Culture-Negative Infective Endocarditis Post-mitral Valve Repair: A Case Illustrating the Role of Advanced Imaging in Surgical Decision-Making
Kayla West, Margaret Ho, Pristine Floyde, Alexander Kraev, K. Dean Gubler, Shunsuke Aoi

TL;DR
This case report highlights how advanced imaging can help diagnose endocarditis in a patient with a history of mitral valve repair and stroke, even when blood tests are negative.
Contribution
The paper emphasizes the diagnostic value of advanced imaging in atypical cases of endocarditis with stroke as the sole symptom.
Findings
Advanced imaging identified valve abnormalities in a patient with negative blood cultures and recurrent stroke.
Dynamic imaging findings prompted surgical intervention before microbiologic confirmation.
Stroke can be the sole manifestation of endocarditis in patients with prior valvular repair.
Abstract
Endocarditis is a rare but serious condition that can occur in patients with valvular heart disease, particularly after valvular repair or in those with prosthetic heart valves. While it is generally considered less common following successful valvular repairs without evidence of active infection, endocarditis can present in a variety of ways, including as an incidental finding in patients with stroke. Stroke in the setting of endocarditis is often caused by embolic events originating from infected valve leaflets or vegetations. Although blood cultures remain the gold standard for diagnosing infective endocarditis, negative blood cultures are not uncommon, particularly in early or indolent cases. Advanced imaging modalities, such as transesophageal echocardiography (TEE) and cardiac computed tomography (CT), play a crucial role in identifying valve abnormalities, vegetations, and other…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
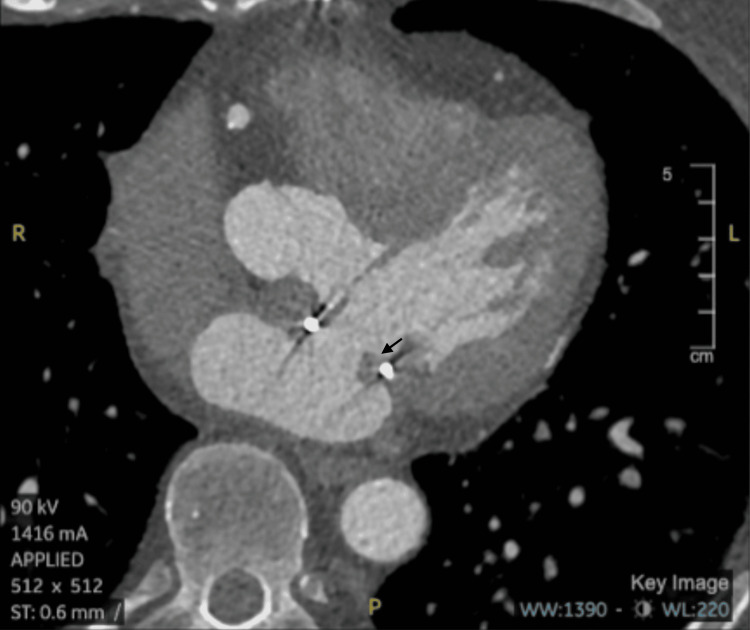 Figure 1
Figure 1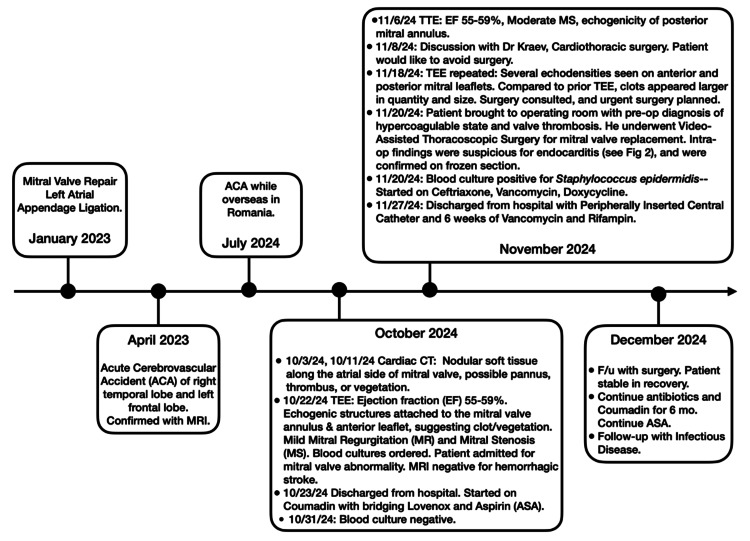 Figure 2
Figure 2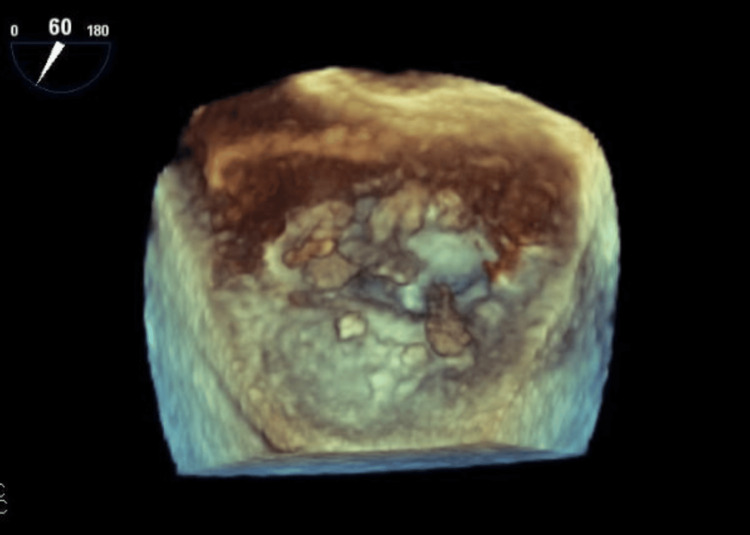 Figure 3
Figure 3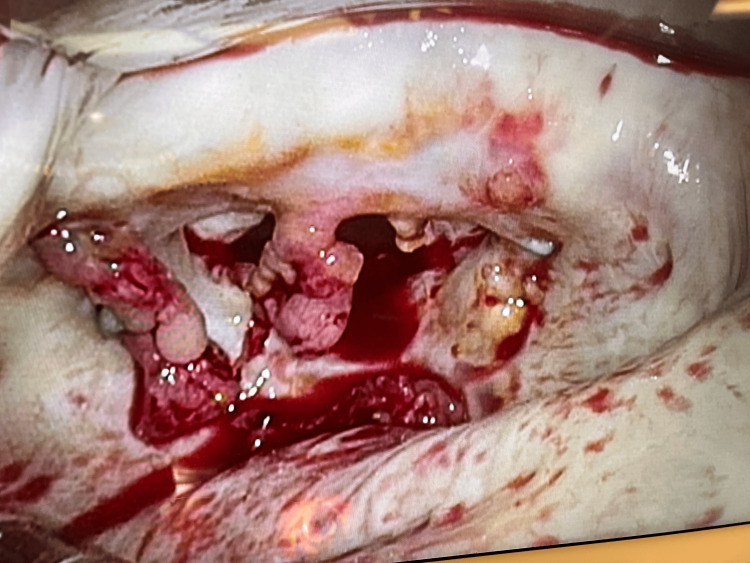 Figure 4
