Streptococcus dysgalactiae subsp. equisimilis bacteremia in Finland: changes in emm-type distribution combined with clinical presentation
Viivi Nevanlinna, Janne Aittoniemi, Reetta Huttunen, Hanne-Leena Hyyryläinen, Tapio Seiskari, Tiina Luukkaala, Sari Rantala

TL;DR
This study examines changes in emm-type distribution of Streptococcus dysgalactiae subsp. equisimilis (SDSE) bacteremia in Finland and its clinical implications over two decades.
Contribution
The study identifies a newly emerged emm type, stG62647, and links specific emm types to clinical outcomes and mortality.
Findings
The emm types stG480, stG485, and stG6 remained the most common, with stG62647 emerging as the third most common emm type.
Emm type StC74a was associated with higher mortality rates, while stG480 was linked to arthritis.
The overall incidence of SDSE bacteremia increased due to both rising common emm types and the emergence of stG62647.
Abstract
The incidence of SDSE bacteremia has risen dramatically over the past two decades, but it is unclear whether this increase is influenced by changes in the emm types of SDSE isolates. Furthermore, the relationships between emm types and clinical manifestations or disease severity are poorly understood. We conducted a retrospective, population-based study of emm types in SDSE bacteremia episodes in the Pirkanmaa health district from August 2015 to June 2018 and compared the findings to data from the same geographic area collected between 1995 and 2004. During the study period, 230 episodes of SDSE bacteremia were identified. The most common emm types were stG480, stG485, and stG6, consistent with findings from the same geographic area 20 years ago. The most notable change in emm type distribution was the emergence of stG62647 as the third most common emm type, along with stG6. Despite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
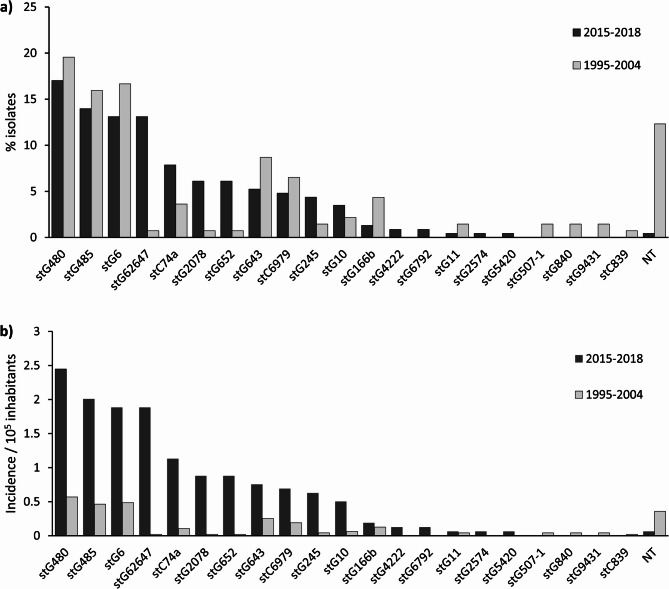 Figure 1
Figure 1- —Tampere University (including Tampere University Hospital)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Neonatal and Maternal Infections · Bacterial Identification and Susceptibility Testing
Introduction
Streptococcus dysgalactiae subspecies equisimilis(SDSE) is a beta-hemolytic streptococcus that primarily expresses Lancefield carbohydrate antigens C and G [1]. SDSE is part of the human commensal flora and was once considered to be of low pathogenicity [2]. However, more recent studies have shown that it causes a range of infections similar to those of Streptococcus pyogenes, including severe invasive infections such as cellulitis, pneumonia, deep abscesses, arthritis, endocarditis, and necrotizing fasciitis [3].
The incidence of SDSE bacteremia has significantly increased over the past few decades, even surpassing that of S. pyogenes in some countries [4–7]. This rise has been particularly notable in Finland, where the incidence of Group C and G bacteremia reached 17.6/100,000 inhabitants in 2019 [8]. A similar trend was observed in the Pirkanmaa Health District (HD), with the incidence of SDSE bacteremia rising from 2.05/100,000 in 1995 to 16.9/100,000 inhabitants in the current study population in 2015–2018 [9, 10].
