Bridging silos on a budget: how interprofessional education shapes collaborative attitudes across low-and middle-income countries - a systematic review
Urvish Joshi, Renjith Raj Puthuparampil, Sanjay Kini, Sharon Baisil

TL;DR
This review finds that interprofessional education can improve teamwork attitudes among health students in low-and middle-income countries, but more rigorous research is needed.
Contribution
The study synthesizes limited evidence on IPE's impact in LMICs, highlighting contextual factors and methodological gaps.
Findings
Four of five studies showed significant positive changes in collaborative attitudes after IPE interventions.
Positive outcomes were most common in clinically embedded and small-group IPE settings.
Methodological limitations like lack of control groups and small samples reduced evidence certainty.
Abstract
Interprofessional education (IPE) enables health-profession students from different disciplines to learn together, fostering teamwork, communication, and collaborative practice. Although widely implemented in high-income countries (HICs), evidence from low-and middle-income countries (LMICs) is limited and scattered. This systematic review synthesized quantitative evidence on the impact of IPE interventions on students’ collaborative attitudes in LMIC contexts, and explored intervention characteristics, methodological quality, and evidence gaps. Following PRISMA (2020) guidance, we searched PubMed, Scopus, and Embase (January 2010-August 2025) and screened grey literature. Eligible studies included undergraduate or pre-licensure health-profession students from at least two disciplines in LMICs, exposed to structured IPE interventions, with pre- and post-measurement of attitudes using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
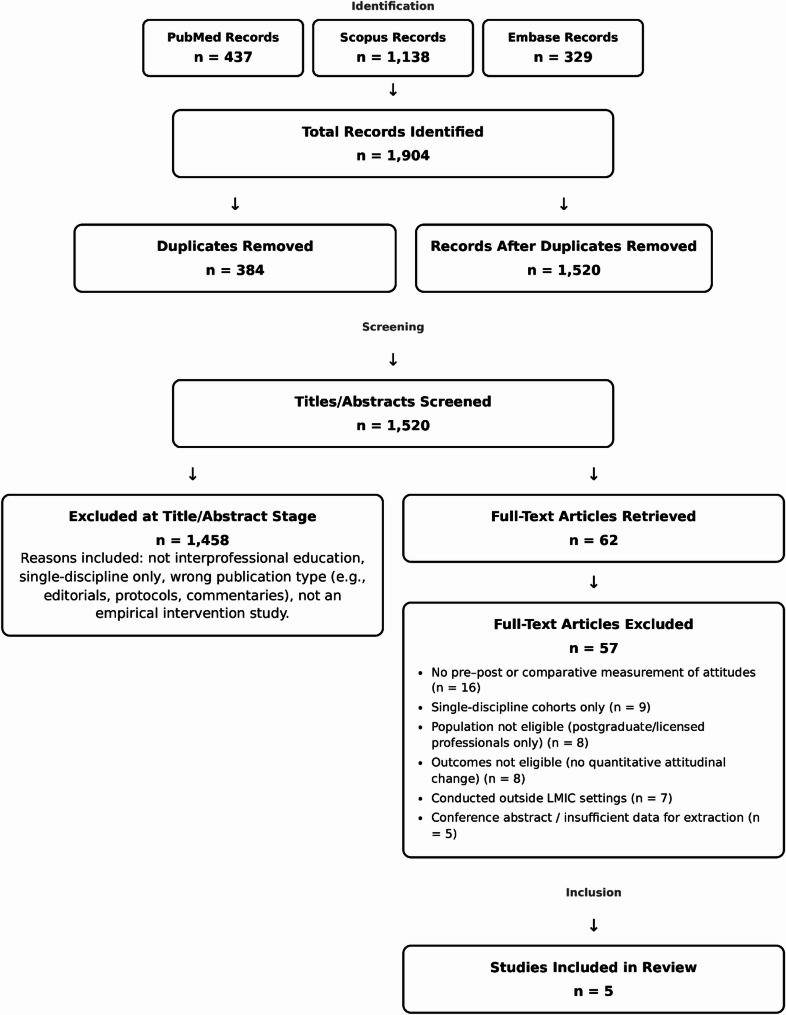 Figure 1
Figure 1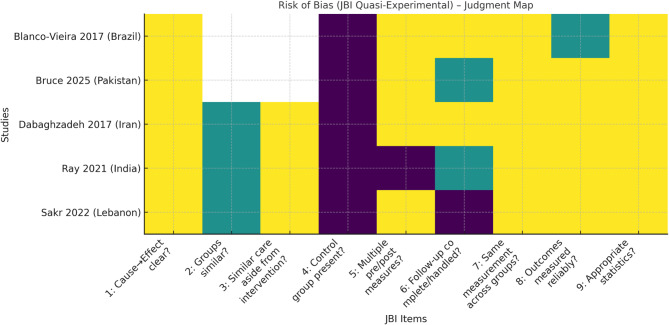 Figure 2
Figure 2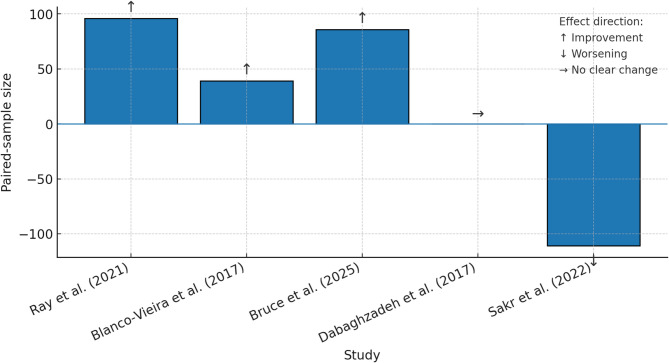 Figure 3
Figure 3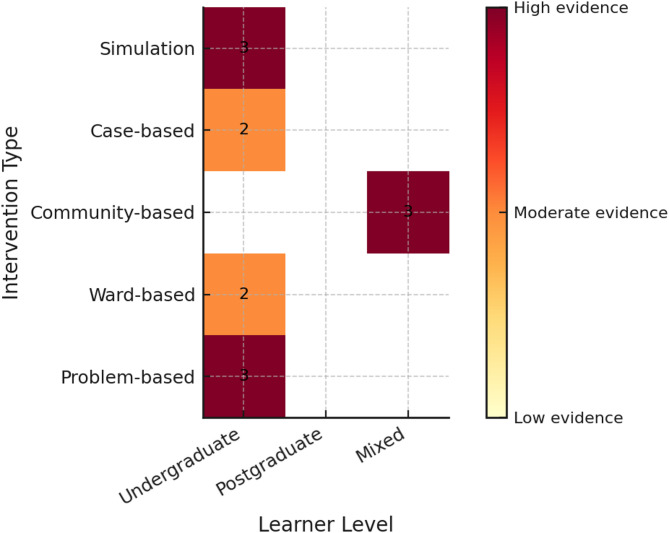 Figure 4
Figure 4- —Manipal Academy of Higher Education, Manipal
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterprofessional Education and Collaboration · Global Health and Surgery · Innovations in Medical Education
Introduction
IPE is recognized worldwide as an effective method for enhancing collaborative skills, patient safety, and health outcomes. It involves instances where students from multiple health professions learn about, from, and with each other to facilitate effective collaboration and improve health outcomes [1]. The World Health Organization’s (WHO) 2010 Framework for Action on IPE & Collaborative Practice advocates for the integration of IPE into health professional curricula to strengthen teamwork, communication, and ethical behavior [1]. HICs have made notable progress in adopting IPE, supported by established frameworks such as the Interprofessional Education Collaborative (IPEC) competencies from 2016 to 2023, which define essential areas like roles and responsibilities, interprofessional communication, teamwork, and values and ethics for collaborative practice [2, 3]. Conversely, evidence from LMICs is sparse and fragmented, with descriptive studies identifying barriers and facilitators but often lacking thorough outcome evaluation, especially for undergraduate and pre-licensure health profession students [4, 5].
Systematic reviews of IPE frequently emphasize attitudinal outcomes, such as willingness to collaborate, role comprehension, and communication skills, as immediate indicators of effectiveness, which are especially critical in LMICs due to resource constraints necessitating efficient team-based care models [1, 5]. However, most evidence derives from HICs using robust designs, while LMICs face scarcity, uncontrolled pre-post studies, lack of follow-up, and self-report biases, underscoring the need for focused synthesis on undergraduate/pre-licensure students where attitudes form early and influence future practice [5–7]. In HICs, IPE has shown sustained improvements in professional attitudes and collaborative behaviors among both students and practicing professionals, whereas graduate and continuing education often builds on existing silos; thus, this review targets undergraduates in LMICs to address the evidence gap and inform early curricular integration [6–8].