Figure 4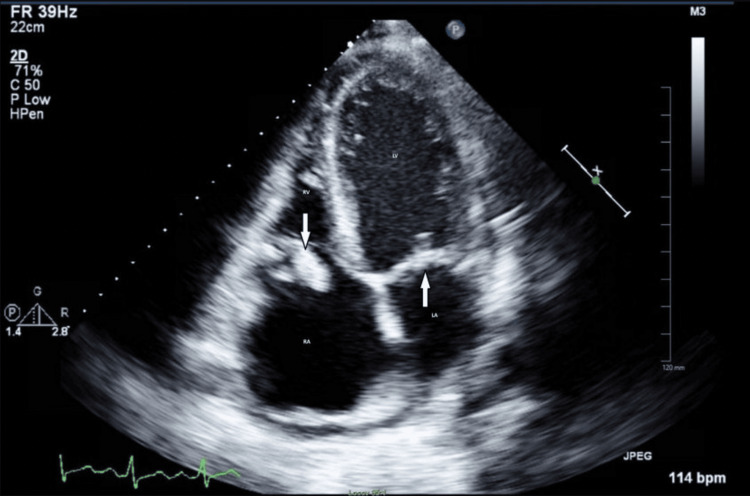 Figure 5
Figure 5| Category | Criteria |
| Major | Blood Culture Positive |
| Major | Evidence of IE |
| Minor | Predisposing Heart Condition |
| Minor | Fever |
| Minor | Vascular Phenomenon |
| Minor | Immunologic Phenomenon |
| Minor | Microbiologic Evidence |
| Pathologic | Microorganism in a vegetation |
| Pathologic | Pathologic Lesion |
| Characteristic | CT | TTE | TEE |
| Sensitivity | ~64% | ~70% | ~92-96% |
| Specificity | ~88% | ~91-98% | ~95-100% |
| Utility in Diagnosis | Used primarily for detecting complications (abscesses, septic emboli, paravalvular extension) and structural anomalies | First-line test for screening, helpful for assessing valve motion and vegetations | Gold standard for detecting vegetations, abscesses, and valve perforations |
| Invasiveness | Non-invasive | Non-invasive | Invasive (requires sedation) |
| Image Quality | High-resolution, can identify emboli, abscesses, paravalvular extension and other complications | Good for vegetations, but less clear for small lesions or abscesses | High-quality, excellent for visualizing small vegetations and valve abnormalities |
| Limitations | Limited in detecting vegetations on the valves, but excellent for abscesses and emboli | Can miss small vegetations or abscesses, less effective in obese patients | Requires expertise, not always available in emergency settings |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Valve Diseases and Treatments · Infectious Aortic and Vascular Conditions
Introduction
This article was previously presented as a poster at the 2025 Association of Military Osteopathic Physicians and Surgeons on February 20, 2025. Infective endocarditis (IE) remains a life-threatening disease with high morbidity and mortality, particularly in patients with predisposing factors such as prosthetic heart valves, congenital heart disease, prior valvular repair, or intravenous drug use [1]. Despite advances in medical and surgical management, diagnosing IE remains