In a genome sequence homology analysis, SDSE has been closely related to S. pyogenes, sharing 72% genetic similarity, presumably due to a common ancestor, but also horizontal gene transfer [11, 12]. S. pyogenes and SDSE share many major virulence factors, including the M-protein, which is essential for resisting phagocytosis, disrupting the complement system and promoting adherence to human cells [13]. As in S. pyogenes, the N-terminal region of the emm gene, encoding the M-protein, is also used for molecular typing in SDSE.
In Finland, the most common emm types in 1994–2004 were stG480, stG6, and stG485, which have also been among the most common isolates in Norway and Sweden [14–16]. However, in the past two decades, new regional upsurges in certain emm types have been reported. In several European countries, including Norway, Denmark, Spain, and Germany, as well as in Canada, the lineage stG62647 has become the major emm type, whereas in Japan, stG6792 became predominant in the 2000 s [5, 17–21]. The emm type stG62647 has been associated with severe clinical manifestations and higher case fatality rates in Norway [17]. Similarly, stG6792 has been associated with poor outcomes in Japan [22]. While specific emm types in S. pyogenes have been associated with certain clinical manifestations, similar studies on SDSE bacteremia are still lacking. In one previous study of SDSE bacteremia, no association was found between emm type and the source of infection [23].
In this study, we provide an updated distribution of emm types in SDSE bacteremia, combined with clinical data, in the Pirkanmaa Health District, Finland. Our objective was to compare these findings with previously reported data from the same health district covering the years 1995–2004 [9, 14]. We aimed to investigate whether the changes in emm type-distribution contribute to the substantial increase in the incidence of SDSE bacteremia. Moreover, we present, to our knowledge, the first comprehensive study evaluating the associations between emm types and disease severity, as well as emm types and clinical manifestations.
Methods
The Pirkanmaa Health District is the second-largest health district in Finland, with a catchment area of approximately 535 000 inhabitants. It includes Tampere University Hospital, four regional hospitals, and various smaller healthcare units. This population-based study was focused on all adult patients (≥ 18 years old) with blood culture positive SDSE bacteremia within Pirkanmaa HD from August 2015 to July 2018. All positive blood cultures were recorded in the Finnish Register for Hospital Infections and Antimicrobial Use (SAI) and were identified retrospectively. Throughout the study period, 230 episodes involving ≥ 1 positive blood cultures for SDSE were identified, with all patients also exhibiting clinical signs compatible with infection. Of these episodes, emm typing was conducted on 229 SDSE isolates, and medical records were available for 217 episodes (211 patients). The medical records were reviewed, and structured case report forms (SRs) were completed. The study was approved by the Regional Ethics Committee of Tampere University Hospital.
All blood samples taken at Pirkanmaa HD were studied at Fimlab laboratories, Tampere. During August 2015–October 2017, blood-culture samples were collected into BacT/Alert FA Plus aerobic and FN Plus anaerobic blood-culture bottles and incubated in an automated BacT/Alert 3D microbial detection system (bioMérieux). During November 2017– July 2018, blood-culture samples were collected in BD BACTEC Plus Aerobic/F and Lytic/10 Anaerobic/F culture vials and incubated in a BD BACTEC FX blood-culture system (Becton Dickinson).