In a more recent systematic examination, Berger-Estilita et al. (2020) confirm that even in well-funded environments, assessments of medical students’ attitudes are hindered by ceiling effects and the inconsistent application of validated tools [6]. Similarly, Kitema et al.’s (2024) systematic review in sub-Saharan Africa points out issues such as limited outcome reporting, small sample sizes, and inconsistent study designs, underscoring the necessity for synthesizing quantitative changes in attitudes within LMIC contexts [5].
These results highlight a significant gap: there is no comprehensive synthesis quantifying IPE’s impact on attitudes in LMICs, the types of designs used, and methodological limitations that complicate interpretation. This systematic review synthesizes evidence on structured IPE interventions’ impact on collaborative attitudes among undergraduate health profession students in LMIC contexts, exploring intervention characteristics, methodological quality, and evidence gaps.
Methodology
Review Question, objectives and framework
Our primary research question aimed to explore how IPE interventions affect health-professional students’ attitudes towards collaborative practice in LMICs, and under what contextual conditions these effects occur. The main objective was to assess whether IPE led to a positive (↑), negative (↓), or neutral (↔) change in student attitudes, utilizing validated instruments to classify and code these outcomes. Secondary objectives included investigating how elements such as the context of delivery, the level of learners, and regional or cultural traits impacted these attitude shifts through narrative comparison; integrating qualitative themes to corroborate observed variations; assessing the risk of bias at the study level; summarizing the overall certainty of the evidence; and identifying evidence gaps for future research.
This systematic review used the PICO-framework to ensure a methodical approach to formulating questions, conducting literature searches, and selecting studies. The review explored: For undergraduate or pre-licensure health-profession students in LMICs, how do structured IPE interventions, compared to other interventions or none, influence attitudes toward interprofessional collaboration? The population consisted of undergraduate or pre-licensure students from at least two health professions, with studies taking place in LMICs as classified by World Bank FY-2026 income thresholds [9]. The intervention was a structured IPE activity, aligned with WHO (2010) definition and IPEC core competencies, where students learn with, from, and about each other in academic or clinical environments [1]. Comparators could be any educational activity or none, as seen in within-group pre/post designs. The outcome was quantitative change in attitudes toward interprofessional collaboration, assessed using validated instruments such as the Interdisciplinary Education Perception Scale (IEPS), Interprofessional Attitudes Scale (IPAS), Readiness for Interprofessional Learning Scale (RIPLS), Knowledge-Attitude-Practice (KAP) questionnaire, or a custom tool reporting numerical pre/post change [10–13].
The PICO-framework was enhanced by insights from the WHO Framework for Action on IPE & Collaborative Practice (2010) and the IPEC-Core Competencies for IPEC Practice (2016 update; 2023 revision), which highlight the importance of values and ethics, roles and responsibilities, interprofessional communication, and teamwork [1–3]. These global standards guided both the selection criteria and the analysis of the evidence base.