challenging, especially when traditional clinical criteria are inconclusive. The modified Duke criteria, which incorporate clinical, microbiologic, and imaging findings, serve as the primary diagnostic tool but have notable limitations in prosthetic valve disease and culture-negative infections [2]. This challenge is particularly relevant in patients with prior mitral valve repair, where residual valvular changes or non-infectious thrombotic material can complicate imaging interpretation.
One of the most concerning complications of IE is embolic stroke, occurring in up to 20-40% of cases [3]. Stroke in the context of IE is typically caused by septic embolization of valvular vegetations to the cerebral vasculature. While embolic stroke is often accompanied by systemic signs of infection, such as fever and leukocytosis, some patients present with cerebrovascular events as their initial or sole manifestation. This atypical presentation can delay diagnosis, particularly when blood cultures remain negative. Culture-negative endocarditis, accounting for approximately 10% of cases, presents an additional diagnostic hurdle and is often due to prior antibiotic exposure or infection with fastidious organisms that are difficult to isolate [2,4]. Given the potential for devastating neurologic outcomes, prompt recognition and early intervention are critical in patients with suspected embolic stroke secondary to IE.
In recent years, advanced imaging modalities have become increasingly vital in evaluating endocarditis, particularly when standard diagnostic criteria are inconclusive. Techniques such as transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), and cardiac computed tomography (CT) are commonly used; however, in patients with prior mitral valve repair or prosthetic valves, differentiating infectious vegetations from non-infectious findings like pannus or thrombus remains challenging [5,6]. In these cases, supplementary imaging tools are often necessary to enhance diagnostic accuracy and guide clinical decision-making.
