Beyond the Break: Radiologic Diagnosis and Outcomes of Necrotizing Fasciitis Complicating Orthopedic Fractures
Kiranjot Kaur, Muhammad Zain Ul Abidin, Shahmeen Rasul, Ahmed M Mohamed, Karthika Kalissery Biju Chandrasekhar, Shenouda R Shehata Abdelmesih, Jarallah H. J. Alkhazendar, Faiqa Ijaz, Aliaa H Alkhazendar, Riyan Khalid, Mohit H Buch

TL;DR
Necrotizing fasciitis complicating orthopedic fractures is rare but deadly, with poor outcomes and a need for better diagnostic and reporting standards.
Contribution
This study systematically reviews the radiologic diagnosis and outcomes of necrotizing fasciitis in orthopedic fracture patients.
Findings
CT and MRI are critical for diagnosing fascial necrosis, especially under immobilization casts.
Fracture-associated necrotizing fasciitis has a high mortality rate, with most reported cases resulting in death or amputation.
Systemic complications like acute kidney injury are underreported despite their importance in prognosis.
Abstract
Necrotizing fasciitis (NF) is a rapidly progressive infection with high mortality. When NF complicates orthopedic fractures, early recognition is particularly challenging because swelling, erythema, and pain may be misattributed to trauma or postoperative changes. A systematic review was conducted using PubMed, Embase, Scopus, and Cochrane databases up to June 2025 according to Preferred Reporting Items for Systematic reviews and Meta-Analyses 2020 guidelines. Eligible studies included human patients with orthopedic fractures complicated by NF in whom radiologic evaluation and clinical outcomes were reported. Risk of bias was assessed using the Joanna Briggs Institute checklist for case reports. Six studies were included, comprising six individual patients with fracture-associated NF. Radiologic evaluation revealed that plain radiographs occasionally demonstrated subcutaneous gas, while…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
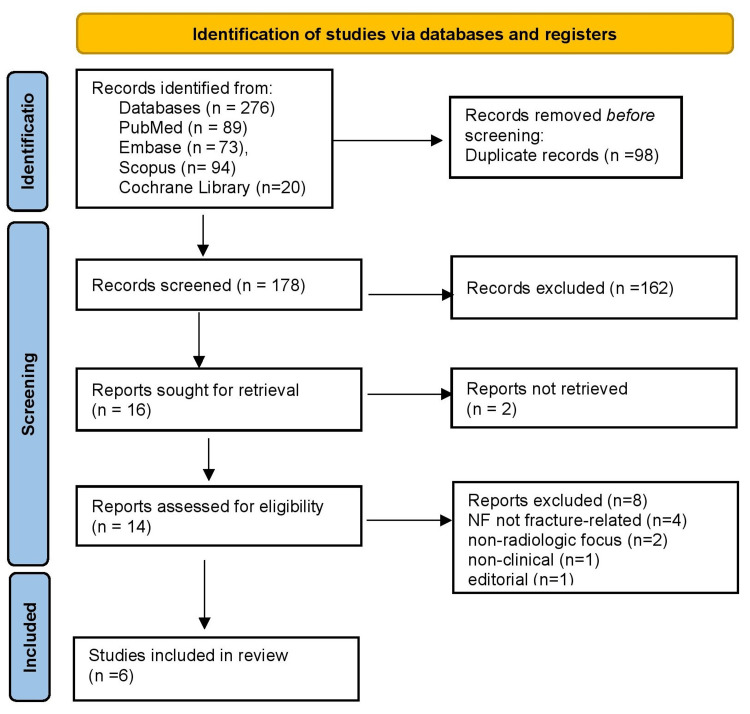 Figure 1
Figure 1| Authors and year | Population (P) | Exposure/Condition (I) | Comparator (C) | Outcomes of NF (O) | Pathophysiological findings | Anatomical impact | Radiologic diagnosis |
| Shang et al., 2017 [ | Older adult with tibial fracture | Tibial shaft fracture treated with MIPO/ORIF → postoperative NF | None | Death from septic shock and multi-organ failure | Diabetes, immunosuppression, and bacterial toxin-mediated spread | Deep fascia and subcutaneous tissue necrosis; rapid extension | Radiographs showed soft tissue gas; CT revealed fascial fluid and gas |
| Joomun et al., 2020 [ | A 56-year-old diabetic female with polytrauma | Hip fracture fixation (ORIF) → incisional NF with abdominal extension | None | Serial debridements, NPWT, and eventual death from sepsis | Idiopathic NF after sterile fixation; systemic inflammatory cascade | Necrosis along the fascial planes from the hip wound to the abdominal wall | CT demonstrated fascial thickening and subcutaneous gas; X-ray was less sensitive |
| Patil et al., 2021 [ | A 48-year-old male with a proximal tibia fracture | Proximal tibia fracture complicated by NF, managed with external fixation | None | Limb salvage achieved; fracture united at 18 months | Polymicrobial invasive necrosis; host immune compromise | Extensive skin, fascia, and periosteum with exposed bone | X-rays revealed soft tissue swelling; intraoperative correlation confirmed the diagnosis |