Eligibility criteria
Studies were eligible if they met these conditions: The design had to be experimental, quasi-experimental, or interrupted time-series, with pre- and post-intervention measurements of student attitudes toward interprofessional collaboration. The population comprised undergraduate or pre-licensure students in health-profession programs like medicine, nursing, pharmacy, physiotherapy, or public health, representing at least two disciplines. Studies had to be conducted in LMICs as defined by World Bank FY-2026 income thresholds [9]. The intervention was a structured IPE activity such as workshops, courses, or simulations involving interactive learning across professions; facilitating learning with, from, and about multiple health professions, delivered in academic or clinical environments. The primary outcome was quantitative change in attitudes toward interprofessional collaboration, measured using a named, described, or validated scale-such as IEPS, IPAS, RIPLS, or KAP - or a custom tool reporting numerical pre/post change [10–13]. Only studies published in English between January 2010, and July 2025 were eligible.
Research was not included if it consisted of cross-sectional surveys, single-arm opinion polls, or was entirely qualitative. Studies that concentrated exclusively on postgraduate or licensed health professionals were deemed ineligible, as were those that did not conduct both pre- and post-intervention evaluations of attitudes. Additionally, non-primary research outputs such as conference abstracts, editorials, commentaries, and opinion pieces were excluded. Studies were also not considered if they did not meet the requirement of being set in LMICs or if they did not include participants from at least two different health professions.
Design and registration
This systematic review adhered to the PRISMA (2020) guidelines for systematic reviews and meta-analyses [14]. All the items as per PRISMA checklist are mentioned in Appendix. The review protocol was planned in advance and registered with the Open Science Framework (OSF) under the registration number 10.17605/OSF.IO/63ZXD. A mixed-methods convergent integrated synthesis was utilized in the review to merge quantitative and qualitative evidence regarding IPE interventions in LMICs.
Information sources and search strategy
Databases were searched from January 2010 to August 10, 2025, including PubMed/MEDLINE, Scopus, and EMBASE. A combination of controlled vocabulary (e.g., MeSH) and free-text terms related to “IPE,” “collaborative attitudes,” and “low- and middle-income countries” was used. The full database-specific search strategies are detailed in the Appendix 1.
To supplement the database search, we explored grey literature sources such as Google Scholar, OpenGrey, and institutional repositories. We also hand-searched the reference lists of all included studies and relevant systematic reviews to identify any additional eligible articles.
Study selection process
All retrieved citations were imported into Rayyan for deduplication and screening [15]. Three reviewers (UJ, RRP, SB) independently screened all titles and abstracts for eligibility. Full texts for potentially relevant studies were then retrieved and independently assessed by both reviewers. Discrepancies were resolved through discussion, with a fourth reviewer (SK) arbitrating when necessary. The study selection process is summarized in a PRISMA flow diagram under the results section.
Data extraction
Data were extracted independently by two reviewers (UJ, RRP) using a piloted extraction form. The extracted items included study identifiers, country and World Bank income classification, participant demographics, professional mix, and prior exposure to IPE. We also collected detailed information on intervention characteristics, such as the type, framework used, duration, delivery mode, setting, group size, professions included, facilitator details, and clinical focus. Outcome-instrument properties, numeric results, and any qualitative feedback were also extracted.
Discrepancies between reviewers were resolved through discussion or, when necessary, with the arbitration of a third or fourth reviewer (SB or SK). Where articles lacked certain information (e.g., attrition rates or reliability coefficients), this was coded as “NR” (Not Reported) to ensure transparency, in line with best-practice guidelines.
We extracted the following variables: author(s), year, country, income classification, participant disciplines, sample size, study design, intervention description (duration, setting, pedagogy), outcome instrument(s), timing of measurement, main results, and funding source.
Risk-of-bias & certainty of evidence - assessment
The risk of bias for all included studies was assessed independently by two reviewers using the JBI Critical Appraisal Checklist for Quasi-Experimental Studies [16]. This tool evaluates potential bias across nine domains, including confounding, participant selection, classification of interventions, deviations from intended interventions, missing data, and reliability of outcome measurement. Disagreements between reviewers were resolved through discussion or third-party adjudication. The judgments for each study were presented item-by-item in a summary table and visually summarized using a colour-map.
Certainty of evidence for each outcome was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach, considering risk of bias, inconsistency, indirectness, imprecision, and publication bias. Summary of findings tables were generated accordingly [17].
Effect measures and data synthesis
Meta-analysis was not feasible due to heterogeneity in study designs, outcome measures, and reporting. Instead, we performed a narrative synthesis following the Synthesis Without Meta-analysis (SWiM) guideline [18]. Our approach involved grouping studies by learner level and delivery context, and coding primary attitude outcomes by effect direction (↑ for significant improvement, ↓ for significant decline, and ↔ for no change) using a p-value threshold of < 0.05. We visualized these vote-count results in a harvest plot, where the bar height was proportional to the paired-sample size. The narrative synthesis explored how delivery format, clinical exposure, and professional mix influenced the direction of effects. We also mapped evidence gaps by plotting intervention type against learner level. The findings were further grouped by geographic region, intervention type, and the specific instrument used, and we tabulated study characteristics and main outcomes, integrating qualitative descriptions where available.
Publication bias assessment
We did not formally assess publication bias due to the small number of included studies (< 10) and heterogeneity in outcomes; however, we acknowledge the possibility of selective reporting in the included literature.
Qualitative integration
Where available, open-ended responses were extracted and analyzed thematically. We used a convergent integrated mixed-methods approach, in which qualitative themes were triangulated with quantitative effect direction to identify plausible explanations for heterogeneity.
Patient and public involvement
No patients or members of the public were involved in the design, conduct, reporting, or dissemination of this review.
Results
Study selection
Our searches identified 1,904 records (PubMed = 437, Scopus = 1,138, Embase = 329). After removing 384 duplicates, 1,520 unique titles/abstracts were screened; 1,458 were excluded at this stage for reasons such as: clearly not IPE, single-discipline/uni-professional reports, wrong publication type (e.g., editorials, protocols, commentaries), or not being an empirical intervention study.
Sixty-two full texts were retrieved and assessed for eligibility; 57 were excluded for the following reasons aligned with our a-priori criteria: no pre-post or comparative measurement of attitudes (n = 16); single-discipline cohorts only (n = 9); population not eligible (postgraduate/licensed professionals only) (n = 8); outcomes not eligible (no quantitative attitudinal change reported) (n = 8); conducted outside LMIC settings (n = 7); and conference abstract/insufficient data for extraction (n = 5).
