotonic dystrophy (CDM) is the most severe form of myotonic dystrophy type 1 (DM1), typically presenting in the neonatal period with hypotonia, respiratory distress, and feeding difficulties. Neuroimaging findings in neonates with CDM are rarely described. We present a genetically confirmed case of CDM in a neonate who demonstrated restricted diffusion in the genu and splenium of the corpus callosum (CC). The patient developed respiratory failure at three weeks of age and required mechanical ventilation. The brain MRI performed 11 days after onset revealed restricted diffusion in the genu and splenium of the CC. The follow-up imaging at four months showed resolution of diffusion restriction and mild atrophy of the genu. Genetic testing confirmed CDM with 1000-1150 trinucleotide (CTG) repeats. We considered that the diffusion restriction observed in this patient may have been…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
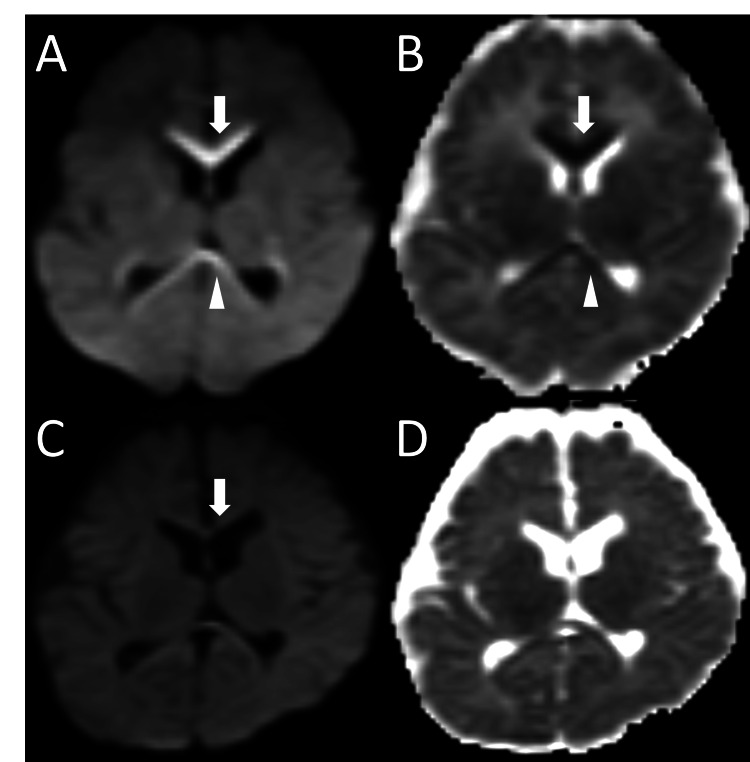 Figure 1
Figure 1| Test | Result | Reference value (for age & gender) | Unit |
| Venous blood gas | |||
| pH | 7.235 | 7.31–7.41 | |
| pCO2 | 51.5 | 40–50 | mmHg |
| HCO3- | 21 | 23–28 | mmol/L |
| Base excess | -7 | -2–2 | mmol/L |
| Glucose | 117 | 70–105 | mg/dL |
| Lactate | 7.5 | 0.5–2.2 | mmol/L |
| Hematology | |||
| White blood cells | 16100 | 4800–18500 | /μL |
| Hemoglobin | 20 | 11–15 | g/dL |
| Platelet | 465 | 150–450 | x 103/μL |
| Biochemistry | |||
| Total bilirubin | 0.7 | 0.4–3.2 | mg/dL |
| Aspartate aminotransferase | 26 | 20–62 | U/L |
| Alanine aminotransferase | 18 | 11–45 | U/L |
| Lactate dehydrogenase | 293 | 198–404 | U/L |
| Alkaline phosphatase | 557 | 530–1610 | U/L |
| Urea nitrogen | 14 | 3.7–15.5 | mg/dL |
| Creatinine | 0.21 | 0.3–0.8 | mg/dL |
| Na+ | 130 | 135–143 | mmol/L |
| K+ | 5.8 | 4.1–6.0 | mmol/L |
| Cl- | 97 | 101–111 | mmol/L |
| Creatine kinase | 74 | 44–310 | U/L |
| C-reactive protein | 0.17 | 0–0.3 | mg/dL |
| Cerebrospinal fluid | |||
| Cells | 4 | 0–20 | /μL |
| Mononuclear cells | 91 | 60–80 | % |
| Polymorphonuclear cell | 9 | 20–40 | % |
| Protein | 45 | 30–100 | mg/dL |
| Glucose | 59 | 40–80 | mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic Neurodegenerative Diseases · Infectious Encephalopathies and Encephalitis · Mitochondrial Function and Pathology
Introduction
Congenital myotonic dystrophy (CDM) is the most severe form of myotonic dystrophy type 1 (DM1), typically presenting in the neonatal period with hypotonia, respiratory distress, and feeding difficulties [1-3]. While the clinical features of CDM are well described, neonatal neuroimaging findings remain underreported [4-6]. Here, we report a neonate with genetically confirmed CDM who exhibited restricted diffusion in the genu and splenium of the corpus callosum (CC), suggestive of pre-Wallerian degeneration (pWD) due to hypoxic ischemic encephalopathy.
