Real-world clinical and economic outcomes associated with supplemental oxygen therapy use among patients with fibrosing interstitial lung disease in the United States
Joseph Yang, Andrea Steffens, Lee Brekke, Amy Anderson, Gursimran Basra, Amy L. Olson, Phani Veeranki, Joao A. de Andrade

TL;DR
This study finds that using supplemental oxygen therapy in patients with fibrosing interstitial lung disease is linked to higher mortality and healthcare costs, likely due to more advanced disease.
Contribution
The study provides real-world evidence on the clinical and economic outcomes of oxygen therapy in fibrosing ILD patients in the U.S.
Findings
Patients using oxygen therapy had significantly higher mortality compared to those who did not.
Oxygen therapy was associated with increased hospitalizations and healthcare resource utilization.
Higher healthcare costs were observed in the oxygen therapy group for both all-cause and fibrosing ILD-related care.
Abstract
Patients with fibrosing interstitial lung disease (ILD) experience a decline in lung function with progressive symptoms, poor response to treatment, and reduced quality of life. While supplemental oxygen therapy is commonly prescribed in clinical practice for patients with fibrosing ILD, the long-term outcomes associated with oxygen therapy remain unclear. This study aimed to address this knowledge gap. This non-interventional study used the Optum® Market Clarity database from 01 October 2015 to 30 June 2022. Patients aged ≥ 18 years with newly diagnosed fibrosing ILD (≥ 2 fibrosing ILD diagnoses on different service dates within 365 days) were included. Patients meeting initial selection criteria were assigned to cohorts based on oxygen therapy initiation. Patients who initiated oxygen therapy following the ILD diagnosis (oxygen therapy cohort) were propensity scores matched 1:1 to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
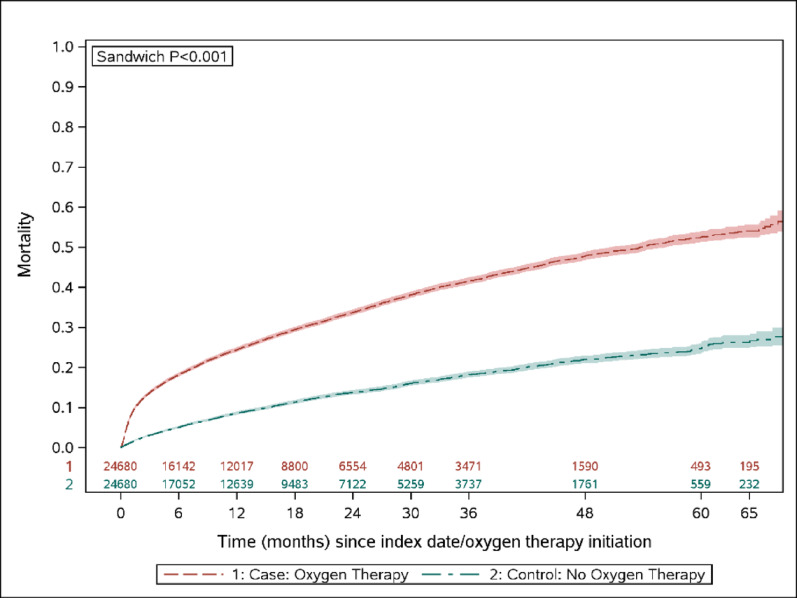 Figure 1
Figure 1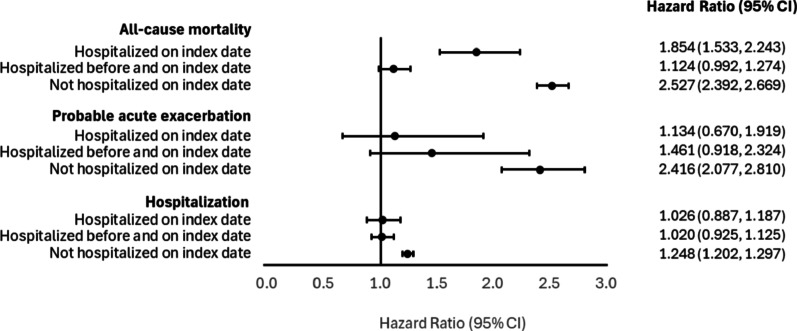 Figure 2
Figure 2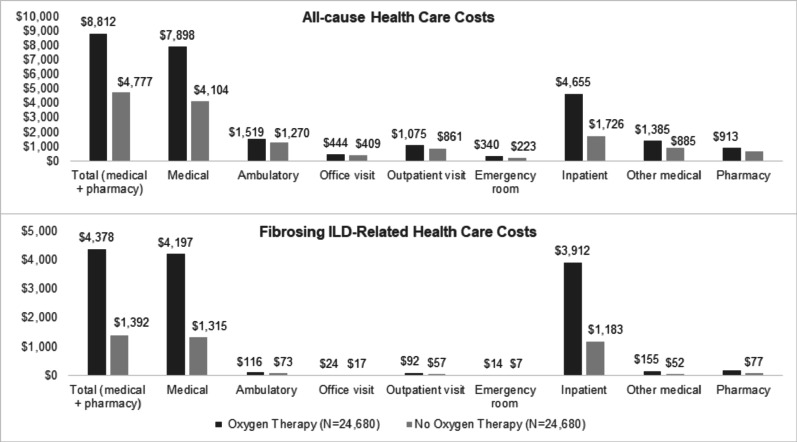 Figure 3
Figure 3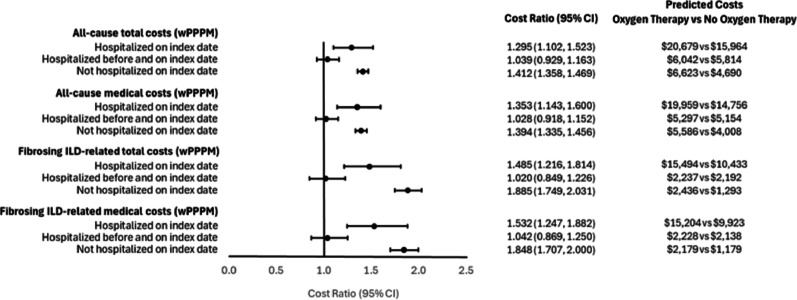 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Chronic Obstructive Pulmonary Disease (COPD) Research · Systemic Sclerosis and Related Diseases
Introduction