Five studies met all inclusion criteria and were included in the synthesis. These were conducted in Brazil, Iran, India, Lebanon, and Pakistan.
PRISMA flow diagram encompassing every stage of screening is presented as Fig. 1.
Fig. 1PRISMA flow diagram
Table 1 presents the characteristics of the five included studies, conducted between 2017 and 2025 in Brazil, Lebanon, India, Iran, and Pakistan, enrolling a total baseline sample of 396 participants from multiple health professions, most commonly medicine and nursing. All studies used a pre-post design without a concurrent control group. Intervention formats ranged from single-day workshops to multi-week clinical placements and a year-long postgraduate course, delivered in classroom, blended, or ward-based settings. Group sizes varied from pairs to small groups of up to nine students. Attitudes were measured using a mix of validated tools (IEPS, IPAS, RIPLS) and custom questionnaires, with four studies reporting significant positive change in overall attitudes, particularly in domains such as teamwork, role understanding, and communication; and one reporting mixed results with decline in a specific domain.
Table 1. Characteristics of included studies [19–23]Author (Year)Country/Income Level (WB)Participants & DisciplinesSample Size (N)Study DesignIntervention DescriptionDuration/FrequencyOutcome Measure(s)Follow-up PeriodMain Attitudinal OutcomeBlanco-Vieira et al. (2017) [19]Brazil/UMICMedical, Nursing111Pre-post without controlCase-based workshops on collaborative practice3 sessionsIEPSImmediate post-test↑ IEPS subscales (p < 0.05)Dabaghzadeh et al. (2017) [20] Iran/UMICPharmacy, Nursing39Pre-post without controlWard-based collaborative training rounds4 weeksRIPLSImmediate post-test↑ RIPLS teamwork subscaleRay et al. (2021) [21]India/LMICMBBS, BSc Nursing, BPT90Pre-post without controlSimulation-based IPE on patient care scenarios1 dayRIPLSImmediate post-test↑ Total RIPLS score (p < 0.05)Sakr et al. (2022) [22]Lebanon/LMICMedical, Nursing, Physiotherapy72Pre-post without controlProblem-based IPE on clinical decision-making2 weeksRIPLSImmediate post-test↑ Total RIPLS score; role understanding improvedBruce et al. (2025) [23]Pakistan/LMICMedical, Nursing, Pharmacy84Pre-post without controlCommunity health clinic-based IPE rotation2 weeksATHCTSImmediate post-test↑ Positive attitudes towards teamwork*WB *World Bank, *UMIC *Upper-middle-income country, *ATHCTS *Attitudes Toward Health Care Teams Scale
Population and context
Table 2 outlines the demographic and contextual characteristics of participants across the five included studies. Sample sizes analyzed ranged from 39 in Brazil’s postgraduate mental-health specialization to 111 in Lebanon’s semester-long IPE course, with attrition varying from 0% in the Indian and Pakistani studies to 57% in Lebanon. Female representation was high where reported, ranging from 58% in India to 85% in Brazil. Academic levels varied, with most participants being undergraduates, except in Brazil, where all were multi-professional postgraduates. Recruitment methods included voluntary participation in three studies and course-mandated enrolment in Lebanon; only Pakistan reported explicit year-wise distribution. Instruction was delivered in English in most settings, except Brazil and Iran, where Portuguese and Persian/English mixes were used. Notable contexts included rural or tribal delivery in India, a busy tertiary-care hospital in Pakistan, and the first documented large-scale IPE integration in Middle Eastern medical curricula in Lebanon.
Table 2. Population demographics & study context [16, 19–23]Study IDCountry/WB Income LevelInstitution Type/LocationEligible NRecruited N (Baseline)Analyzed NAttrition %Recruitment MethodKey DemographicsProgram MixPrior IPELanguageMotivation/Ethics/IncentiveNotable Context/Notes Blanco-Vieira et al., 2017 [19]Brazil/Upper middleFederal public university, urban (São Paulo)54543928NR85% female; mean age 34.8 y; multi-professional postgraduates (psychiatrists 39%)11 disciplines; psychiatry dominantMajority had prior clinical contact; formal IPE NRPortugueseEthics approved; written consent; no incentives360-h interprofessional mental-health specialization Dabaghzadeh et al., 2017 [20]Iran/Upper middlePublic university-affiliated teaching hospital, urban (Kerman)NRNRNRNRVoluntary (prospective cohort)Gender/age NR; final-year medical and pharmacy studentsMedicine & Pharmacy (ratio NR)NonePersian/English mixEthics approved; written consent; no incentivesInpatient infectious-disease ward Ray et al., 2021 [21]India/Lower middlePrivate teaching hospital campus, rural/tribal (Wayanad, Kerala)NR96960Not described58% female; male/female by profession given; age NRBalanced 1:1:1 (Medicine, Nursing, Physiotherapy)None statedEnglishVoluntary; ethics approved; written consent; no incentivesPostnatal care IPE in hierarchical Indian setting Sakr et al., 2022 [22]Lebanon/Upper middleResearch-intensive private university, urban (Beirut)34626011157Course-mandated enrolmentGender/age NR; medicine, nursing, MPHMedicine 54%, Nursing 25%, Public Health 22%Prior IPE NR; high baseline scoresEnglishMandatory curricular course: ethics approved; verbal consent; no incentivesFirst large IPE in Middle East medical curricula Bruce et al., 2025 [23]Pakistan/Lower middlePublic tertiary-care teaching hospital, urban (Lahore)NR86 (43 nursing, 43 medicine)860Convenience sampling76.7% female; age 18–26 y; year 2 (31%), year 3 (36%), final year (33%)Balanced 1:1 (Medicine, Nursing)NoneEnglishVoluntary; ethics approved; written consent; no incentivesCourse embedded in busy teaching hospital*MPH *Master of Public Health. “Eligible N” refers to the number of students meeting inclusion criteria prior to recruitment; “Analyzed N” reflects participants included in final analysis. Attrition % calculated as (Recruited N - Analyzed N) ÷ Recruited N × 100
Table 3 summarizes the design and delivery of the IPE interventions across the five included studies. Intervention duration ranged from single-day workshops (India, Iran) to multi-week or semester-long programmes (Pakistan, Lebanon) and a 360-hour postgraduate course (Brazil). Formats included classroom-based didactic sessions, case-based learning, simulation, ward-based clinical placements, and blended approaches. Group sizes within activities varied from small interprofessional teams of 6–8 students to larger mixed-discipline cohorts. Facilitators were drawn from multiple professions in all studies, with varying degrees of structured faculty training in IPE. All interventions targeted interprofessional competencies such as teamwork, communication, and understanding of roles, though emphasis differed by study.