This case underscores the complexities of diagnosing infective endocarditis in a patient with an atypical presentation. It highlights the challenges posed by negative blood cultures and the absence of classic infectious signs, emphasizing the critical role of advanced imaging in guiding clinical management. Additionally, it explores the importance of maintaining a high index of suspicion for endocarditis in patients with embolic stroke and a history of valvular intervention. This report discusses diagnostic challenges, the role of multimodal imaging, and implications for clinical care in such cases.
Case presentation
A 63-year-old male with a history of hypertension, obstructive sleep apnea, dyslipidemia, and mitral valve repair in 2023 presented to his primary care physician with multiple presyncopal episodes, several months after experiencing his second cerebral infarction in July 2024, following a prior stroke in April 2023. Given his recurrent embolic events and history of mitral valve repair, his primary care physician ordered a cardiac CT with and without contrast to evaluate for potential cardiac sources of embolism. Notably, additional risk factors included a recent dental procedure, poor dental hygiene, recent colonoscopy, with no history of injection drug use or other immunocompromising conditions. A few possible etiologies under consideration included IE, thrombus formation in the setting of a hypercoagulable state, pannus overgrowth, and cardioembolic stroke secondary to arrhythmia. The CT identified abnormal soft tissue around the prosthetic mitral annulus but was unable to definitively differentiate between pannus, thrombus, or vegetation (see Figure 1). Due to the uncertainty, a TEE was recommended for further evaluation (see Figure 2 for timeline of events).
Cardiac Computed Tomography Imaging of the Prosthetic Mitral ValveAxial computed tomography image demonstrating abnormality around the prosthetic mitral valve repair, including early pannus formation and possible thrombus or vegetation. Image was obtained from the patient with their permission.
Timeline of Medical Events Chronological overview of the patient’s cerebrovascular events, imaging studies, and interventions related to suspected infective endocarditis. Key dates include initial stroke (April 2023), recurrent stroke (July 2024), cardiac CT and transesophageal echocardiography (TEE) evaluations, follow-up imaging, and eventual surgical intervention. Figure Credits: Kayla West, primary author.
The patient underwent a TEE 11 days later, which identified an echogenic structure attached to the mitral annulus and anterior leaflet, concerning for either clot or vegetation (see Figure 3). Left ventricular function was preserved, with an ejection fraction of 55-59% with moderate mitral stenosis and mild tricuspid regurgitation. Given these findings and the patient's history of embolic strokes, his cardiologist recommended urgent evaluation in the emergency department for further workup, including blood cultures and a brain magnetic resonance imaging (MRI) to assess for any new infarcts. The MRI revealed chronic lacunar infarcts, bilateral thalami and left cerebellum with no acute infarcts. Additionally, three sets of blood cultures on 10/22/2024 remained negative at that time.
Transesophageal Echocardiography (TEE) of the Prosthetic Mitral ValveTEE images showing echogenic structures attached to the atrial aspect of the anterior and posterior mitral leaflets, concerning for thrombus or vegetation. Image was obtained from the patient with their permission.
A previously scheduled TTE was performed during his admission, showing findings similar to those noted on TEE: confirmed echodensity, immobile structure suggestive of either chronic clot/scar or healed vegetation. Given the diagnostic uncertainty and concern for potential endocarditis versus noninfectious thrombotic material, the case was discussed with the cardiothoracic surgery team. After extensive discussion, the patient opted to defer immediate surgical intervention and instead follow up with a repeat TEE in approximately one month to assess for interval changes.
The follow-up TEE demonstrated several new echodensities attached to the atrial aspect of both the anterior and posterior mitral leaflets. Compared to his prior study, the lesions had increased in size and number, raising further concern for an ongoing pathological process. Importantly, the patient’s initial blood cultures were negative, consistent with early, culture-negative endocarditis. Serial imaging over the ensuing weeks demonstrated enlarging echodensities on the mitral valve, highlighting dynamic changes in valve pathology. Given the high risk of embolization and mortality associated with potential clot dislodgment, these progressive imaging findings - rather than laboratory confirmation alone - were the primary driver of the decision to proceed with mitral valve replacement. After further discussions with his cardiologist and cardiothoracic surgery team, he consented to the procedure.