| Hong et al., 2018 [ | An adult with a type I open tibial fracture | Open tibial fracture in aquatic setting → fulminant NF ( | None | Rapid death within days despite debridement and ICU care | Virulent aquatic pathogen; rapid toxin and sepsis | Lower-limb fascia and muscle necrosis extending proximally | CT demonstrated extensive soft tissue gas and fascial involvement |
| Weidle et al., 2009 [ | A 77-year-old female with a distal radius (Colles’) fracture | Closed distal radius fracture → upper-limb NF | None | Amputation at the shoulder; death from septic shock | Group A | Entire upper-limb fascial compartments destroyed | Radiographs showed extensive soft tissue gas spreading beyond the fracture site |
| Netzer et al., 2009 [ | A 43-year-old female with a tibial fracture immobilized in a cast | Tibial shaft fracture in plaster cast → NF under cast | None | Early debridement, survival, and limb salvage with prolonged recovery | Cast pressure/ischemia enabled bacterial invasion; hypoxia promoted necrosis | Fascia and subcutaneous tissues of the leg beneath the cast | Plain radiograph initially inconclusive; MRI confirmed fascial edema and necrosis |
| Study | Study design | Risk of bias tool | Risk of bias rating | Justification |
|
Shang et al., 2017 [ | Case report | JBI case report checklist | High | Single case; outcome influenced by multiple comorbidities; limited imaging detail |
|
Joomun et al., 2020 [ | Case report | JBI case report checklist | High | Single case; systemic complications; renal outcomes not reported; potential reporting bias |
|
Patil et al., 2021 [ | Case report | JBI case report checklist | High | Single patient; publication bias toward successful limb salvage; incomplete generalizability |
|
Hong et al., 2018 [ | Case report | JBI case report checklist | High | Fatal case; very rapid course; limited detailed radiology; ecological exposure unique |
|
Weidle et al., 2009 [ | Case report | JBI case report checklist | High | Lethal case; no comparator; reporting limited to acute course; missing long-term follow-up |
|
Netzer et al., 2009 [ | Case report | JBI case report checklist | High | Single case; inference about pathophysiology under cast is narrative; limited imaging reproducibility |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments
Introduction and background
Necrotizing fasciitis (NF) is a rapidly progressive infection of the fascia and subcutaneous tissue, characterized by fulminant systemic toxicity and high mortality. Its global incidence is estimated at 0.3 to 5 cases per 100,000 population annually, though this may be an underestimation due to under-reporting in low- and middle-income countries [1]. Mortality rates range from 20% to 40%, despite advances in imaging, antibiotics, and surgical debridement [2]. Predisposing factors include diabetes mellitus, chronic kidney disease, immunosuppression, and peripheral vascular disease. In a cohort analysis, diabetes was present in 44% of NF cases, and renal dysfunction independently predicted mortality [3]. Anatomically, extremity involvement is most frequent, followed by truncal and perineal disease. When NF complicates orthopedic fractures, diagnosis is particularly challenging because early symptoms such as swelling, erythema, and pain are easily misattributed to trauma or postoperative change. This diagnostic ambiguity can result in catastrophic delays [4].