Table 3IPE intervention characteristics [19–23]Study IDIntervention Name†TypeFramework/ModelDurationIntensity/ScheduleDelivery FormatSettingGroup SizeProfessions IncludedKey Learning MethodsAssessment MethodsFacilitator TypeFacilitator TrainingClinical FocusPatient/Case Type Blanco-Vieira et al., 2017 19]Child & Adolescent Mental Health Specialization Course (CESMIA)Post-graduate courseProblem-based learning model360 h totalSchedule NR (delivered across academic year)Face-to-faceUniversity classrooms & small-group roomsSmall groups (size NR) from cohort of 39Lectures, small-group PBL case discussionsSummative - KAP survey pre/postCourse tutors/facultyNRChild & adolescent mental healthPaper/discussion cases-- Dabaghzadeh et al., 2017 [20]Infectious-disease ward IPE placementClinical placementNR2 weeksDaily 4 h (08:00–12:00)Face-to-face clinicalIn-patient infectious-disease wardPairs of 2 (1 Pharm + 1 Med)Bedside care, medication review, daily roundsSummative - RIPLS pre/postID specialist ་ clinical pharmacistNRInfectious diseasesReal in-patients-- Ray et al., 2021 [21]IPE learning experience in Post-natal CareMixed (didactic + case-based + workplace)NRNR (multi-session module)2 didactic talks, 3 case-sessions, ward-based teamwork (period NR)Blended (classroom ་ ward)Classroom & postnatal ward6 students/team; 8 teams/batchMedicine, Nursing, PhysiotherapyLectures, case vignettes, small-group planning, bedside care, poster presentationRetro-prequestionnaire ་ formative posterFaculty (obstetrics, nursing, physio)NRPostnatal maternal careReal ward patients & paper vignettes Sakr et al., 2022 [22]IPE & Collaboration (IPEC) courseCase-based courseIPEC competency framework≈ 3 months (one semester)Small-group discussion once/week (exact hours NR)Face-to-faceClassroom small-group rooms9 students (4–5 Med, 2–3 Nurs, 2 MPH)Case-based collaborative learningSummative - IPAS pre/postFaculty from three schoolsYes - multiple preparatory workshopsPublic-health topics (smoking cessation, HIV, cardiac care, etc.)Hypothetical paper cases-- Bruce et al., 2025 [23]“Structured IPE module” (title NR)Mixed (case-based + simulation)NR4 weeksWeekly sessions, hours NRFace-to-faceClassroom sessions ་ simulation lab6–8 studentsMedicine & Nursing under-graduates (1:1)Scenario-based case discussions, team simulations, guided reflectionSummative - IEPS pre/post surveyFaculty (medicine & nursing)NRGeneral teamwork & patient-centered careSimulated scenariosMissing items are coded “NR”; no study stated an explicit social-psychological theory (e.g., Contact or Social-Identity) beyond the IPEC competency framework in Sakr et al., 2022. The Lebanese IPEC course is the only programme that explicitly documented structured faculty workshops before delivery, fulfilling best-practice recommendations for facilitator preparation
Risk of bias
All five included studies were appraised using the JBI Critical Appraisal Checklist for Quasi-Experimental Studies, as each employed a non-randomized, pre-post design without a concurrent control group [16]. Table 4 presents the item-by-item judgments alongside brief justifications and an overall verdict for each study, while Fig. 2 displays the same data as a colour-coded map. Across studies, risk was most often introduced by the absence of a control arm (JBI Item 4), unclear reporting on baseline group comparability (Item 2) and incomplete follow-up or limited handling of attrition (Item 6). Measurement reliability was generally acceptable, with three studies using validated attitude scales (IEPS, IPAS, RIPLS) and two relying on tools with limited or no prior validation [10–12]. Appropriate statistical analyses for within-group comparisons were reported in all cases. Based on these criteria, three studies were judged at moderate risk of bias, while two (Ray 2021; Sakr 2022) were judged at serious risk, mainly due to retrospective-predesign or substantial attrition [21, 22].