Interstitial lung disease (ILD) comprises over 200 distinct lung disorders with various etiologies that are characterized by varying levels of inflammation and fibrosis of the interstitium of the lung [1]. Patients with ILD exhibit common respiratory-related symptoms, including dyspnea and persistent dry cough, which can lead to exertional limitation, hypoxemia, respiratory failure, and death [1, 2]. Among these, a subset of patients with fibrosing ILD develop a progressive phenotype marked by irreversible lung function decline, worsening symptoms, and reduced quality of life, despite standard therapy. Idiopathic pulmonary fibrosis (IPF) is the most common type of progressive ILD without a known cause [3]. Recent studies have underscored the importance of unresolved acute lung inflammation in driving fibrotic changes in the lung [3]. In addition, certain comorbidities such as gastroesophageal reflux disease (GERD) may further drive fibrogenesis through chronic microaspiration, impacting disease progression and prognosis [4]. Recent evidence highlights that patients with progressive fibrosing ILD, including non-IPF subtypes, may share similar clinical trajectories and outcomes, prompting a shift toward phenotype-based management strategies [5].
The major treatment goals in ILD are to slow the lung function decline and improve the symptoms, exercise capacity, and health-related quality of life [6]. Current guideline recommended pharmacologic treatment for ILD includes the antifibrotic agents nintedanib and pirfenidone [7, 8]. Both nintedanib and pirfenidone are indicated for the treatment of IPF, whereas nintedanib has additional indications as a treatment for progressive non-IPF ILD (i.e., progressive pulmonary fibrosis [PPF]) and systemic sclerosis-associated ILD (SSc-ILD). Moreover, immunosuppressants are often used to treat certain forms of PPF, such as those related to connective tissue diseases and hypersensitivity pneumonitis [9]. Despite these therapies, many patients continue to experience progressive clinical deterioration and reduced quality of life [10, 11].
Exertional and resting hypoxemia are common clinical events and are poor prognostic factors among patients with fibrosing ILD [12]. Hypoxemia is accompanied by increased dyspnea and reduced exercise capacity, which further decreases patients’ quality of life. In our recently published study, we found that close to 40% of patients with fibrosing ILD initiated oxygen therapy following their diagnosis [13]. Several clinical guidelines also recommend its use among ILD patients [14–16], however, evidence supporting its use is largely derived from studies on chronic obstructive pulmonary disease (COPD) and based on expert opinions. This highlights the need for studies on the efficacy and long-term effects of oxygen therapy in patients with fibrosing ILD to further refine these recommendations [17].
