Assessing first-line treatment for advanced EGFR-mutated NSCLC in diverse clinicopathological subgroups: a systematic review and network meta-analysis
Ting Mei, Ting Wang, Qinghua Zhou

TL;DR
This study identifies the best first-line treatments for advanced EGFR-mutated lung cancer based on patient characteristics like age and mutation type.
Contribution
The study provides subgroup-specific treatment recommendations for EGFR-mutated NSCLC using network meta-analysis of diverse clinicopathological factors.
Findings
Osimertinib plus chemotherapy improves progression-free survival across most patient subgroups.
Amivantamab plus lazertinib offers the best overall survival outcomes in specific mutation and gender subgroups.
Treatment combinations like afatinib plus cetuximab and dacomitinib show OS benefits in 19del and L858R mutation subgroups.
Abstract
This network meta-analysis (NMA) aimed to indicate the most effective first-line therapeutic options for advanced EGFR-mutated NSCLC, particularly considering their specific clinicopathological characteristics. Articles in the EMBASE, Cochrane Library, PubMed, and Web of Science databases and conference abstracts published as of December 2023, were searched to obtain data from randomized controlled trials (RCTs) of the first-line treatment of advanced EGFR-mutated NSCLC cases with EGFR-TKIs alone or together with other agents. 37 RCTs including 24 treatment regimens were incorporated into this NMA. With respect to the overall patient cohort, osimertinib + chemotherapy (CT) was associated with the greatest benefit to progression-free survival (PFS), whereas amivantamab + lazertinib yielded the greatest benefit to overall survival (OS). Osimertinib + CT yielded the best PFS outcomes…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
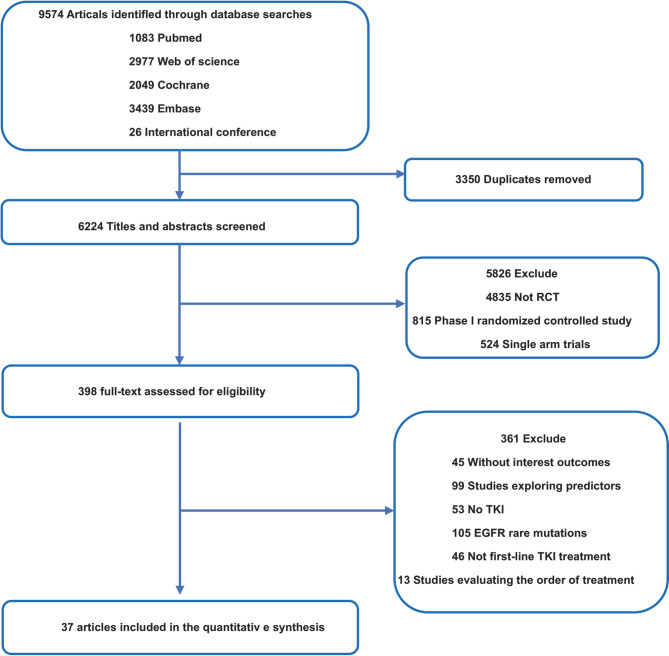 Figure 1