Case presentation
A female infant was born at 38 weeks and four days of gestation via spontaneous vaginal delivery, weighing 2710 g. There was no polyhydramnios or concern regarding fetal movements during pregnancy. She cried promptly after birth without signs of neonatal asphyxia. The Apgar score was not available. She was discharged on day five without any apparent abnormalities. However, since she developed pallor, irregular breathing, and poor feeding, she was admitted to our hospital on day 23. On admission, she was lethargic, cyanotic, hypothermic, and tachycardic, with episodes of apnea. Her muscle tone was normal, but her cry had been weak for the three days preceding admission. Oxygen saturation was 85%, frequently dropping below 70%. We immediately treated her with emergency ventilation, intubation, and intensive care unit admission. Her weight was 3100 g, reflecting an average daily weight gain of approximately 25 g. Although initial laboratory tests and microbiological studies were unremarkable, venous blood gas analysis revealed respiratory and metabolic acidosis (Table 1). The results of all the newborn mass screening tests, including tandem mass spectrometry, were negative, providing additional clinical context. Imaging (chest X-ray, echocardiography, and head computed tomography) showed no abnormalities. However, the brain MRI on hospital day 10 (age 32 days) revealed restricted diffusion in the genu and splenium of the CC (Figures 1A, 1B) and a small lesion in the left periventricular white matter (data not shown). These areas appeared hyperintense on the diffusion-weighted imaging (DWI) and showed low values on the apparent diffusion coefficient maps, with no corresponding abnormalities on the T1- or T2-weighted images. Her respiratory status gradually improved, allowing extubation on hospital day eight, and she was discharged on day 15 without complications.
Diffusion restriction in the corpus callosum in congenital myotonic dystrophyAxial diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) maps are shown at the level of the corpus callosum. (A, B) MRI obtained at 32 days of age (hospital day 10) demonstrates high signal intensity in the genu (arrow) and splenium (arrowhead) on DWI (A), with corresponding low signal on the ADC map (B), indicating restricted diffusion. (C, D). A follow-up MRI at four months shows resolution of the previously observed diffusion restriction and mild atrophy of the genu of the corpus callosum (arrow).
The follow-up MRI at four months showed resolution of the previously observed diffusion restriction and mild atrophy of the genu of the CC (Figures 1C, 1D). Development was reported as normal until age three years, but she showed mild intellectual disability at age six years. At age 10 years, the patient was diagnosed with CDM after her mother was diagnosed with DM1 due to muscle weakness. Genetic testing revealed 1000-1150 CTG repeats in the patient and 200 in the mother.
Discussion
In this report, we observed diffusion restriction in the genu and splenium of the corpus callosum, associated with progressive respiratory failure in a child with CDM. These lesions disappeared after four months, leaving behind atrophy, suggesting that they were due to hypoxic-ischemic encephalopathy caused by respiratory failure in CDM.
MRI, particularly diffusion-weighted imaging (DWI), can detect early brain injury in neonates [7]. One such process is Wallerian degeneration (WD), in which axons and their myelin sheaths degenerate distal to the site of injury, typically over days to weeks following hypoxia or trauma [8]. A preceding stage, known as pre-Wallerian degeneration (pWD), involves early axonal changes, such as swelling and cytoskeletal disruption, that appear as restricted diffusion on MRI before structural abnormalities become apparent [9,10]. The pWD has been mainly reported in severe hypoxic-ischemic encephalopathy (HIE), affecting pathways such as the corticospinal tracts and the corpus callosum (CC) [9,10].
Previously reported neuroimaging findings in CDM include ventriculomegaly and periventricular white matter abnormalities; however, CC involvement has been rarely described [4-6]. In our case, restricted diffusion in the genu and splenium of the CC likely represents pWD, supported by several observations. First, the 11-day interval between respiratory compromise and MRI is consistent with the reported timeframe for pWD following hypoxic-ischemic injury in neonates, which typically ranges from one to two weeks [9,10]. Second, mild genu atrophy observed on follow-up imaging suggests residual structural change secondary to earlier axonal injury. Third, although restricted diffusion in the splenium can occasionally be an incidental finding in infants under four months, particularly on 3T MRI, this is unlikely in our patient because a 1.5T scanner was used, where the reported prevalence is very low (~3%) [11].