Radiologic evaluation plays a critical role. Plain radiographs may show subcutaneous emphysema but have limited sensitivity. CT offers better detection of fascial gas and fluid tracking, while MRI remains the most sensitive tool for mapping fascial edema and necrosis [5]. Ali et al. (2013) confirmed that MRI is highly valuable for diagnosing NF, with deep intermuscular T2 hyperintensity and fascial thickening serving as key differentiators from cellulitis or myositis. Contrast-enhanced sequences further aid early detection, enabling timely and effective management [6]. Despite MRI’s high sensitivity, it has been emphasized that radiology should complement, not replace, clinical suspicion. Recent prognostic studies highlight that renal impairment, advanced age, and delayed debridement are consistent predictors of mortality [7].
This systematic review aims to synthesize current evidence on radiologic diagnosis and clinical outcomes of NF complicating orthopedic fractures, with special attention paid to anatomical extent, pathophysiology, and renal involvement. By consolidating the limited literature, this review aims to highlight knowledge gaps and provide a foundation for future multicenter investigations.
Review
Methodology
Search Strategy
This systematic review adhered to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines to ensure methodological rigor [8]. A comprehensive search was conducted in four electronic databases: PubMed/MEDLINE, Embase, Scopus, and the Cochrane Library, covering all records published up to June 30, 2025. The strategy combined controlled vocabulary terms (e.g., MeSH and Emtree) with free-text keywords, linked with Boolean operators. For PubMed, the search string included terms for the condition (“necrotizing fasciitis,” “necrotising fasciitis,” “necrotizing soft tissue infection”), the exposure (“fracture,” “orthopedic fracture,” “open fracture,” “internal fixation,” “external fixation,” “plaster cast”), radiologic modalities (“radiography,” “X-ray,” “computed tomography,” “CT,” “magnetic resonance imaging,” “MRI”), and outcomes (“treatment outcome,” “mortality,” “amputation,” “renal failure,” “acute kidney injury”). Similar search syntax was adapted for Embase, Scopus, and Cochrane, using Emtree and title/abstract fields where appropriate. Boolean operators were used to refine the search; for example, (“necrotizing fasciitis” OR “necrotising fasciitis”) AND (fracture OR “orthopedic fracture”) AND (radiography OR CT OR MRI) AND (mortality OR amputation OR renal failure). Searches were limited to human studies and English-language publications. To ensure completeness, reference lists of included studies and relevant reviews were manually screened. Grey literature, such as conference abstracts and editorials, was excluded due to insufficient clinical or radiologic data.
Eligibility Criteria
Eligibility was defined using the PICO framework [9]. The Population (P) included human patients of any age with an orthopedic fracture, such as open or closed, treated operatively or conservatively, who subsequently developed NF at or near the fracture site. The Intervention/Exposure (I) was fracture-associated NF with radiologic evaluation using plain radiography, CT, or MRI. No formal Comparator (C) was required, but studies contrasting NF with other soft tissue infections were considered relevant. The Outcomes (O) of interest included radiologic features, anatomical extent, clinical endpoints such as limb salvage, amputation, or mortality, and systemic complications, including acute kidney injury.
We included original reports (case reports, case series, and observational studies) published in the English language that provided full-text patient-level data, described radiologic findings, and documented clinical outcomes. Exclusions were animal or cadaveric studies, in vitro studies, reviews, editorials, letters, and abstracts lacking outcome data. Reports of NF unrelated to fractures or confined to non-orthopedic contexts (e.g., Fournier’s gangrene) were also excluded, as were duplicate publications without new information. Although inclusion of single-patient reports inherently carries a high risk of bias, this was justified by the extreme rarity of fracture-associated NF, making such evidence the only available basis for synthesis.