Long-term oxygen therapy has been suggested to offer benefits such as improved exercise capacity and enhanced health-related quality of life [18–20]. Despite these potential advantages, the evidence regarding its impact on dyspnea reduction and patient survival remains inconclusive, necessitating further research [21, 22]. Moreover, there are challenges associated with oxygen therapy that may counterbalance its long-term benefits, including logistical and financial barriers [23]. Therefore, a deeper understanding of the outcomes related to oxygen therapy is crucial. Building on our prior work that characterized oxygen therapy use in fibrosing ILD, this study leverages real-world data to evaluate the clinical and economic outcomes associated with its initiation [13]. By evaluating the clinical and economic outcomes associated with supplemental oxygen therapy use in patients with fibrosing ILD, we aim to fill these knowledge gaps.
Methods
This study’s methodology builds upon our previously published manuscript that assessed the prevalence of oxygen therapy use among patients with fibrosing ILD [13]. To ensure methodological consistency, we applied similar patient selection criteria and data source as described in our previous work. This approach allows us to extend our previous findings by evaluating outcomes associated with oxygen therapy initiation [13].
Data sources
This retrospective cohort study leveraged Optum’s de-identified Market Clarity Data (Optum^®^ Market Clarity), which includes integrated administrative claims and electronic health record (EHR) data. The database is statistically de-identified under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy Rule’s Expert Determination method and is managed according to Optum^®^ customer data use agreements. The Optum^®^ Market Clarity dataset links EHR data with administrative claims data, including pharmacy claims, physician claims, facility claims (with clinical information), medications prescribed and administered, diagnoses, procedures, and information derived from clinical notes using natural language processing. In this study, only the subset of individuals with health plan enrollment data during the period from 01 October 2015 through 30 June 2022 (study period) were included.
Study population
The study cohort of interest was patients with fibrosing ILD who initiated oxygen therapy after diagnosis. Adult patients (≥ 18 years of age) newly diagnosed with fibrosing ILD were identified from 01 October 2016 through 30 June 2022 (patient identification period). Newly diagnosed fibrosing ILD was defined as ≥ 2 fibrosing ILD diagnoses on different dates of service and within 365 days of each other, with the earliest date of a claim with ILD diagnosis set as the fibrosing ILD diagnosis date. To collect patient demographics and clinical characteristics, 12 months of continuous enrollment in a health plan prior to the fibrosing ILD diagnosis date (pre-ILD baseline period) was required for all patients. Patients with a fibrosing ILD diagnosis in the pre-ILD baseline period or with unknown gender or geographic region were excluded.
Patients meeting the initial selection criteria were stratified further based on the use of oxygen therapy after ILD diagnosis. Patients who initiated oxygen therapy and did not have evidence of oxygen therapy use during the pre-ILD baseline period (oxygen therapy cohort) were propensity scores matched to those who had not yet initiated oxygen therapy (no oxygen therapy cohort). The index date for the oxygen therapy cohort was defined as the first date of a claim for oxygen therapy. For the no oxygen therapy cohort, the index date was assigned to match the duration between the initial ILD diagnosis date and the index date of the matched oxygen therapy patient. The pre-index period was defined as the 12-month period prior to the index date, which may have included the fibrosing ILD diagnosis date. Follow-up for each patient continued until the earliest of the following events: disenrollment from the health plan, death, end of the study period, or initiation of oxygen therapy for a no oxygen therapy cohort patient.
Study measures
Demographic and clinical characteristics
Patient demographic and clinical characteristics included age as of the index year, gender, race, insurance type, US Census region, and the Quan-Charlson comorbidity score, based on diagnosis codes on medical claims [24, 25]. General comorbid conditions were defined with Clinical Classifications Software managed by the Agency for Healthcare Research and Quality (AHRQ) [26]. Provider specialty, medication use (corticosteroids, biologics, calcineurin inhibitors, other immunosuppressants) were also assessed.
Outcomes
Clinical outcomes of interest included time to all-cause mortality, all-cause hospitalization, and probable acute exacerbations. A claims-based algorithm was used to identify probable acute exacerbation, which was defined as meeting all of the criteria: 1) ≥ 1 claim with procedure code for CT scan, 2) evidence of dyspnea within 30 days prior to the date of CT scan, 3) no claims with diagnosis for pulmonary infection, left heart failure, pulmonary embolism or other identifiable causes of acute lung injury within 30 days prior to the date of CT scan, and 4) evidence of high-dose corticosteroid therapy within 15-day window before or after the date of CT scan.