Following surgical intervention, intraoperative findings confirmed friable material on the mitral valve leaflets, and subsequent blood cultures several days later returned positive for *Staphylococcus epidermidis *(see Figure 4). Pathologic examination of the intraoperative biopsy was consistent with infective endocarditis caused by Staphylococcus epidermidis. This case highlights the challenges in diagnosing culture-negative endocarditis and underscores the importance of multimodal imaging and a high index of suspicion in patients with recurrent embolic strokes and prior valvular intervention.
Endocarditis VegetationsIntraoperative view of the mitral valve showing friable vegetations consistent with infective endocarditis. Image obtained from the patient’s surgical record and used with permission; adapted for this article.
Discussion
This case illustrates an atypical presentation of IE in a patient with a history of mitral valve repair. Unlike classical cases of Staphylococcus epidermidis IE, which typically present with fever, leukocytosis, and positive blood cultures, this patient was afebrile, hemodynamically stable, and had persistently negative blood cultures. Notably, the patient did not initially meet the modified Duke criteria for definitive IE: three major criteria, one major and three minor, or five minor criteria (see Table 1) [2]. At the time of initial evaluation, only two of the five minor clinical criteria were satisfied, including predisposing valvular disease and embolic stroke, with standard CT imaging unable to definitively identify the presenting abnormality on the initial valve repair.
The modified Duke criteria, while widely used, have reduced sensitivity in cases involving prosthetic valves and culture-negative infections. This patient’s eventual diagnosis was only established postoperatively, after intraoperative pathology and valve cultures confirmed S. epidermidis infection. With modern, stringent surgical precautions, S. epidermidis is an unusual pathogen for culture-negative IE. This highlights a critical diagnostic gap, as culture-negative endocarditis constitutes up to 10% of IE cases and often necessitates reliance on clinical suspicion and advanced imaging [7]. Its identification in this case highlights the potential for the persistence of indolent infections in prosthetic material, particularly in the absence of systemic symptoms.
The role of advanced imaging modalities cannot be overstated, especially when standard diagnostic criteria are inconclusive. While clinical evaluation and history provided initial context, imaging modalities such as CT, TEE, and TTE were pivotal in diagnosing and guiding management. Each modality offers unique strengths and limitations in assessing prosthetic valve endocarditis, necessitating careful selection based on clinical suspicion and diagnostic yield (see Table 2) [4,5]. Figures 1, 3 show the patient’s actual cardiac scans and images, while Figure 5 presents a representative example image for comparison [8]. Initial CT imaging provided a broad overview, detecting abnormality of the prosthetic valve, but lacked the resolution to differentiate between pannus, thrombus, or vegetation. Initial TTE and TEE identified echogenic structures attached to the mitral annulus and anterior leaflet; however, they were unable to differentiate between clot and vegetation. It was ultimately a follow-up TEE that demonstrated progressive and newly developing echodensities of the atrial aspect of both anterior and posterior mitral leaflets that led to escalation of care, surgical intervention, and eventual diagnosis of culture-negative IE despite the absence of major Duke criteria and most of the minor criteria. This finding emphasizes the critical importance of repeated imaging in difficult cases and suggests that dynamic changes over time may serve as an important clinical marker, particularly when microbiologic data is inconclusive. TEE remains the gold standard for evaluating prosthetic valve endocarditis due to its superior sensitivity and resolution compared to TTE. Cardiac CT serves as a valuable adjunct, particularly for detecting complications or for evaluating surrounding structures, but cannot replace the role of TEE in suspected IE.
Transthoracic Echocardiography (TTE) of the Tricuspid and Mitral ValveRepresentative TTE image illustrating tricuspid and mitral vegetations noted on apical four-chamber view. Image reproduced with permission from the original publisher [8].
Emerging diagnostic approaches, such as molecular methods (organism-specific polymerase chain reaction (PCR), broad-range 16S rRNA PCR, targeted or shotgun metagenomic sequencing) and radiotracer-based imaging, represent promising tools for the future diagnosis of infective endocarditis [9]. These were not reviewed in depth here, as our focus was on established imaging modalities (CT, TTE, and TEE) most relevant to the clinical course of the present case.