Table 4. Risk of bias summary table with justification and verdict [16, 19–23]Study IDJBI1: Cause→Effect clear?JBI2: Groups similar?JBI3: Similar care aside from intervention?JBI4: Control group present?JBI5: Multiple pre/post measures?JBI6: Follow‑up complete/handled?JBI7: Same measurement across groups?JBI8: Outcomes measured reliably?JBI9: Appropriate statistics?Justification (summary)Final verdictBlanco-Vieira et al. (2017) [19]YesN/AN/ANoYesYesYesNo/UnclearYesUncontrolled pre/post; partial follow-up; non-validated KAP tool elevates measurement bias; stats appropriate.Moderate riskDabaghzadeh et al. (2017) [20]YesUnclearYesNoYesYesYesYesYesProspective cohort; no control; validated RIPLS; high completion; appropriate non-parametric analysis.Moderate riskRay et al. (2021) [21]YesUnclearYesNoNoUnclearYesYesYesRetro‑pre (no true baseline); no control; handling of missing data unclear; stats align with within-subject design.Serious riskSakr et al. (2022) [22]YesUnclearYesNoYesNoYesYesYesPre/post with substantial attrition; no control; validated IPAS; appropriate paired analysis.Serious riskBruce et al. (2025) [23]YesN/AN/ANoYesUnclearYesYesYesUncontrolled pre/post; attrition handling unclear; validated IEPS with appropriate paired tests.Moderate risk
Fig. 2. Risk of Bias (JBI) map [16, 19–23]. Colour-map of JBI Critical Appraisal Checklist ratings for the five included studies, where green = “Yes/low risk”, yellow =“Unclear/No-unclear”, and red/purple = “No/high risk”; White denotes items not applicable
Quantitative synthesis (SWiM vote-count approach)[18]
Table 5 details the attitudinal outcome measures used and their key properties. Three studies employed validated instruments-the IEPS, IPAS, or RIPLS-while two used custom or adapted questionnaires with partial or no validation evidence [10–12]. All tools generated numerical pre- and post-intervention scores, allowing calculation of change over time. The number of items per scale ranged from 9 to 35, with response formats typically on 5- or 6-point Likert scales [24]. Domains covered included teamwork, communication, perceptions of professional roles, and readiness for interprofessional learning. Timing of post-intervention measurement was immediate in all studies.Table 5. Outcome measurements and instruments [19–23]Study IDPrimary instrument (full name)CodeTotal itemsSub-scales/domains assessedResponse scale & score rangeOriginal validation contextLocal validation reported?Language of administrationReliability (α) reportedMeasurement scheduleSecondary outcomes Blanco-Vieira et al., 2017] [19]Knowledge-Attitude-Practice questionnaire (self-developed)KAPNR (18 attitude items within larger tool)Knowledge; Attitudes; Practice domains (item-level details NR)NR (Likert type stated, anchors NR)Not previously validated (new tool)NoPortuguese (assumed; not specified)NRPre-course and post-course (end of 360-h programme)Knowledge & Practice sub-scores Dabaghzadeh et al., 2017 [20]Readiness for Interprofessional Learning ScaleRIPLS19Teamwork & Collaboration; Professional Identity (positive & negative); Roles & Responsibilities5-pt Likert (1 = Strongly Disagree → 5 = Strongly Agree); score range NRWidely used with under- & post-graduate health students internationallyPersian version previously validated; current study did not re-validate (No)PersianCronbach’s α NR (instrument validity noted)Pre-workshop and immediate post-workshop (same day)None Ray et al., 2021 [21]Custom retro-pre-IPE attitude questionnaireRetro-Pre35Comfort questioning peers; Reliability & Trust (plus other attitude facets - item list NR)NR (Likert type implied but not specified)Developed with University of Houston IPE facultyUnclearEnglish (online survey)NRSingle administration post-course capturing retrospective “pre” & “post” ratings (retrospective-predesign)Open-ended qualitative feedback Sakr et al., 2022 [22]Interprofessional Attitudes ScaleIPAS27Team Roles & Responsibilities; Patient–Centeredness; Interprofessional Biases; Diversity & Ethics; Community-Centeredness7-pt Likert (1 = Strongly Disagree → 7 = Strongly Agree); one item reverse-scored; total-score range NR Norris et al., 2015, USA students (cited)NoEnglish (instruction language)NR (tool described as “validated”)Baseline first course session & 3 months later at course completionNone Bruce et al., 2025 [23]IPE Perception ScaleIEPSNRCompetency & Autonomy; Perceived Need for Co-operation; Perception of Actual Co-operation5-pt Likert (1 = Strongly Disagree → 5 = Strongly Agree); total-score range NRDeveloped for USA health-professions students (cited in text)NoEnglish (paper, supervised)“Strong internal reliability” - exact α NRPre-module (week 0) & immediate post-module (week 4)None
We coded the direction of change (↑ improvement, ↓ worsening, ↔ no change) for each primary attitude outcome, following SWiM guidance and presented findings in a harvest plot. Effect-direction coding revealed that four of the five included LMIC studies reported statistically significant positive shifts in IPE attitudes (↑, p ≤ 0.001). These studies were Bruce 2025 (IEPS), Ray 2021 (retro-pre survey), the medical subscales of Dabaghzadeh 2017 (RIPLS), and Blanco-Vieira 2017 (KAP). In contrast, Sakr 2022 showed a small but significant decline in the IPAS patient-centeredness domain (↓, p = 0.003), an effect that coincided with the highest attrition rate (68%), suggesting potential response bias. It is noteworthy that while the medical subscales in Dabaghzadeh 2017 were positive, the overall attitude score for the study remained neutral (↔). This study also highlighted context-sensitive outcomes, as clinical placements in Iran produced profession-specific effects: a positive shift for medical students (↑) versus no change for pharmacy students (↔). (Fig. 3)
Fig. 3- Harvest plot illustrating effect direction (↑ improvement, ↓ worsening, → no clear change) and paired-sample size for each study
Qualitative synthesis
Table 6 summarizes qualitative data from open-ended survey questions or focus group discussions conducted in four of the five included studies. The most frequently reported themes were improved teamwork, better understanding of other professional roles, and enhanced communication. Other themes included increased confidence in collaborative settings, greater appreciation of shared decision-making, and recognition of mutual respect among professions. In two studies, participants highlighted the practical relevance of IPE to clinical practice. A minority of comments reflected logistical challenges or perceptions of unequal participation among disciplines.