Economic outcomes included all-cause and fibrosing ILD-related health care resource utilization (HCRU) and direct health care costs, measured during the pre-ILD baseline, pre-index, and follow-up periods. HCRU included rate of ambulatory visits (physician office and hospital outpatient), emergency department (ER) visits, inpatient admissions, and pharmacy fills. Health care costs were calculated and presented in categories of pharmacy costs and medical costs (ambulatory [office visits, outpatient visits], ER costs, inpatient stay costs, other medical costs). Health care costs were adjusted to reflect inflation using the annual medical care component of the Consumer Price Index (CPI) [27]. Costs and HCRU were considered fibrosing ILD-related if the claim had a diagnosis in any position for fibrosing ILD, prescription claim for antifibrotic agents, or chest imaging tests (i.e., chest radiography, high-resolution computed tomography).
Statistical analysis
Propensity score matching
To address potential confounding between study outcomes and oxygen therapy status, the oxygen therapy cohort was matched via propensity scores in a 1:1 ratio to the no oxygen therapy cohort. Propensity scores were estimated using the variables measured in the pre-ILD baseline period (fibrosing ILD diagnosis year, age, gender, race, ethnicity, insurance type, comorbidity, medication use, and healthcare resource utilization). For each oxygen therapy cohort patient, a patient from the no oxygen therapy cohort with the closest available propensity score, within a caliper of ± 0.01, was selected. Patients from the oxygen therapy cohort could serve as a no oxygen therapy control for another patient from the oxygen therapy cohort prior to their oxygen therapy initiation. In such instances, the follow-up for these patients concluded one day before they initiated oxygen therapy.
The quality of the match was evaluated by comparing the characteristics included in the propensity score model between cohorts using standardized mean differences (SMD). An SMD of less than 10% was considered an adequate balance between the cohorts. Statistical tests between cohorts included variance adjustments for clustering due to matching. Unmatched patients were excluded from the analysis.
Descriptive analyses
Numbers and percentages were provided for categorical variables; means and standard deviations (SD) were provided for continuous variables. Clinical measures were also reported for the pre-index period to capture any changes in patient status between the fibrosing ILD diagnosis date and the index date. HCRU and cost outcomes were weighted by the minimum follow-up time of each matched pair and reported as weighted per-patient-per-month (wPPPM). Kaplan-Meier analysis was used to estimate the censor-adjusted proportion of patients with all-cause mortality, probable acute exacerbation, and inpatient visits over time.
Multivariable analyses
Multivariable analyses were performed for the key outcomes of interest, adjusting for pre-index characteristics. Differences between cohorts in all-cause and fibrosing ILD-related total and medical costs were assessed using generalized linear models with a gamma distribution and log link. Cox proportional hazards regression modeling was used to assess differences between cohorts in the hazard of all-cause mortality, probable acute exacerbation, and hospitalization. Three distinct hazard ratios (HR) and costs ratios were reported to account for significant interactions observed between cohort and inpatient setting at index date (i.e., hospitalized on the index date, hospitalized before and on the index date, not hospitalized on the index date).
Results
Pre-ILD baseline demographic and clinical characteristics
Among 93,578 patients meeting the initial cohort selection criteria, 24,686 (26.4%) initiated oxygen therapy after the fibrosing ILD diagnosis date (Supplementary Fig. 1). After matching, a total of 49,360 patients were included in the final study sample, of which 24,680 patients (50.0%) were included in the oxygen therapy cohort and 24,680 (50.0%) were included in the no oxygen therapy cohort.
The post-match baseline demographic and clinical characteristics were similar between the study cohorts (Table 1). The mean age at the initial ILD diagnosis was 68.9 years for both cohorts. In the matched oxygen therapy vs. no oxygen therapy cohorts, patients were predominantly male (51.2% vs. 50.6%; SMD = 1.01%), White (68.7% vs. 68.8%, SMD = 0.18%), from the Midwest (40.3% vs. 39.9%, SMD = 0.69%), and had Medicare insurance coverage (47.6% vs. 47.9%, SMD = 0.58%). The mean (SD) Charlson comorbidity score was 2.6 (2.4) and 2.5 (2.4), and COPD was the most commonly observed respiratory disease (37.0% vs. 37.6%, SMD = 1.22%) (Table 1).