SDSE was primarily identified on the basis of typical large-colony-forming growth and β-hemolysis on blood agar plates. Until February 2017, identification of the bacteria was based on latex agglutination (Lancefield grouping, PathoDxtraTM Strep Grouping Kit, Thermo Scientific, Basingstoke, Hants, UK), with confirmation (API^®^ 20 STREP [bioMérieux, Marcy l’Etoile, France] or matrix-assisted laser-desorption/ionization time-of-flight mass spectrometry, i.e., MALDI-TOF MS [VITEK^®^ MS, bioMérieux, Marcy l’Etoile, France]). Since March 2017, MALDI-TOF MS has been the primary method for identification. MALDI-TOF analysis provides results for S. dysgalactiae subsp. dysgalactiae/equisimilis, which was interpreted as S. dysgalactiae subsp. equisimilis associated with human disease. Antimicrobial susceptibility testing was based on the disk diffusion method, according to The European Committee on Antimicrobial Susceptibility Testing (EUCAST) standard [24]. The SDSE strains were stored in skimmed-milk broth at −70 °C until further emm type analysis. Emm typing was conducted according to the guidelines of the Centers for Disease Control and Prevention [25].
Epidemiology, patient characteristics, and clinical manifestations of the study population have been described in detail elsewhere [10, 26]. To compare the distribution of emm types, we utilized previously published data from the same health district, covering the years 1995–2004 [9, 14]. Statistical analyses were performed by using IBM SPSS Statistics for Mac, Version 29 (IBM corp., Armonk, NY, US). The associations between emm types and sex, clinical manifestations and markers of severe disease were tested using the χ2 test or Fisher’s exact test, as appropriate. The associations between emm types and age was studied using the Mann–Whitney U test. P-values under 0.05 were considered statistically significant. Mantel–Haenszel Common Odds Ratio estimates were calculated, and odds ratios are expressed with 95% confidence intervals.
Results
Over the three-year study period, 230 episodes of SDSE bacteremia were detected, with 229 episodes available for emm typing. Medical records were available concerning 217 episodes, involving 211 patients. Altogether, 17 emm types were identified, and a total of 29 subtypes. Four new subtypes were discovered: stG2078.18, stG4222.5, stG6.34, and stG6.35. One isolate remained non-typeable.
The distribution of emm types, compared with findings reported previously from the same health district during 1995–2004, is presented in Fig. 1. The six most prevalent emm types identified in the current study were stG480 (39 isolates), stG485 (32 isolates), stG62647 (30 isolates), stG6 (30 isolates), stC74a (18 isolates), and stG2078 (14 isolates), covering 71% of all isolates. Notably, stG480, stG485 and stG6 have remained the three most common emm types in the same region over the past 20 years. However, in the present study, stG62647 emerged as the third most common emm type, along with stG6, accounting for 13% of the isolates, compared with only one isolate detected over the ten-year period 20 years ago. StG643, stC6979 and stG2078 now constitute smaller proportions compared with the previous data. Conversely, the proportions of stC74a, stG166b, and stG652 have increased. Compared with the previous study, four new types have appeared: stG4222, stG6792, stG2574 and stG5420, and four types have disappeared: stG507-1, stG840, stG9431 and stC839.