Table 6. Qualitative feedback & thematic findings [19–23]Study IDQualitative methods usedQualitative sample (n)Positive feedback themesChallenges/barriers reportedLearning outcomes describedBehavior/professional-identity impactImplementation acceptability & suggestionsFaculty observations Blanco-Vieira et al., 2017 [19]None (KAP survey; narrative reflection in discussion)39 completed both KAP surveysParticipants valued small-group case discussion supervised by child-mental-health tutors to “build a joint solution”No validated tool; small sample; absence of follow-up; convenience samplingReported 17% attitude gain, 14% practice gain reinforcing relevance of inter-professional coursesOlder, more experienced professionals gained most knowledge (identity reinforcement)Participants felt course length (360 h) and multiple interactive methods were important for changeNR Dabaghzadeh et al., 2017 [20]None (prospective cohort with RIPLS; qualitative remarks in discussion)NRStudents reported increased knowledge and eagerness for more IPE coursesExtracurricular timing, busy clinical schedules, time-consuming two-week rotationImproved teamwork & communication (author interpretation)NRRecommend embedding IPE in curricula and providing suitable environmentNR Ray et al., 2021 [21]Open-ended questions analyzed thematically96 students; 96 responses, 40-31−25 citing top themesTeamwork (42%), Communication (32%) & Knowledge of other roles (26%) with illustrative quotes such as “The greatest thing was working together … in a clinical scenario”None noted by students; authors discuss cultural hierarchies as potential barrierEnhanced respect, clarity on roles, confidence in inter-disciplinary dialogueStudents reported “now I fully comprehend what their roles are” indicating shift in professional identitySmall-group discussion and real ward work were rated “most important” parts of experienceFacilitators observed that questioning across professions-built trust Sakr et al., 2022 [22]None (pre/post IPAS survey only)NRNR (study focused on attitude scores)Resource-intensive course; 40 faculty/year, curricular change across three faculties, heterogeneity of student experienceNRNRAuthors highlight need for protected time and faculty development to sustain courseNR Bruce et al., 2025 [23]None reported (quantitative survey only; no open-ended items)NRStudents’ discussion section notes “significant gains in perceived cooperation, shared decision-making and understanding of roles”Single-site setting, no long-term follow-up, limited generalizabilityBetter appreciation of teamwork and mutual respectFinal-year students showed highest post-scores, suggesting stronger professional identity integrationNR (course judged effective but no student suggestions captured)NR
Mixed-methods integration and heterogeneity
Aligning quantitative vote-count data with qualitative themes suggests that interventions emphasizing small-group dialogue and real clinical exposure (Pakistan, India, Iran) were more likely to produce positive attitude shifts, whereas resource-intensive, semester-long courses with high attrition (Lebanon) risk dilution of impact. Professional hierarchy and lack of protected time emerged as plausible explanations for heterogeneity.
Evidence gap map
Plotting of Intervention type against learner level was as seen in Fig. 4. Empty cells underscore missing evidence for simulation-based IPE and long-term (> 6 month) follow-up in LMIC contexts.
Fig. 4. Evidence gap map of IPE interventions by learner level. Numeric values within cells indicate the strength of available evidence (1 = low, 2 = moderate, 3 = high). Empty cells represent areas with no identified studies. Notably, no studies evaluated simulation-based IPE at postgraduate or mixed learner levels, and no included study assessed outcomes beyond six months post-intervention
Certainty of evidence
Using the GRADE adaptations for narrative synthesis, overall certainty was low due to risk of bias (uncontrolled designs), imprecision (small samples) and inconsistency (one study showing decline) [17]. Nevertheless, direction-of-effect consistency in four studies allowed moderate confidence that brief, well-facilitated IPE can improve professional attitudes in LMIC undergraduate settings. (Table 7)
Table 7GRADE summary of Findings - Attitudes toward IPEC after IPE among LMIC Health‑Professions students [17]Outcome (construct)No. of studies (design)Population & settingComparatorFindings (direction & consistency)Certainty of evidence (GRADE)Reasons for rating (domain‑wise justification)Overall attitude toward interprofessional collaboration after IPE (primary)5 studies (all non‑randomized pre-post; 3 with validated tools: IEPS/IPAS/RIPLS; 2 with bespoke/KAP tools)Undergraduate and postgraduate learners in Pakistan, Lebanon, India, Iran, Brazil; classrooms, blended, and clinical placementsWithin‑group pre vs. post4 of 5 studies showed significant improvement (↑); 1 study reported a small decline limited to an IPAS subdomain (patient‑centredness). Direction of effect coherent across contexts; largest attrition occurred in the study with the decline.LowRisk of bias - serious (downgrade 1 level): all are uncontrolled pre-post; 1 retrospective‑pre; one with substantial attrition. Inconsistency - not serious: 4↑ vs. 1↓ (limited to a single subdomain) with a plausible explanation (attrition/response bias). Indirectness - not serious: LMIC students; IPE interventions match review question; three validated attitude scales used. Imprecision - not serious: total analyzed N ≈ 383; although effect sizes/SDs often missing, direction is consistent and sample adequate for vote‑count SWiM. Publication bias - suspected but not rated: small studies and positive direction could suggest bias, but evidence insufficient to downgrade further.Patient‑centredness subdomain of attitudes (sensitivity outcome)1 study (IPAS domain analysis)Undergraduate students in a semester‑long IPE course (Lebanon)Within‑group pre vs. postSmall but statistically significant decline (↓) confined to patient‑centredness; other IPAS domains not consistently decreased.Very lowRisk of bias - serious: high attrition and no control; domain‑specific post‑hoc focus. Inconsistency - very serious: effect seen in a single study/domain without replication. Indirectness - not serious. Imprecision - serious: single study with attrition and no precision estimates for domain effect. Publication bias - suspected. (Multiple downgrades yield very low.)Starting level set per GRADE for non‑randomized pre-post designs (observational), i.e., Low; downgrades and additional downgrades applied by domain using narrative‑synthesis guidance. No upgrading was applied because large, precise, and consistent magnitude effects or dose‑response patterns were not demonstrated across studies
Discussion
IPE in LMICs remains inconsistently implemented despite long-standing global calls for collaborative practice [1–3]. This review synthesized evidence from five quasi-experimental studies in India, Pakistan, Brazil, Iran, and Lebanon, all reporting positive or neutral shifts in student attitudes toward collaboration [19–23]. These findings support the WHO’s Framework for Action on IPE & Collaborative Practice and align with the IPEC’s core competency updates, which emphasize values/ethics, roles and responsibilities, interprofessional communication, and teamwork [1–3].