The small lesion observed in the left periventricular white matter may also reflect focal hypoxic-ischemic injury, possibly occurring in parallel with the axonal changes in the CC. This finding is consistent with earlier reports describing periventricular white matter involvement in CDM [4-6] and may indicate that both focal and tract-specific injuries can occur in the neonatal period.
The differential diagnosis included mild encephalitis/encephalopathy with a reversible splenial lesion (MERS), which can present with transient splenial diffusion restriction [12,13]. However, in neonates, incomplete myelination reduces the likelihood of intramyelinic edema, the presumed mechanism of MERS [12]. Other causes, such as viral infections, including human parechovirus, metabolic disorders, or postictal changes, were not supported by clinical history or laboratory findings. Taken together, these considerations support the interpretation that the observed CC lesions might reflect pWD in the context of CDM complicated by hypoxic-ischemic insult.
This report has some limitations. CDM results from large CTG repeat expansions in the 3′ untranslated region of the myotonic dystrophy protein kinase gene, causing multisystem involvement that includes both skeletal muscle and the central nervous system [1-3]. In particular, the immature white matter tracts in CDM may exhibit intrinsic vulnerability due to abnormal axonal development, potentially predisposing the CC to injury even in the absence of severe hypoxia [4,6]. Nevertheless, the neonatal presentation often features profound hypotonia and respiratory insufficiency, both of which increase susceptibility to hypoxic events. In this case, the observed brain changes may reflect an interplay between intrinsic vulnerability of white matter tracts and secondary hypoxic-ischemic injury; however, the possibility that the lesions were purely hypoxia-related cannot be excluded, as detailed neonatal observations were not available.
Conclusions
This case suggests that restricted diffusion in the genu and splenium of the CC may represent early axonal injury in neonates with congenital myotonic dystrophy, potentially reflecting both intrinsic vulnerability of white matter tracts and secondary hypoxic-ischemic injury in the setting of respiratory compromise. Although not definitive, MRI findings such as these could provide early imaging evidence of central nervous system involvement in CDM. Further studies are warranted to clarify their diagnostic value and long-term clinical implications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Myotonic dystrophy type I in childhood Long-term evolution in patients surviving the neonatal period Eur J Paediatr Neurol Echenne B Rideau A Roubertie A 2102231220081789295810.1016/j.ejpn.2007.07.014 · doi ↗ · pubmed ↗
- 2Congenital myotonic dystrophy: Canadian population-based surveillance study J Pediatr Campbell C Levin S Siu VM 12012516320132341561710.1016/j.jpeds.2012.12.070 · doi ↗ · pubmed ↗
- 3Prenatal, neonatal, and early childhood features in congenital myotonic dystrophy J Neuromuscul Dis Zapata-Aldana E Ceballos-Sáenz D Hicks R Campbell C 331340520183001014110.3233/JND-170277 · doi ↗ · pubmed ↗
- 4Brain magnetic resonance image changes in a family with congenital and classic myotonic dystrophy Brain Dev Kuo HC Hsiao KM Chen CJ 2912962720051586219310.1016/j.braindev.2004.09.002 · doi ↗ · pubmed ↗
- 5Brain involvement in myotonic dystrophies: neuroimaging and neuropsychological comparative study in DM 1 and DM 2J Neurol Romeo V Pegoraro E Ferrati C 1246125525720102022177110.1007/s 00415-010-5498-3 · doi ↗ · pubmed ↗
- 6White matter lesions detected by magnetic resonance imaging in neonates and children with congenital myotonic dystrophy Pediatr Neurol Peglar LM Nagaraj UD Tian C Venkatesan C 64699620193100547710.1016/j.pediatrneurol.2019.03.004 · doi ↗ · pubmed ↗
- 7Diffusion-weighted imaging of the brain in infants and children Pediatr Radiol Robertson RL Glasier CM 7497683720071758983710.1007/s 00247-007-0515-0 · doi ↗ · pubmed ↗
- 8Clinical and magnetic resonance imaging features in acute ischemic stroke with early wallerian degeneration: a case-control study BMC Neurol Ota K Nakazato Y Seo K 1702520254024724110.1186/s 12883-025-04179-4PMC 12004872 · doi ↗ · pubmed ↗