Despite changes in distribution, the incidence rates of isolates of all emm types identified in this study have significantly increased compared with 20 years ago (Fig. 1b). The incidence of stG62647 isolates has risen dramatically. However, the incidences of the three most common emm types in the previous study—stG480, stG485, and stG6— have also all increased, approximately fourfold.Fig. 1a Distribution of 229 emm types of Streptococcus dysgalactiae subsp. equismilis isolates from August 2015 to June 2018, compared with previously published data from the same health district in 1995–2004, Finland. StG480, stG485, and stG6 have remained the three most common emm types over the past 20 years, but stG62647 has emerged to share third place with stG6. b Mean annual incidence of emm types of Streptococcus dysgalactiae subsp. equismilis isolates from August 2015 to June 2018, compared with a previously published study from the same health district in 1995–2004, Finland. The incidence of all major emm types identified in the present study has significantly increased compared to that of 20 years ago. NT, nontypeable
The median age of the patients, in the 217 episodes where medical records were available, was 75 years (range 28 to 95 years), and 60% of the patients were male. The most common clinical manifestations are presented in relation to emm types in Table 1. Of all patients, 72% presented with skin and soft-tissue infections (SSTIs). Compared with other emm types, bacteremia caused by stG485 more often had an unknown infection focus (p = 0.010, OR 3.395 [95% CI 1.375–8.382]), and SSTIs were less common (p = 0.046, OR 0.455 [95% CI 0.207–1.000]). Arthritis was more frequently observed in patients with emm type stG480 (p = 0.033, OR 5.147 [95% CI 1.227–21.589]). Age or sex were not associated with specific emm types.Table 1. The most common clinical manifestations and outcome of Streptococcus dysgalactiae subsp. equisimilis from August 2015 to July 2018, FinlandSite of infection^a^stG480N = 38stG485N = 31stG6N = 29stG62647N = 28stC74aN = 18AllN = 217n(%)p-valueOR(95% CI)n(%)p-valueOR(95% CI)n(%)p-valueOR(95% CI)n(%)p-valueOR(95% CI)n(%)p-valueOR(95% CI)n(%)Skin/soft tissue infections29(76)0.5931.249(0.552–2.824)18(58)0.0460.455(0.207–1.000.207.000)23(79)0.3981.505(0.580–3.903)19(68)0.5280.759(0.322–1.788)13(72)1.0000.968(0.330–2.845)158(72)Cellulitis27(71)0.7271.147(0.532–2.473)17(55)0.0730.497(0.229–1.078)22(76)0.3691.510(0.611–3.727)17(61)0.3310.667(0.294–1.515)10(56)0.2110.540(0.203–1.434)149(69)Purulent skin infection7(18)0.8120.897(0.365–2.202)4(13)0.2970.558(0.184–1.691)9(31)0.1032.038(0.854–4.865)3(11)0.1950.447(0.128–1.556)5(28)0.3631.630(0.548–4.848)43(20)Pneumonia7(18)0.6721.218(0.488–3.037)5(16)1.0001.000(0.356–2.812)6(21)0.4291.430(0.536–3.818)4(14)1.0000.849(0.275–2.620)4(22)0.5021.548(0.478–5.016)35(16)Deep abscess3(8)0.7051.449(0.379–5.535)00.2233(10)0.3902.054(0.530–7.956)3(11)0.2262.148(0.553–8.339)1(6)1.0000.917(0.112–7.482)13(6)Bone and joint infection4(11)0.0763.392(0.908–12.667)3(10)0.1572.740(0.669–11.221)1(3)1.0000.710(0.087–5.824)00.3671(6)0.5871.242(0.148–10.395)10(5)Arthritis4(11)0.0335.147(1.227–21.589)2(7)0.3202.069(0.398–10.748)1(3)1.0000.923(0.109–7.792)00.6001(6)0.5061.613(0.187–13.895)8(4)Bacteremia without defined focus2(5)0.1060.313(0.071–1.376)9(29)0.0103.395(1.375–8.382)3(10)0.7740.719(0.203–2.547)5(18)0.5491.495(0.519–4.304)1(6)0.4790.359(0.046–2.807)29(13)Fatal outcome3(8)1.0001.010(0.276–3.704)1(3)0.4780.354(0.045–2.771)2(7)1.0000.854(0.185–3.946)3(11)0.4661.5000(0.403–5.590)4(22)0.0404.088(1.177–14.202)17(7)^a^One patient may have one or more clinical manifestations
The emm types accounting for less common clinical manifestations are presented in Table 2. There was notable variation among the emm types responsible for these manifestations, with nine out of all 16 detected emm types also identified in less common manifestations. The four most common emm types (stG480, stG485, stG6 and stG62647) were also the most common types in rarer clinical manifestations, collectively accounting for 65% of these episodes, whereas in more common clinical manifestations, the top four emm types accounted for 60% of the episodes (p = 0.869).