Table 1. Post-match pre-ILD baseline patient demographic and clinical characteristicsDemographicsOxygen therapy(N=24,680)No oxygen therapy(N=24,680)Standardized mean difference (%) Age (continuous) 68.8868.89-0.09Index age group, n (%)18-441,320 (5.35)1,272 (5.15)0.8745-647,444 (30.16)7,472 (30.28)-0.2565+15,916 (64.49)15,936 (64.57)-0.17 Gender, n (%) Female12,056 (48.85)12,181 (49.36)-1.01Male12,624 (51.15)12,499 (50.64)1.01 Region, n (%) Northeast5,386 (21.82)5,387 (21.83)-0.01Midwest9,937 (40.26)9,854 (39.93)0.69South6,893 (27.93)6,945 (28.14)-0.47West2,464 (9.98)2,494 (10.11)-0.40 Race, n (%) White16,955 (68.70)16,976 (68.78)-0.18African-American2,396 (9.71)2,403 (9.74)-0.10Asian350 (1.42)342 (1.39)0.28Unknown4,979 (20.17)4,959 (20.09)0.20 Ethnicity, n (%) Hispanic980 (3.97)1,009 (4.09)-0.60Not Hispanic17,124 (69.38)17,091 (69.25)0.29Unknown6,576 (26.65)6,580 (26.66)-0.04 Insurance type, n (%) Commercial only7,595 (30.77)7,563 (30.64)0.28Medicare only11,741 (47.57)11,812 (47.86)-0.58Medicaid only2,393 (9.70)2,328 (9.43)0.90Multiple known types2,248 (9.11)2,260 (9.16)-0.17Unknown type703 (2.85)717 (2.91)-0.34 Fibrosing ILD year ^1^ , n (%) 20161,903 (7.71)2,226 (9.02)-4.7320175,483 (22.22)6,242 (25.29)-7.2320184,726 (19.15)5,073 (20.56)-3.5320194,356 (17.65)4,394 (17.80)-0.4020203,518 (14.25)3,268 (13.24)2.9420213,677 (14.90)2,938 (11.90)8.8020221,017 (4.12)539 (2.18)11.10 Index year, n (%) 2016500 (2.03)832 (3.37)-8.3120173,382 (13.70)4,064 (16.47)-7.7320184,093 (16.58)4,456 (18.06)-3.8920194,577 (18.55)4,683 (19.97)-1.1020204,365 (17.69)4,335 (17.56)0.3220215,348 (21.67)4,495 (18.21)8.6620222,415 (9.79)1,815 (7.35)8.69Charlson comorbidity score^2^ (continuous), mean (SD)2.58 (2.41)2.53 (2.36)2.33 Charlson comorbidity score (categorical), n (%) 05,154 (20.88)5,004 (20.28)1.501-28,877 (35.97)9,290 (37.64)-3.473-45,885 (23.85)5,907 (23.93)-0.215+4,764 (19.30)4,479 (18.15)2.96 Underlying ILD type during the study period (mutually exclusive), n (%) Autoimmune ILD3,205 (12.99)3,581 (14.51)-4.43Hypersensitivity Pneumonitis6,492 (26.30)6,099 (24.71)3.65Sarcoidosis519 (2.10)502 (2.03)0.48Multiple1,333 (5.40)1,586 (6.43)-4.35Unclassified IIP13,131 (53.21)12,912 (52.32)1.78IPF2414 (9.78)2,435 (9.87)-0.29 Medications, n (%) Antifibrotics22 (0.09)24 (0.10)-0.27Corticosteroids9,181 (37.20)9,500 (38.49)-2.67Biologics714 (2.89)741 (3.00)-0.65Calcineurin inhibitors237 (0.96)223 (0.90)0.59Other immunosuppressants824 (3.34)928 (3.76)-2.28 Respiratory diseases, n (%) Pulmonary hypertension1,928 (7.81)1,863 (7.55)0.99Acute respiratory failure2,781 (11.27)2,346 (9.51)5.78Asthma3,967 (16.07)4,106 (16.64)-1.52COPD9,140 (37.03)9,286 (37.63)-1.22Pneumonia6,157 (24.95)5,892 (23.87)2.50Lung transplantation62 (0.25)69 (0.28)-0.55Lung cancer1,071 (4.34)1,071 (4.34)0.00Cystic fibrosis48 (0.19)53 (0.21)-0.45Respiratory tract infection8,033 (32.55)8,222 (33.31)-1.63Upper respiratory tract infection5,247 (21.26)5,420 (21.96)-1.70Lower respiratory tract infection4,516 (18.30)4,662 (18.89)-1.52 Other clinical characteristics, n (%) Gastroesophageal reflux disease (GERD)8,221 (33.31)8,193 (33.20)0.24Heart failure5,872 (23.79)5,601 (22.69)2.60Obstructive sleep apnea4,452 (18.04)4,540 (18.40)-0.92Smoking status, n (%)10,294 (41.71)10,152 (41.13)1.17Two-sample t-test was used for continuous measuresZ-test using robust standard errors in an OLS regression was used for continuous measuresPearson chi-square test was used for binary measuresRao-Scott test was used for binary measures^1^The identification period used only partial years in 2016 (October – December) and 2022 (January – July)^2^Ref. [25]
Clinical and economic outcomes
Clinical outcomes
The mean (SD) length of follow-up among the oxygen therapy vs. no oxygen therapy was 16.6 (16.2) and 17.7 (16.4) months, respectively. The mean (SD) duration between the initial fibrosing ILD diagnosis and the index date for both cohorts was 8.5 (12.6) months. At 65 months, a significantly higher percentage of the oxygen therapy cohort had died compared to the no oxygen therapy cohort (Kaplan-Meier adjusted percentages of 54.0% vs. 26.3%, p < 0.001; Fig. 1). Similarly, a significantly higher percentage of the oxygen therapy cohort experienced hospitalization and probable acute exacerbation during the follow-up period (Supplementary Figs. 2 and 3).