Figure 1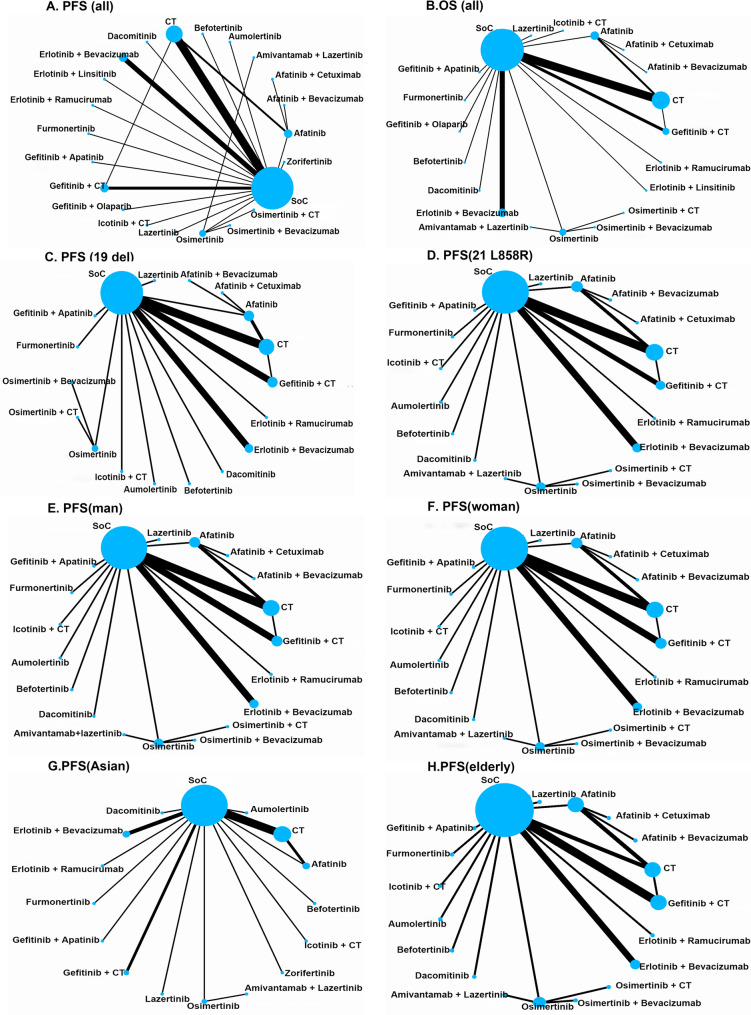 Figure 2
Figure 2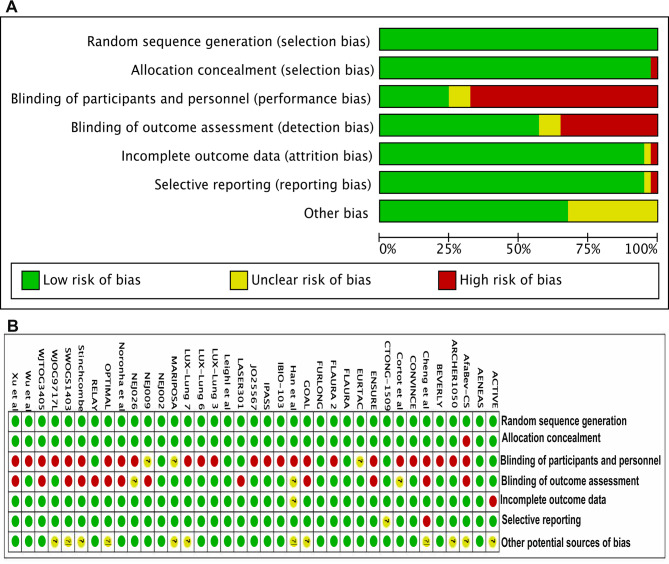 Figure 3
Figure 3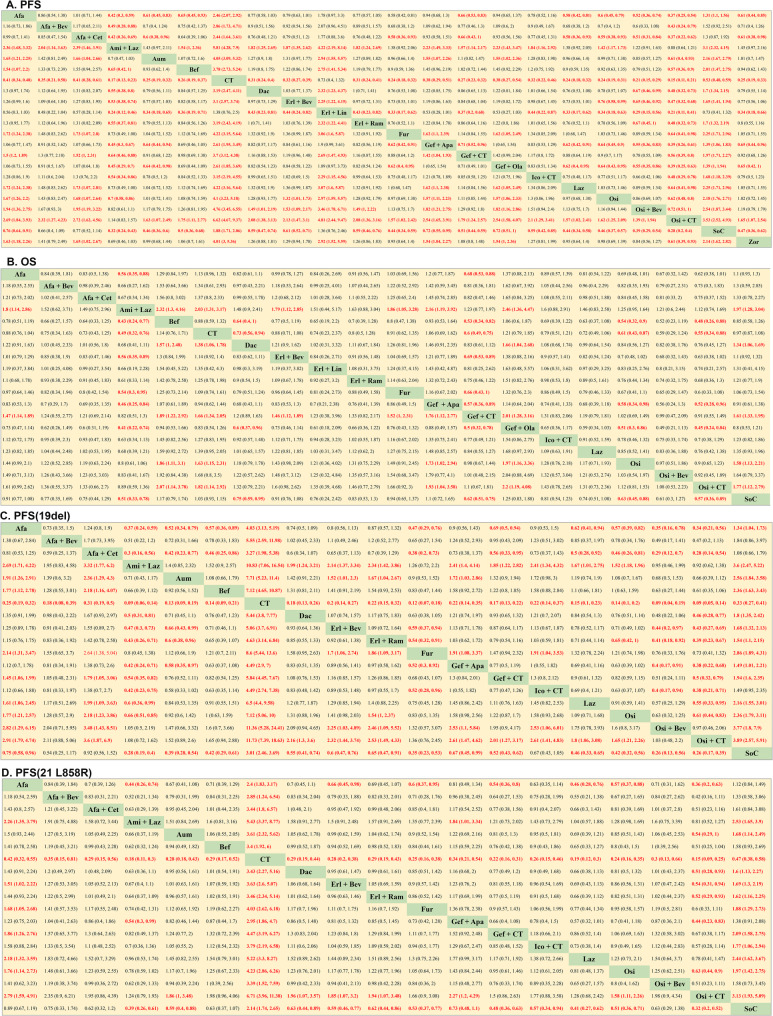 Figure 4
Figure 4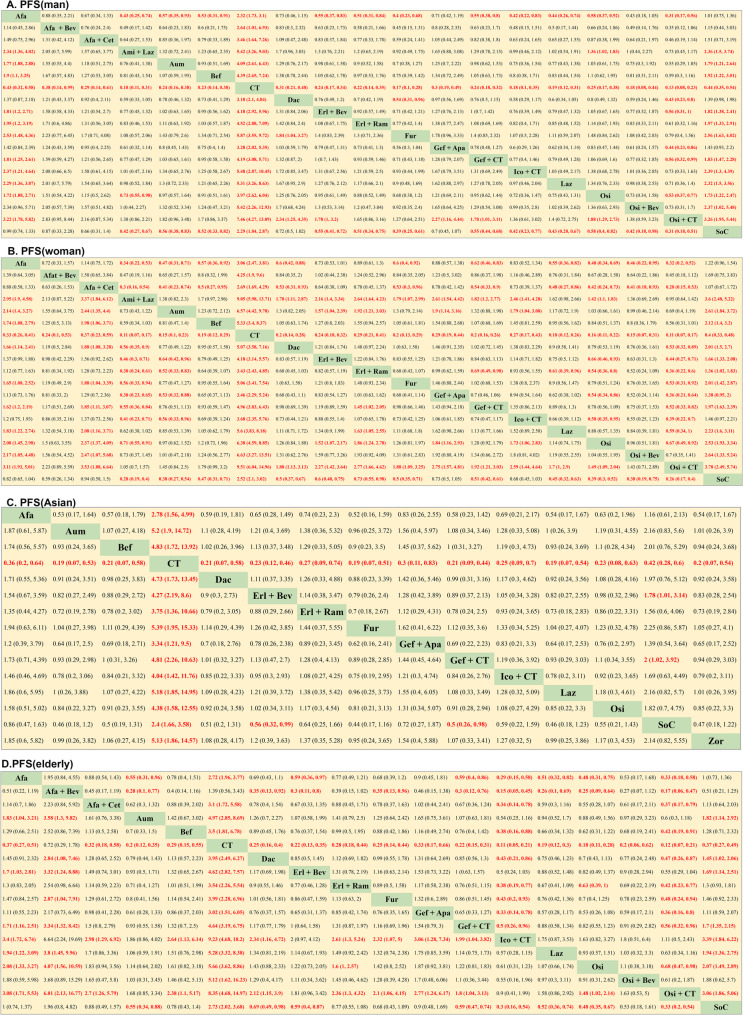 Figure 5
Figure 5- —Regional Innovation Cooperation Project of Sichuan Science and Technology Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Colorectal Cancer Treatments and Studies · Chronic Myeloid Leukemia Treatments
Introduction
Lung cancer bears the unfortunate distinction of being the foremost contributor to cancer-related mortality on a global scale, with NSCLC representing a staggering 85% of diagnosed lung tumor cases [1, 2]. Within the landscape of NSCLC tumors, EGFR mutations emerge as prominent drivers, with the exon 21 Leu858Arg (21L858R) mutation and the exon 19 deletion (19del) standing out as the two most prevalent and clinically significant subtypes [3–5].