Table 2. Distribution of emm types among isolates causing rare clinical manifestations of Streptococcus dysglactiae subsp. equisimilis bacteremia from August 2015 to July 2018, FinlandSite of infection^a^emm typeNecrotizing fasciitis1 stG652Osteomyelitis2 stG4801 stG485Spondylitis1 stG4801 stG485Periprosthetic joint infection1 stG4801 stG4851 stG61 stG2078Empyema1 stG4801 stG6Endocarditis1 stC74a1 stG6431 NTAortitis1 stC74aForeign body infection1 stG4801 stG62647Puerperal sepsis1 stG4801 stG61 stG20781 stG6792Intra-abdominal infection1 stG4801 stG4851 stG62647Endophthalmitis1 stG643^a^One patient may have one or more clinical manifestations
Seventeen patients (8%) died within 30 days of a positive blood culture. As shown in Table 1, the highest case fatality rate was observed in episodes caused by stC74a (22%), which was statistically significantly higher compared with other emm types (p = 0.040, OR 4.088 [95% CI 1.177–14.202]). Regarding disease severity (admission to an ICU or death within 30 days), no statistically significant differences were observed among the emm types. Emm types were also studied in relation to various characteristics of severe disease, which included a lowered level of consciousness (or unconsciousness), hypotension, septic shock, disseminated intravascular coagulation, multiorgan failure, and the need for surgical intervention, but no statistically significant differences were observed. Emm type StG62647 appeared to be associated with septic shock, though this result did not reach statistical significance (p = 0.051). When comparing the eight most common emm types (each accounting for over 5% of the isolates) with the rarer emm types, no statistically significant differences were found in terms of case fatality rate (9% vs. 3%, p = 0.317) or disease severity (12% vs. 3%, p = 0.136). Similar results were found in comparison of the top four emm types (each accounting for over 10% of the isolates) vs. others.
All emm types were susceptible to penicillin and cephalosporins. Clindamycin resistance was observed in 2% of strains, and one strain (0.4%) was intermediately sensitive. All strains resistant to clindamycin were also resistant to erythromycin. The rate of erythromycin resistance was 10%, and 2% were intermediately sensitive. The highest rates of resistance to both clindamycin and erythromycin were found in connection with stG480 (n = 38, 16% each) and stG245 (n = 8, 13% and 25% respectively). Among the ten most common emm types, clindamycin resistance was observed in stG485 (n = 31, 3%) and stG652 (n = 12, 8%). Erythromycin resistance was present in all ten most common emm types, but not in stG62647 (n = 28), stG10 (n = 8), and stG166b (n = 3). Notably, there was no significant resistance in the emerging emm type stG62647; one strain was intermediately sensitive to erythromycin and all strains were susceptible to clindamycin.
Discussion
In this population-based study, the three most common emm types remained stG480, stG485 and stG6, consistent with findings from the same geographic region 20 years ago. StG485 and stG6 are prevalent in several countries globally [15, 22, 23, 27–29]. StG480 is frequent in Norway, Sweden and Austria, as in Finland, but is rarer in other countries [15, 16, 27]. In the USA, stG6 has been the most common emm type, and stG485 and stG480 ranked among the top eight [30]. Interestingly, none of these three emm types were among the most common in Canada [21].
The most notable change in emm-type distribution in our study was the emergence of emm type stG62647, which is now, along with stG6, the third most common type. This trend has been observed in several other countries. In Norway, stG62647 was rare prior to 2013, but between 2013 and 2015, it became the most common emm type, representing 20% of the isolates [17]. Increasing proportions of stG62647 have also been reported in Sweden, Denmark, Germany, Spain, and Canada [16, 18–21]. Conversely, in Japan, the lineage stG6792, which was rare before 2003, has since become the most common emm type [5]. In. a Norwegian study concerning the geographic distribution of SDSE sequence types, it was found that the SDSE population in Norway and Canada shared similar sequence types, while the SDSE population in Japan was more phylogenetically divergent [31].