This case also highlights several important teaching points for clinicians managing prosthetic valve patients. First, stroke may be the sole presenting manifestation of endocarditis in patients with prosthetic valves, even in the absence of fever or positive blood cultures. Second, vegetations may be missed initially, especially on standard imaging, necessitating serial and repeated imaging to detect dynamic changes over time. Third, surgical intervention may be required prior to microbiologic confirmation, as progressive imaging findings and risk of embolization can justify early operative management. Finally, culture-negative endocarditis underscores the importance of integrating clinical suspicion, imaging, and patient risk factors rather than relying solely on laboratory confirmation. Collectively, these points reinforce the critical role of dynamic imaging and clinical vigilance in guiding timely intervention for prosthetic valve endocarditis.
Conclusions
This case of culture-negative IE due to S. epidermidis highlights critical diagnostic challenges. The patient’s atypical presentation - absence of systemic infection signs, negative blood cultures, and initial imaging uncertainty - resulted in delayed diagnosis and appropriate care, exposing the limitations of current diagnostic frameworks such as the Duke criteria, particularly in patients with prosthetic valves or prior valvular repairs. This patient’s eventual diagnosis was heavily reliant on serial imaging, which reinforces the importance of maintaining a high suspicion for IE in patients who present with embolic phenomena and a history of prosthetic material, regardless of blood culture results.
Furthermore, this case demonstrates the benefits of the adjunction of varying imaging modalities: TTE and cardiac CT for initial screening and anatomic clarification, and TEE for high-resolution detection of valvular pathology. Timely serial imaging - alongside multidisciplinary collaboration - was paramount in achieving the correct diagnosis and guiding effective treatment. It was diagnostic suspicion by the patient’s care team and early surgical intervention guided by imaging findings, rather than traditional microbiologic criteria alone, that proved to be superior in providing life-saving treatment.
Emerging molecular diagnostic techniques, such as organism-specific PCR and metagenomic sequencing, may in the future provide earlier microbiologic confirmation of infective endocarditis. While not yet widely available due to cost, these methods have the potential to complement imaging and traditional microbiology, improving diagnostic accuracy and enabling earlier intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 12020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J Am Coll Cardiol Otto CM Nishimura RA Bonow RO 077202110.1016/j.jacc.2020.11.03533342587 · doi ↗ · pubmed ↗
- 2The 2023 Duke-International Society for Cardiovascular Infectious Diseases criteria for infective endocarditis: updating the modified Duke criteria Clin Infect Dis Fowler VG Durack DT Selton-Suty C 5185267720233713844510.1093/cid/ciad 271PMC 10681650 · doi ↗ · pubmed ↗
- 3Systemic embolization in infective endocarditis Indian J Thorac Cardiovasc Surg Kildahl HA Brenne EL Dalen H Wahba A 40464020243882755510.1007/s 12055-023-01616-2PMC 11139814 · doi ↗ · pubmed ↗
- 4ACR Appropriateness Criteria® infective endocarditis J Am Coll Radiol Malik SB Hsu JY Hurwitz Koweek LM 06118202110.1016/j.jacr.2021.01.01033958118 · doi ↗ · pubmed ↗
- 5Imaging to evaluate suspected infective endocarditis Cleve Clin J Med Haq IU Haq I Griffin B Xu B 1631728820213364896910.3949/ccjm.88a.19142 · doi ↗ · pubmed ↗
- 6Surgery for mitral valve disease: degenerative replacement Essentials of Operative Cardiac Surgery Hartley P Kyriazis PG Punjabi PP 107124 Cham Springer 2022
- 7Infective endocarditis Nat Rev Dis Primers 8 2025 Holland TL Baddour LM Bayer AS Hoen B Miro JM Fowler VG Jr 16059220162758241410.1038/nrdp.2016.59PMC 5240923 · doi ↗ · pubmed ↗
- 8Cryptococcus neoformans infective endocarditis of native valves in an immunocompetent host ID Cases Roy M Ahmad S Roy AK 66701220182990462210.1016/j.idcr.2018.03.002PMC 6000992 · doi ↗ · pubmed ↗