Study Selection
Two reviewers independently screened titles/abstracts. Full texts of eligible studies were retrieved and evaluated. Discrepancies were resolved by consensus.
Data Extraction
Data were independently extracted by two reviewers. Information collected included study characteristics (author, year, design), patient demographics, fracture type, radiologic modality and findings, clinical outcomes such as amputation or mortality, and systemic complications, with an emphasis on renal involvement. Any discrepancies in extraction were resolved through discussion to ensure accuracy. Data consistency was further verified by cross-checking across both reviewers. This process minimized errors and maintained methodological rigor.
Risk of Bias Assessment
Risk of bias for the included studies was evaluated using the Joanna Briggs Institute (JBI) checklist for case reports [10]. Each study was assessed for clarity of patient description, diagnostic certainty, outcome reporting, and potential confounding factors. Studies were rated as high risk when reporting was incomplete, comparators were absent, or systemic outcomes were poorly documented. Two reviewers performed independent assessments, and discrepancies were resolved by consensus. This ensured a transparent and standardized evaluation of study quality.
Data Synthesis
Given the rarity of fracture-associated NF, all included studies were case reports, preventing quantitative pooling. A narrative synthesis was therefore undertaken, grouping findings by fracture type, radiologic diagnosis, outcomes, and systemic involvement. Frequencies were described in simple proportions (e.g., deaths, amputations, limb salvage). Radiologic features were compared across modalities to identify consistent diagnostic markers. This qualitative approach highlighted recurring clinical patterns while acknowledging the inherent heterogeneity of single-case evidence.
Results
Study Selection Process
The PRISMA flow diagram is shown in Figure 1. We identified 276 records through database searching: PubMed (n = 89), Embase (n = 73), Scopus (n = 94), and the Cochrane Library (n = 20). After removing 98 duplicate records, 178 unique records remained for screening. Title/Abstract screening excluded 162 records. We sought full texts for 16 reports, of which two were not retrievable. Thus, 14 reports were assessed for eligibility, of which eight were excluded as they did not meet eligibility criteria (e.g., NF not fracture-related, non-radiologic focus, non-clinical, editorial). Six (n = 6) studies met all criteria and were included in the final review.
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 flow diagram.
Characteristics of the Selected Studies
In total, six studies met the inclusion criteria, each representing a single patient with NF complicating an orthopedic fracture. Shang et al. (2017) described an older adult with a tibial shaft fracture treated with minimally invasive plating who developed postoperative NF, ultimately dying from septic shock. Radiographs showed soft-tissue gas, while CT revealed fascial fluid collections [11]. Joomun et al. (2020) reported the case of a 56-year-old diabetic woman with polytrauma who developed incisional NF following hip fracture fixation, extending into the abdominal wall. Despite repeated debridement, the patient succumbed to sepsis, with CT demonstrating fascial thickening and gas [12]. Patil et al. (2021) described the case of a 48-year-old man with a proximal tibia fracture complicated by NF but successfully managed with external fixation and staged surgery, resulting in fracture union and limb salvage at 18 months. Radiographs showed soft tissue swelling confirmed intraoperatively [13]. Hong et al. (2018) presented a fatal case of fulminant NF due to Aeromonas hydrophila in an open tibial fracture sustained in an aquatic environment, with CT revealing extensive fascial gas and necrosis [14]. Weidle et al. (2009) detailed the case of a 77-year-old woman who developed NF after a closed distal radius (Colles’) fracture, leading to amputation and death from septic shock. Radiographs demonstrated widespread subcutaneous gas [15]. Finally, Netzer et al. (2009) reported the case of a 43-year-old woman who developed NF beneath a plaster cast following tibial fracture immobilization. She survived after early debridement, with MRI confirming fascial edema that plain radiographs failed to detect [16]. The collective findings from these cases emphasize the devastating outcomes of fracture-related NF, the frequent diagnostic value of CT and MRI, and the influence of comorbidities such as diabetes and ischemia in worsening prognosis (Table 1).