There are only a few previous studies concerning the associations between emm types and disease severity. StG62647 has been associated with severe clinical outcomes, including necrotizing soft-tissue infections, endocarditis, streptococcal toxic shock syndrome, and death, when compared with other emm types [17]. In a mouse model of necrotizing myositis, stG62647 was shown to be significantly more virulent than emm type stC74a [32]. However, in our study, stG62647 was not significantly associated with severe disease. While the incidence of septic shock was higher in connection with stG62647 compared with other emm types, this difference did not reach statistical significance. In contrast, in our study, stC74a was significantly associated with higher mortality rates. Some investigators have found stC74a to be more prevalent among invasive isolates compared with non-invasive ones [19, 27]. In a Swedish study of SDSE endocarditis, stC74a and stG62647 were the most common emm types, whereas in all invasive isolates in Sweden, stC74a ranked only as the seventh most common [16, 33]. In Japan, emm type stG6792 has been associated with poor clinical outcomes [22]. In another study, emm types stG2078 and stG10 were associated with invasive disease, while stG6792 and stG166b were linked to non-invasive disease [34]. However, many studies concerning emm types and disease severity in SDSE bacteremia are limited by small sample sizes or insufficient availability of clinical data. More research is needed to better understand the associations between emm types and disease severity in SDSE bacteremia.
In a previous study conducted within the same health district as the current study, rarer emm types were associated with severe disease, compared with the five most common ones [14]. Similar findings were reported in Norway, where mortality rates were higher in connection with less common emm types [15]. However, in our current study we did not confirm these results. Instead, we observed that the most prevalent emm types appeared to cause more severe disease and higher case fatality rates, although the differences were not statistically significant. Additionally, our results suggested that even in cases of rarer clinical manifestations, the majority were still caused by the most common emm types.
Both previous studies in Finland and Norway in which rare emm types were associated with severe disease were conducted when the incidence of SDSE bacteremia was much lower, and before the emergence of lineage stG62647. Since then, the incidence rates of both previously common emm types and that of stG62647 have risen significantly. It is possible that these common emm types, along with stG62647, have acquired selective advantages, leading to their dramatic increase in incidence and shifting the spectrum of emm types causing severe disease toward the more common ones.
In the same geographic area as the present study, the incidence of SDSE bacteremia increased from 2.05 to 4.75 episodes per 100,000 inhabitants between 1995 and 2004 [35]. As reported in our previous article, the mean annual incidence during the current study period reached 16.9 per 100,000 inhabitants [10]. The substantial rise in the incidence of SDSE bacteremia in Finland appears to be due to the increased prevalence of common emm types, along with the emergence of stG62647. In addition to potential microbial adaptations, changes in host susceptibility are likely to have contributed to these trends. SDSE primarily causes bacteremia in elderly individuals with multiple comorbidities. In our previous study we identified obesity, diabetes, and coronary artery disease as significant risk factors of SDSE bacteremia. Over the past two decades in Finland, there has been a notable increase in the prevalence of obesity and diabetes, along with a rise in the proportion of individuals aged above 65 years [36–38].
As well as disease severity, previous research on the associations between SDSE emm types and clinical manifestations is limited, with only a few descriptive studies available. In one study no association was found between emm types and clinical outcomes [23]. Regarding S. pyogenes, however, certain emm types have shown associations with specific conditions: emm1 and emm3 have been linked to severe diseases such as necrotizing fasciitis and streptococcal toxic shock syndrome, and emm28 to puerperal sepsis [39]. In our study, stG480 was associated with arthritis, while stG485 more often had an unknown infection focus and it was less frequently associated with skin and soft-tissue infections. No other statistically significant associations between emm types and clinical manifestations were observed. Further studies are needed to determine whether these findings can be confirmed in other populations.
In our study, we found decreased susceptibility (intermediate susceptibility or resistance) to erythromycin in 12% of strains, and to clindamycin in 2%. A comparative analysis covering 1995 to 2004 in the Pirkanmaa Health District revealed decreased susceptibility to erythromycin in 10% of Group G Streptococcus isolates and a 1% decrease as regards clindamycin [9]. However, in other countries, rising trends in erythromycin and clindamycin resistance in SDSE have been reported. In Norway, resistance to both erythromycin and clindamycin, which was previously absent before 2009, increased to 12% during 2016–2018 [40]. Similarly, in Japan, macrolide resistance grew from 10.3% in 2003–2005 to 18.5% in 2010–2013[5, 41].