EGFR-mutated NSCLC first-line intervention usually includes a variety of EGFR-TKI, namely, 1st-generation EGFR-TKI (gefitinib, erlotinib and icotinib), 2nd-generation EGFR-TKI (dacomitinib and afatinib), and 3rd-generation EGFR-TKI (osimertinib, furmonertinib, almonertinib) [6–9]. Improvement of the efficacy of TKI treatment or to slowing down the onset of therapeutic resistance emerged notable objectives, and researchers have increasingly explored the administration of first-line combination therapies for advanced EGFR-mutated NSCLC, including combining TKIs and chemotherapeutic or anti-angiogenic drugs [10]. In one prior network meta-analysis (NMA) evaluating these various first-line approaches to the therapy of NSCLC cases with advanced EGFR-mutated disease, the investigators identified that osimertinib in isolation exhibited the most favorable patient progression-free survival (PFS), while the combination of gefitinib and pemetrexed-based chemotherapy was linked to superior overall survival (OS) rates [11]. Recently, there have been multiple promising breakthroughs in the first-line therapy of advanced EGFR-mutated NSCLC cases including those derived from the FLAURA2 study [12], MARIPOSA study [13], LASER301 study [14], and IBIO-103 study [15]. This raises the question of whether these results may alter the conclusions of the previous NMA, offering new guidance for therapeutic decision-making. As such, additional comprehensive comparative analyses are essential to delineate the most optimal first-line therapeutic approaches for NSCLC cases carrying EGFR mutations.
At present, first-line EGFR-TKI treatment is recommended for NSCLC cases with both EGFR 19del and EGFR 21L858R mutations, which are classified as completely distinct disease subtypes. Relative to 19del NSCLC, 21L858R disease is associated with more aggressive growth, higher rates of concomitant mutations, reduced EGFR-TKI sensitivity, and other distinct molecular characteristics [16–19]. EGFR mutation subtypes should thus be taken into consideration when selecting patient treatments. There are also differences in the prevalence of driver gene mutations when comparing Asian and non-Asian patient cohorts, and the ARCHER 1050, LUX-Lung3, and FLAURA trials all reported significant differences in therapeutic outcomes when comparing patients of different ethnicities [20–22]. Several other clinicopathological factors beyond ethnicity and EGFR mutation status have also been shown to be relevant to patient prognosis and treatment outcomes, including sex and age, emphasizing their relevance to treatment protocol planning [23, 24]. At present, however, given the ambiguity surrounding the most efficacious treatment strategies for advanced NSCLC cases with distinct EGFR mutation subtypes and clinicopathological profiles, uncertainties persist.
To address these questions, we conducted this NMA, which has been widely used in the absence of head-to-head trial data, to provide an in-depth exploration of the optimal first-line treatment for patients with advanced EGFR-mutant NSCLC. By comparing the efficacy of individual treatment regimens in subgroups of patients with specific clinical and pathological characteristics, this study can provide a solid basis for selecting appropriate treatment regimens for patients.
We present this article in accordance with the PRISMA reporting checklist.
Methods
Conducted on the basis of the guidelines outlined in the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) checklist extension for NMAs, it was attempted to register this study on PROSPERO (ID# CRD42024506995) (Table S1).
Data sources
The Embase, Cochrane Library, Web of Science, and PubMed databases, in conjunction with conference abstracts, underwent a precise systematic search. This search aimed to involve randomized controlled trials (RCTs) published in English up to December 2023, specifically concentrating on trials that included EGFR-TKI regimens in at least one arm. Full details regarding the utilized search strategy are demonstrated in Table S2. Moreover, the title, abstract, and full text of retrieved articles were independently evaluated by two scholars for the purpose of indicating whether the studies met the defined eligibility criteria, with all discrepancies being resolved by a third investigator.