Fig. 1. Time-to-all-cause mortality from the index date during follow-up
We observed a significant difference in all-cause mortality risk between the cohorts using the Cox proportional hazards regression model, adjusting for the clinical characteristics measured during the pre-index period. Among patients who were not hospitalized on the index date, the oxygen therapy cohort had 2.5-fold higher risk of all-cause mortality vs. no oxygen therapy (HR = 2.52; 95% confidence interval [CI] = 2.39–2.67; Fig. 2). Similar trends were observed for hospitalization (HR = 1.24; 95% CI = 1.20–1.30) and probable acute exacerbation (HR = 2.41; 95% CI = 2.08–2.81). Among patients who were hospitalized on the index date, the oxygen therapy cohort had 85% higher risk of all-cause mortality vs. no oxygen therapy (HR = 1.85; 95% CI = 1.53–2.24; Fig. 2), whereas the adjusted HRs for probable acute exacerbation and hospitalizations were not statistically significant. Lastly, the adjusted HRs for all-cause mortality, probable acute exacerbation, and hospitalization were not statistically significant among patients who were hospitalized before and continued till the index date. Fig. 2. Adjusted hazard ratios ofall-cause mortality, probable acute exacerbation, and hospitalization, oxygen therapy vs. nooxygen therapy
Economic outcomes
During the follow-up period, the oxygen therapy cohort had significantly higher all-cause and fibrosing ILD-related HCRU compared to the no oxygen therapy cohort across all categories. The oxygen therapy cohort had higher wPPPM ambulatory visits (2.64 [2.81] vs. 2.30 [2.51], p < 0.001), emergency room visits (0.24 [0.52] vs. 0.17 [0.46], p < 0.001), and inpatient stays (0.09 [0.21] vs. 0.05 [0.16], p < 0.001) (Table 2).
Table 2. All-cause and fibrosing ILD-related health care resource utilization during the follow-up periodOxygen therapy (N=24,680)No oxygen therapy(N=24,680)p-value All-cause HCRU counts, mean (SD), wPPPM Ambulatory visits2.64 (2.81)2.30 (2.51)<0.001Office visits1.47 (1.67)1.38 (1.52)<0.001Outpatient visits1.20 (2.01)0.93 (1.77)<0.001Emergency room visits0.24 (0.52)0.17 (0.46)<0.001Inpatient stays0.09 (0.21)0.05 (0.16)<0.001Length of stay, days1.24 (4.35)0.54 (3.46)<0.001Pharmacy fills4.21 (4.10)3.57 (3.85)<0.001 Fibrosing ILD-related HCRU counts, mean (SD), wPPPM Ambulatory visits0.34 (0.57)0.21 (0.40)<0.001Office visits0.13 (0.27)0.09 (0.20)<0.001Outpatient visits0.21 (0.44)0.13 (0.32)<0.001Emergency room visits0.08 (0.21)0.05 (0.19)<0.001Inpatient stays0.06 (0.18)0.02 (0.11)<0.001Length of stay, days0.98 (3.78)0.36 (3.27)<0.001Pharmacy fills0.02 (0.11)0.01 (0.07)<0.001HCRU health care resource utilization, wPPPM weighted per-patient-per-monthFibrosing-ILD-related is defined as any diagnosis of fibrosis or a claim for chest imaging or a claim for antifibrotic medication
The mean (SD) wPPPM all-cause total costs were significantly higher in the oxygen therapy cohort vs. no oxygen therapy cohort (27,142] vs. 13,571], p < 0.001; Fig. 3). The proportions of total costs attributable to medical costs were 89.6% and 85.9% in the oxygen therapy and no oxygen therapy cohorts, respectively. Inpatient costs were the major contributor to medical costs in both cohorts, accounting for 58.9% and 42.0% in oxygen therapy and no oxygen therapy cohorts, respectively. Similar trends were observed for fibrosing ILD-related costs.