Previous investigators have reported significant diversity in emm types with respect to antimicrobial susceptibility. In Japan, emm types stG245 and stG10 have been associated with macrolide resistance [5]. In our study, the highest rates of erythromycin and clindamycin resistance were observed in lineage stG245, but no resistance was detected in lineage stG10.
In South Korea, emm type stG254 has been linked to resistance to both macrolides and erythromycin [42].
Our study has several strengths. The study population is relatively large, and it combines emm types with comprehensive clinical data. As a population-based study, it provides reliable distributions of both emm types and clinical manifestations of SDSE bacteremia. The emm typing was thorough, with only one strain remaining non-typeable. Additionally, emm typing had been performed in the same geographic region two decades earlier, allowing for a detailed understanding of changes in emm type distribution.
There are also some limitations. To better assess the associations between emm types and clinical manifestations, an even larger study population would be beneficial. In future, more studies of associations between emm types, clinical manifestations and disease severity are needed.
Conclusion
In this population-based study, the most common emm types causing SDSE bacteremia—stG485, stG480, and stG6—remained consistent with findings from the same geographic region 20 years ago. The most notable change in emm-type distribution was the emergence of stG62647 as the third most common emm type, along with stG6. However, the dramatic rise in the incidence of SDSE bacteremia over the past few decades is not solely due to the emergence of stG62647—the incidence of all major emm types has increased significantly, contributing to the overall surge in SDSE bacteremia. In our study, emm type stC74a was found to be significantly associated with mortality. More studies concerning the associations between emm types, disease severity and clinical manifestations are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rantala S. A Population-based Study of Beta-hemolytic Streptococcal Bacteremia: Epidemiological, clinical and molecular characteristics - Trepo. 2012. Accessed February 20, 2022. https://trepo.tuni.fi/handle/10024/66868
- 2Shimomura Y, Okumura K, Murayama SY, et al. Complete genome sequencing and analysis of a Lancefield group G Streptococcus dysgalactiae subsp. Equisimilis strain causing Streptococcal toxic shock syndrome (STSS). BMC Genomics. 2011;12. 10.1186/1471-2164-12-17.10.1186/1471-2164-12-17PMC 302715621223537 · doi ↗ · pubmed ↗
- 3Oppegaard O, Mylvaganam H, Skrede S, Lindemann PC, Bård, Kittang R. Emergence of a Streptococcus dysgalactiae subspecies equisimilis st G 62647-lineage associated with severe clinical manifestations OPEN. 10.1038/s 41598-017-08162-z 10.1038/s 41598-017-08162-z PMC 554891028790435 · doi ↗ · pubmed ↗
- 4Lambertsen LM, Ingels H, Schønheyder HC, et al. Nationwide laboratory-based surveillance of invasive beta-haemolytic Streptococci in Denmark from 2005 to 2011. Clin Microbiol Infect. 2014;20(4). 10.1111/1469-0691.12378.10.1111/1469-0691.12378 PMC 423200224125634 · doi ↗ · pubmed ↗
- 5EUCAST, Accessed. May 30, 2024. https://www.eucast.org/
- 6Centers for Disease Control and Prevention. Emm Typing Overview and Guidelines. https://www.cdc.gov/strep-lab/php/group-a-strep/emm-typing.html
- 7Broyles LN, Beneden C, Van, Beall B et al. Population-Based study of invasive disease due to b-Hemolytic Streptococci of groups other than A and B. Published Online 2009:48. 10.1086/59703510.1086/59703519187026 · doi ↗ · pubmed ↗
- 8Kaci A, Jonassen CM, Skrede S, Sivertsen A, Steinbakk M, Oppegaard O. Genomic epidemiology of Streptococcus dysgalactiae subsp. Equisimilis strains causing invasive disease in Norway during 2018. Front Microbiol. 2023;14. 10.3389/FMICB.2023.1171913.10.3389/fmicb.2023.1171913 PMC 1036177837485526 · doi ↗ · pubmed ↗