Study inclusion
For eligibility in this NMA, studies were required to meet specific criteria: (1) They had to be Phase II or III RCTs concentrating on cases diagnosed with histologically or cytologically confirmed EGFR mutation-positive advanced NSCLC at stage III, IV, or relapsed stage (patients with advanced NSCLC who have relapsed after previous radical treatment); (2) RCTs comparing a minimum of two first-line therapies, at least one of which included an EGFR-TKI; and (3) RCTs that reported at least one outcome, including OS or PFS. Studies were excluded if they were: (1) trials in which the test treatments were provided as maintenance, adjuvant, or neoadjuvant therapy; (2) trials utilizing radiotherapy or immunotherapy; or (3) reviews, editorials, letters, case reports, author responses, or articles not published in English. When more than one study originated from a single trial, only the most complete was included in this NMA.
Study outcomes and data collection
Data extraction involved the utilization of standardized tables to capture key information, involving study ID, therapeutic modality, first author, publication year, study arms, study design, and total participant count. This extraction process was conducted independently by two investigators. The outcomes for this NMA were patient OS and PFS.
Quality assessment
It was attempted to figure out the level of the RCTs through the Cochrane Risk of Bias tool according to seven possible sources of bias (random sequence generation, allocation concealment, personnel and participant blinding, selective reporting, incomplete outcome data, outcome assessment blinding, and others). Two investigators independently assigned a high (red), medium (yellow), or low (green) risk of bias to each of these items.
Data synthesis and assessment
Utilizing STATA 16.0, direct and indirect comparisons of different therapeutic strategies were undertaken through network geometry maps. Survival outcomes were evaluated based on hazard ratios (HRs) for PFS and OS with 95% CIs Evaluating heterogeneity was executed through I^2^ statistic, with I^2^ < 25%, 25–50%, and >50% respectively indicating low, intermediate, and high heterogeneity levels. Random-effect models were used whenever I^2^ >50% [25]. The statistical global inconsistency test was utilized to evaluate the overall network model for global inconsistency, while differences among the direct and indirect comparisons within a closed treatment loop were evaluated through a node-splitting analysis. A P threshold below 0.05 was suggestive of statistical significance. The Markov chain Monte Carlo method was implemented using the “JAGS” (v 4.3.0) and “getmtc” (v 0.8.2) packages in R (v 4.0.2) for fixed effects and consistency models. The establishment of posterior distributions involved the deployment of four separate and independent Markov chains, all concurrently assessing individual outcomes. This rigorous process consisted of 5,000 burn-in iterations followed by 20,000 inference iterations per chain. It was attempted to figure out convergence of the model through trace plots and the Brooks-Gelman-Rubin method. Subsequently, the Bayesian approach was employed to thoroughly analyze the surface under the cumulative ranking curve (SUCRA) for each treatment modality. Higher SUCRA values were interpreted as denoting superior efficacy [26]. Publication bias was examined utilizing funnel plots, and absence of publication bias was presented by symmetrical plots [27].
Results