The greatest attitudinal gains occurred when IPE was embedded in authentic clinical contexts and included diverse professional groupings. Ray et al. (2021) in rural India and Bruce et al. (2025) in Pakistan demonstrated significant improvements across all measured domains when interventions centered on ward-based care or realistic case simulations [21, 23]. Blanco-Vieira et al. (2017) reported the largest relative improvement (+ 17% in attitudes) following a prolonged, 360-hour course for mental-health professionals, suggesting that both intervention intensity and sustained interaction enhance outcomes [19]. Conversely, Sakr et al. (2022) found only patient-centredness improved, likely due to high baseline scores and a ceiling effect commonly reported in IPE evaluations [7, 22].
Risk-of-bias was generally moderate to serious: all studies used uncontrolled pre/post designs, relied on self-report instruments (e.g., RIPLS, IEPS, IPAS), and two had notable attrition (e.g., 57% unmatched pairs in Sakr et al., 2022) [10–12, 16, 22]. Certainty of evidence was downgraded for risk of bias, imprecision, and inconsistency. Nevertheless, qualitative data from India and Brazil reinforced quantitative gains, with participants citing improved trust, role clarity, and communication-consistent with recent systematic reviews identifying these as core intermediate outcomes of IPE [5, 9]. These findings can inform curriculum design in LMICs by advocating for low-cost, clinically embedded IPE programs that leverage existing resources to foster collaborative attitudes early in training, with policy implications for national health education bodies to prioritize IPE integration for improved team-based care.
Profession-specific responsiveness emerged as a key nuance. Dabaghzadeh et al. (2017) found significant improvement among medical but not pharmacy students after a shared inpatient rotation [20]. Possible explanations include entrenched role perceptions, uneven clinical responsibilities, or smaller pharmacy sample sizes. Literature reports similar profession-specific variations, which underscore the need for tailored role-clarification and feedback strategies [3, 7].
Implementation lessons for LMICs are clear. Curriculum-aligned, low-cost approaches-such as structured case discussions, ward-based team care, and small-group simulations-proved feasible and acceptable in hierarchical, resource-constrained environments [21, 23]. These approaches reflect WHO’s recommendation for context-fit, scalable IPE and align with IPEC’s 2023 emphasis on adaptable core competencies [1, 3].
Looking forward, LMIC-IPE research should progress beyond immediate post-intervention attitudes to assess sustained behavioral change and patient-level outcomes. Cochrane reviews and recent meta-analyses demonstrate such downstream effects are possible, but robust controlled designs, harmonized outcome measures, and longitudinal follow-up are essential to determine both effectiveness and cost-effectiveness in resource-constrained health systems [7, 8].
Limitations
Evidence being generated from LMIC in IPE is not much. Besides the limited number of studies making it to the final review, synthesis is constrained by the methodological quality of the included studies as well. All used uncontrolled pre/post designs, limiting causal inference and leaving findings vulnerable to confounding from concurrent curricular experiences. Reliance on self-reported attitudinal instruments introduces social desirability bias, particularly in mandatory or graded courses.
Sample sizes were modest (39–111 participants per study), and attrition was substantial in some cases (e.g., 57% unmatched pairs in one study), reducing precision and increasing risk of attrition bias. The heterogeneity of participant profiles, intervention intensity, and measurement tools precluded meta-analysis and limited comparability. Differences in cultural norms, health-system structures, and academic calendars across the five LMIC contexts further constrain generalizability.
No study included long-term follow-up, leaving the sustainability of observed attitudinal gains unknown. Finally, publication bias cannot be ruled out, as small-scale LMIC-IPE projects with null results are less likely to be reported. Addressing these limitations will require multicenter, controlled trials using harmonized tools, robust handling of missing data, and mixed-methods approaches to capture context-specific facilitators and barriers.
Recommendations and future directions
This review demonstrates that IPE in LMIC contexts can positively influence learners’ attitudes toward collaboration. The most significant gains were observed in interventions that were contextually relevant, clinically embedded, and inclusive of multiple professional groups, particularly when activities mirrored real-world patient care. These findings suggest that IPE has the potential to foster teamwork and bridge professional silos within resource-constrained, hierarchically structured health systems.
The current body of evidence is limited by several factors, including small sample sizes, methodological heterogeneity, and the frequent absence of control groups. Furthermore, the reliance on self-report measures and short-term follow-up periods reduces the certainty of observed effects, making it difficult to confirm long-term behavioral changes or patient-level benefits.
Lessons from LMIC contexts, such as scalable low-cost models, are applicable to HICs facing resource variability. International collaborations, like the International Interprofessional Collaborative Office Rounds (iiCOR) program connecting professionals across Global North and South via distance technology, could provide further insights for cross-contextual IPE implementation [25].
Supplementary Information
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1IPE Collaborative. IPEC Core Competencies for Interprofessional Collaborative Practice, Version 3. (2023). Washington, DC: IPE Collaborative; 2023. URL (PDF): https://ipec.memberclicks.net/assets/core-competencies/IPEC_Core_Competencies_Version_3_2023.pdf
- 2Reeves S, Perrier L, Goldman J, et al. IPE: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Reviews. 2013;CD 002213. 10.1002/14651858.CD 002213.pub 3.10.1002/14651858.CD 002213.pub 3PMC 651323923543515 · doi ↗ · pubmed ↗
- 3World Bank Group. World bank country and lending groups: FY 2026 income thresholds (effective July 1, 2025). World bank group ; 2025. URL: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519%E 2%80%91world%E 2%80%91bank%E 2%80%91country%E 2%80%91and%E 2%80%91lending%E 2%80%91groups.
- 4Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;n 160. 10.1136/bmj.n 160.10.1136/bmj.n 160PMC 800592533781993 · doi ↗ · pubmed ↗
- 5Campbell M, Mc Kenzie JE, Sowden A et al. Synthesis Without Meta-analysis (S Wi M) in systematic reviews: reporting guideline. BMJ 2020;368:l 6890-None. 10.1136/bmj.l 689010.1136/bmj.l 6890 PMC 719026631948937 · doi ↗ · pubmed ↗