Fig. 3. Follow-up period weighted all-cause andfibrosing ILD-related total costs
We observed significant differences in cost ratios between the cohorts after adjusting for the pre-index characteristics. Among patients who were not hospitalized on the index date, the oxygen therapy cohort had 41% higher all-cause total costs (adjusted cost ratio [aCR] = 1.41; 95% CI = 1.36–1.47) and 39% higher all-cause medical costs (aCR = 1.39; 95% CI = 1.34–1.46) compared to the no oxygen therapy cohort (Fig. 4). Among patients who were hospitalized on the index date, the oxygen therapy cohort had 30% higher all-cause total costs (aCR = 1.30; 95% CI = 1.10–1.52) and 35% higher all-cause medical costs (aCR = 1.35; 95% CI = 1.14–1.60). Similar trends were observed for the fibrosing ILD-related total and medical costs (Fig. 4).
Fig. 4. Multivariable Generalized Linear Regression Model: Adjusted cost ratios and predicted costs for all-cause and fibrosing ILD-related total and medical costs, oxygen therapy vs no oxygen therapy
Discussion
This study evaluated the long-term clinical and economic outcomes among patients with fibrosing ILD who initiated oxygen therapy compared to those who did not initiate oxygen therapy in the real-world setting. Our findings demonstrated that the oxygen therapy cohort had significantly higher rates of all-cause mortality, hospitalizations, and probable acute exacerbations during the follow-up period compared to the no oxygen therapy cohort. Furthermore, the oxygen therapy cohort had higher HCRU and incurred higher total healthcare costs compared to no oxygen therapy cohort. The study findings remained consistent after multivariate analyses with adjustment for pre-index characteristics.
To our knowledge, this is the first real-world study to comprehensively evaluate both clinical and economic outcomes associated with oxygen therapy in patients with fibrosing ILD. Our findings are aligned with prior observational studies that suggested an association between oxygen therapy and disease progression [28–30]as well as an increased risk of death or lung transplant [30]. From a clinical standpoint, it is possible that the higher rates of adverse clinical outcomes among oxygen users are merely a reflection of disease progression and severity. In fact, previous studies have employed oxygen therapy use as a proxy for ILD disease progression in studies using administrative claims data [31, 32] .
Interestingly, when stratifying by hospitalization status at or before the index date, the association between oxygen therapy and adverse outcomes was attenuated, with hazard ratios for most outcomes no longer statistically significant. This suggests that hospitalization itself may be a strong indicator of disease severity, potentially overshadowing the prognostic value of oxygen therapy for clinical outcomes. This implies once patients reach a certain level of disease severity, as reflected by recent or ongoing hospitalizations, the additional risk being associated with oxygen therapy becomes less apparent. This highlights the importance of considering hospitalization as a co-occurring marker of disease progression when interpreting the impact of oxygen therapy.
This study adds novel insights relevant for policy and population health decision makers by quantifying the incremental healthcare burden associated with oxygen therapy in this population, using a large, nationally representative real-world dataset. Our study findings provide additional evidence and reinforce that patients with progressive fibrosing ILD have higher HCRU and incur greater health care costs compared to those without progression [31-34] .
Moreover, initiation of oxygen therapy is an important landmark in a patient’s clinical trajectory, and previous research indicates that supplemental oxygen therapy is correlated with decreased quality of life across various domains, such as emotional well-being, independence, and social participation [35-39] . The DISCOVERY study revealed complex patterns regarding outcomes among patients with ILD who initiated oxygen therapy. The initial study results demonstrated that patients with ILD experienced increased acute exacerbations and hospitalizations following long-term oxygen therapy initiation over a 12-month period. However, sensitivity analyses of ILD patients with adequate 12-month follow-up data demonstrated the opposite effect—showing reduced acute exacerbations and all-cause hospitalizations [40] . These divergent findings underscore the complexity of oxygen therapy’s impact in ILD, suggesting that outcomes may vary significantly based on care quality, follow-up duration, and patient selection criteria. Collectively, these results support the clinical relevance of oxygen therapy as a marker of disease severity and healthcare burden, even as its direct therapeutic effects remain complex and context dependent. Therefore, delaying the need for oxygen therapy may represent a clinically meaningful goal. Therapies aimed at delaying or reducing the lung function decline and ILD progression, hence the need for oxygen therapy use in patients with ILD have the potential to improve clinical and economic outcomes in this population. Continued research and investment in such therapeutic options are warranted, and future clinical trials ought to consider using it as an outcome measure.