Risk of Bias Assessment
All six included studies were single-patient case reports, which inherently carry a high risk of bias. Using the JBI case report checklist, each was rated as high risk due to limitations in generalizability, incomplete outcome reporting, and lack of comparators. The study by Shang et al. (2017) was limited by multiple comorbidities and restricted imaging detail, while Joomun et al. (2020) presented systemic complications but did not report renal outcomes, raising concerns of reporting bias. Patil et al. (2021) demonstrated successful limb salvage, yet selection and publication bias reduced applicability [11-13]. Hong et al. (2018) described a rapidly fatal course with limited imaging documentation, compounded by the unique aquatic exposure [14]. Weidle et al. (2009) reported a lethal case without long-term follow-up, and Netzer et al. (2009) provided mainly narrative inferences about pathophysiology under plaster casting, with limited imaging reproducibility [15,16]. Collectively, the evidence base is constrained by case-level design, underscoring the descriptive rather than generalizable nature of available data (Table 2).
Discussion
Fracture-associated NF is a devastating complication where the initial clinical signs, such as swelling, erythema, pain, and wound discharge, are often masked by trauma or postoperative changes. This diagnostic ambiguity frequently results in delayed intervention and poor outcomes. In the six cases identified, outcomes ranged from fulminant systemic sepsis with death to survival with limb salvage. This suggests that fracture-related NF carries an intrinsically worse prognosis due to compounded risks: fracture-related soft-tissue injury, immobilization-induced ischemia, and postoperative inflammatory overlap.
Comparative analysis of these cases highlights key prognostic determinants. Shang et al. [11] and Joomun et al. [12] both reported postoperative NF following internal fixation in diabetic patients, underscoring the role of systemic comorbidities. Patil et al. [13] showed that timely recognition combined with staged external fixation allowed fracture union and functional limb salvage, making it the only long-term favorable outcome. Conversely, Hong et al. [14] illustrated the rapid lethality of Aeromonas hydrophila after aquatic exposure, consistent with prior reports that environmental organisms accelerate toxin-mediated necrosis. Weidle et al. [15] described NF after a distal radius fracture, where gas was evident on plain radiographs yet mortality ensued despite amputation, highlighting that radiographic diagnosis does not necessarily alter prognosis if systemic deterioration is advanced. Netzer et al. [16] uniquely described NF beneath a plaster cast, where MRI revealed fascial edema invisible on radiographs, and early debridement secured survival. Together, these cases show that outcomes depend on fracture site, microbial virulence, comorbidities, and above all, the timeliness of surgical intervention.
Radiologic evaluation played a pivotal role in differentiating NF from more benign postoperative complications. Plain radiographs, while occasionally diagnostic when emphysema was pronounced [15], are known to have limited sensitivity (<50%) [17]. CT proved to be the most consistently informative tool, revealing fascial gas, edema, and fluid tracking in multiple cases [11,12,14], and its accessibility in unstable patients aligns with prior evidence of CT’s utility in emergency settings [18]. MRI, as employed by Netzer et al. [16], demonstrated superior sensitivity in detecting fascial necrosis and deep tissue involvement, consistent with prior studies establishing MRI as the gold standard [19]. However, NF remains primarily a clinical diagnosis, with imaging acting as a critical adjunct rather than a replacement for surgical exploration. These findings underscore the necessity of integrating radiologic suspicion with clinical acumen, especially in fracture patients, where inflammation and swelling are expected.