Limitations
This study has several limitations that need to be considered when interpreting the results. While we utilized robust matching procedures to balance the study cohorts, this study lacked access to clinical measures of disease severity, such as forced vital capacity (FVC), or radiological assessments which are typically available only through registries or prospective studies. As a result, we were unable to directly adjust for lung function decline. Future research using registry data or other sources that capture pulmonary function metrics will be important to validate and extend these findings. Additionally, identification of newly diagnosed fibrosing ILD patients relied on a claims-based algorithm, and the presence of a diagnosis code does not necessarily indicate presence of disease. To mitigate misidentification of ILD patients, a confirmatory diagnosis was required, and patients without ILD diagnosis in the 12-month pre-ILD baseline period were considered newly diagnosed. We also recognize that coding errors may result in inaccurate or incomplete data, leading to potential misclassification of variables of interest that could have biased our findings. Lastly, our study findings cannot be generalized to uninsured populations and patients with health plans not represented in the database.
Conclusion
This study provides insights into the real-world clinical and economic burden experienced by patients with fibrosing ILD who initiate oxygen therapy. Patients with fibrosing ILD who initiated oxygen therapy are associated with a higher incremental economic burden, primarily driven by increased hospitalization costs, and experienced increased rates of adverse clinical outcomes compared to patients who did not initiate oxygen therapy. Importantly, this study does not suggest that oxygen therapy itself causes harm; rather, oxygen use likely reflects more advanced disease and may serve as a surrogate for poor prognosis. Future management strategies and novel therapies that reduce ILD progression and hence the need for oxygen therapy could potentially alleviate clinical and economic burden in this population additionally.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 150 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Visca D, Mori L, Tsipouri V, et al. Effect of ambulatory oxygen on quality of life for patients with fibrotic lung disease (Amb Ox): a prospective, open-label, mixed-method, crossover randomised controlled trial. Lancet Respir Med. 2018;6(10):759–70. 10.1016/s 2213-2600(18)30289-3.10.1016/S 2213-2600(18)30289-330170904 · doi ↗ · pubmed ↗
- 2Tonga KO, Oliver BG. Effectiveness of pulmonary rehabilitation for chronic obstructive pulmonary disease therapy: focusing on traditional medical practices. J Clin Med. 2023;12(14):4815 . 10.3390/jcm 1214481510.3390/jcm 12144815 PMC 1038185937510930 · doi ↗ · pubmed ↗
- 3Bell EC, Cox NS, Goh N, et al. Oxygen therapy for interstitial lung disease: a systematic review. Eur Respir Rev. 2017;26(143):160080 . 10.1183/16000617.0080-201610.1183/16000617.0080-2016 PMC 948902128223395 · doi ↗ · pubmed ↗
- 4Agency for Healthcare Research and Quality. Clinical classification software (CCS) for ICD-10-CM. https://www.hcup-us.ahrq.gov/toolssoftware/ccs 10/ccs 10.jsp. Accessed February 22, 2023.
- 5US Department of Labor Bo LS. Consumer Price Index. Medical Care. Series ID: CUUR 0000 SAM. Accessed September 17, 2023. http://data.bls.gov/cgi-bin/surveymost?cu
- 6Singer D, Bengtson LGS, Conoscenti CS, et al. Burden of illness in progressive fibrosing interstitial lung disease. J Manag Care Spec Pharm. Aug 2022;28(8):871-880. 10.18553/jmcp.2022.28.8.87110.18553/jmcp.2022.28.8.871PMC 1037303735876293 · doi ↗ · pubmed ↗
- 7Nili M, Steffens A, Anderson A, et al. Health care costs and utilization of progressive fibrosing lung disease by underlying interstitial lung disease type. J Manag Care Spec Pharm. Feb 3 2024;30(2):163-174. 10.18553/jmcp.2024.30.2.16310.18553/jmcp.2024.30.2.163PMC 1083945938308627 · doi ↗ · pubmed ↗
- 8Collard HR, Chen SY, Yeh WS, et al. Health care utilization and costs of idiopathic pulmonary fibrosis in U.S. Medicare beneficiaries aged 65 years and older. Ann Am Thorac Soc. Jul 2015;12(7):981-7. 10.1513/Annals ATS.201412-553OC 10.1513/Annals ATS.201412-553OC 25923447 · doi ↗ · pubmed ↗