Comorbidities and systemic complications further influenced outcomes. Diabetes was a prominent factor in two cases [11,12], consistent with epidemiological evidence linking diabetes to increased NF mortality. Local ischemia beneath immobilization devices, as in Netzer et al. [16], represents another underrecognized mechanism by which fracture management can predispose to NF. Meanwhile, renal dysfunction, an established independent predictor of poor outcomes, was largely unreported across the included studies. More generally, however, systemic complications are frequent in NF, including sepsis and multi-organ failure remain the leading causes of death, while acute kidney injury occurs in up to 30-40% of patients and independently predicts mortality. Additional complications such as respiratory failure, shock, and disseminated intravascular coagulation further contribute to the high morbidity and mortality associated with the disease [20].
This review is limited by the small number of cases, all being single-patient reports subject to publication bias. Radiologic details, microbiology, and systemic outcomes, especially renal involvement, were inconsistently reported, restricting robust conclusions. Therefore, the findings should be viewed as descriptive rather than generalizable.
Conclusions
Fracture-associated NF is an exceptionally rare but devastating complication, with six reported patients showing uniformly poor outcomes: four deaths, one fatality after amputation, and only one case of successful fracture union with limb salvage. Imaging supported diagnosis, but never replaced urgent surgery. CT was the most practical tool in unstable patients for detecting fascial gas, edema, and fluid tracking, while MRI provided the highest sensitivity when radiographs were inconclusive or immobilization masked findings. Prognosis was worsened by diabetes, local ischemia (including cast-related pressure), virulent organisms such as Aeromonas hydrophila, and delays to debridement. These cases highlight the need for heightened clinical suspicion in fracture patients with disproportionate pain or systemic toxicity, where CT or MRI should accelerate but not delay surgical exploration. Given that all available evidence is limited to single case reports with inconsistent reporting of systemic complications, particularly acute kidney injury, future research should prioritize standardized data collection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Necrotizing fasciitis: risk factors of mortality Risk Manag Healthc Policy Khamnuan P Chongruksut W Jearwattanakanok K Patumanond J Yodluangfun S Tantraworasin A 17820152573393810.2147/RMHP.S 77691 PMC 4337692 · doi ↗ · pubmed ↗
- 2Necrotizing fasciitis with no mortality or limb loss Am Surg Martin DA Nanci GN Marlowe SI Larsen AN 809812742008 https://pubmed.ncbi.nlm.nih.gov/18807667/18807667 · pubmed ↗
- 3Necrotizing fasciitis in patients with diabetes mellitus: clinical characteristics and risk factors for mortality BMC Infect Dis Cheng NC Tai HC Chang SC Chang CH Lai HS 4171520152646390010.1186/s 12879-015-1144-0PMC 4604726 · doi ↗ · pubmed ↗
- 4Diagnosing fracture-related infection: current concepts and recommendations J Orthop Trauma Govaert GA Kuehl R Atkins BL 8173420203185597310.1097/BOT.0000000000001614 PMC 6903359 · doi ↗ · pubmed ↗
- 5Imaging of musculoskeletal soft-tissue infections in clinical practice: a comprehensive updated review Microorganisms Spinnato P Patel DB Di Carlo M Bartoloni A Cevolani L Matcuk GR CrombéA 23291020223655758210.3390/microorganisms 10122329 PMC 9784663 · doi ↗ · pubmed ↗
- 6MRI in necrotizing fasciitis of the extremities Br J Radiol Ali SZ Srinivasan S Peh WC 201305608720142428840310.1259/bjr.20130560 PMC 3898976 · doi ↗ · pubmed ↗
- 7Epidemiology and prognostic factors of necrotizing fasciitis in resource-limited regions based on 119 cases Sci Rep Chen Y Huang Y Shou J Song R Tan J Deng J 274581520254072165110.1038/s 41598-025-13278-8PMC 12304161 · doi ↗ · pubmed ↗
- 8The PRISMA 2020 statement: an updated guideline for reporting systematic reviews BMJ Page MJ Mc Kenzie JE Bossuyt PM 0372202110.1186/s 13643-021-01626-4PMC 800853933781348 · doi ↗ · pubmed ↗