In total, this study incorporated 37 RCTs (11 phase II RCTs, 26 phase III RCTs) enrolling 11,539 patients and employing 24 treatment regimens (Table 1) [12–15, 28–60]. A detailed study selection flowchart is presented in Fig. 1. A comparison of the outcomes in this study, which included the PFS and OS of the overall patient cohort and the PFS of male, female, elderly (≥ 65 years), Asia, EGFR 19del, and EGFR L858R cases is presented in Fig. 2. A comparison of the OS of male, female, elderly, Asian, EGFR 19del, and EGFR L858R cases is presented in Figure S1.Table 1. Baseline characteristics of 37 studiesStudy IDYearFirst authorTrial phaseTotal numberArmNeoadjuvant treatmentFLAURA2018Jean-Charles SoriaIII2791Oral osimertinib2772Standard oral EGFR-TKI (gefitinib or erlotinib)CTONG-15092018Qing ZhouIII1571Erlotinib plus bevacizumab1542ErlotinibNEJ0092019Yukio HosomiIII1721Gefitinib plus carboplatin and pemetrexed1702GefitinibENSURE2015Yilong WuIII1101Erlotinib1072Gemcitabine/cisplatin (GP)Noronha et al.2020Vanita NoronhaIII1761Gefitinib plus carboplatin and pemetrexed1742GefitinibHan et al.2017Baohui HanII401Gefitinib plus carboplatin and pemetrexed402Carboplatin and pemetrexed413GefitinibARCHER10502017Yi-Long WuIII2271Dacomitinib2252GefitinibLUX-Lung 32016Martin SchulerIII2301Afatinib1152Cisplatin and pemetrexedLUX-Lung 62014Yi-Long WuIII2421Afatinib1222Cisplatin plus gemcitabineLUX-Lung 72016Keunchil ParkIIB1601Afatinib1592GefitinibJO255672014Takashi SetoII771Erlotinib plus bevacizumab772ErlotinibNEJ0262019Haruhiro SaitoIII1121Erlotinib plus bevacizumab1122ErlotinibRELAY2019Kazuhiko NakagawaIII2241Erlotinib plus ramucirumab2252ErlotinibACTIVE2021Hongyun ZhaoIII1571Gefitinib and apatinib1562GefitinibWJOG9717L2022Hirotsugu KenmotsuII611Osimertinib plus bevacizumab612OsimertinibAENEAS2022Shun LuIII2141Aumolertinib2152GefitinibBEVERLY2022Maria Carmela PiccirilloIII801Erlotinib plus bevacizumab802ErlotinibAfaBev-CS2023Takashi NinomiyaII491Afatinib plus bevacizumab502AfatinibFLAURA22023David PlanchardIII2791Osimertinib plus chemotherapy2782OsimertinibMARIPOSA2023Byoung Chul ChoIII4291Amivantamab plus lazertinib4292OsimertinibFURLONG2022Yuankai ShiIII1781Furmonertinib1792GefitinibCheng et al.2016Ying ChengII1291Gefitinib plus pemetrexed662GefitinibLASER3012023Byoung Chul ChoIII1961Lazertinib1972GefitinibWu et al.2023Yi-Long WuIII2201Zorifertinib2192Gefitinib or erlotinibIBIO-1032023Shun LuIII1821Befotertinib1802IcotinibCONVINCE2017Y K ShiIII1481Icotinib1372Cisplatin/pemetrexedEURTAC2012Rafael RosellIII861Erlotinib872Standard chemotherapyOPTIMAL2011Caicun ZhouIII821Erlotinib722Standard chemotherapyNEJ0022010A. InoueIII1141Gefitinib1142Standard chemotherapyWJTOG34052010Tetsuya MitsudomiIII861Gefitinib862Cisplatin plus docetaxelIPASS2009Tony S. MokIII6091Gefitinib6082Carboplatin and paclitaxelXu et al.2019Lisheng XuII901Icotinib plus pemetrexed and carboplatin892IcotinibStinchcombe et al.2019Thomas E StinchcombeII431Erlotinib plus bevacizumab452ErlotinibSWOGS14032020Sarah B. GoldbergII831Afatinib plus cetuximab852AfatinibLeighl et al.2017Natasha B. LeighlII441Erlotinib plus linsitinib442ErlotinibGOAL2020Rosario Garcia-CampeloII911Gefitinib and olaparib912GefitinibCortot et al.2021Alexis B CortotII591Afatinib plus cetuximab582AfatinibAGAIN2023Shintaro KandaIII2511Gefitinib/Osimertinib + Cisplatin and pemetrexed2512Gefitinib/OsimertinibFig. 1Flow diagram for the selection of eligible studiesFig. 2Network map comparing different treatment outcomes in different groups of patients with advanced epidermal growth factor receptor (EGFR) mutated non-small cell lung cancer (NSCLC) Each circular node represents a type of treatment. The node size is proportional to the total number of patients administering a treatment. Each line represents a type of head-to-head comparison. The width of lines is proportional to the total number of studies comparing the connected treatments. A. PFS of all patients, B. OS of all patients, C. PFS of EGFR 19del, D. PFS of EGFR L858R, E. PFS of man, F. PFS of woman, G. PFS of Asian, H. PFS of elderly. CT, Chemotherapy; SoC, standard of care
Evaluating heterogeneity/inconsistency and risk of bias
Risk of bias for the included RCTs exhibited that 4 presented with a high risk of bias, while 3 had a risk that was unclear, and the other exhibited a low risk of bias (Fig. 3).Fig. 3. Summary of risk-of-bias analysis. A. Risk of bias graph, B. Risk of bias summary. Green represents a low risk of bias, yellow an unclear risk, and red a high
Heterogeneity analyses exhibited low to moderate heterogeneity in most cases, although high heterogeneity was exhibited in few instances, and a random-effects model was thus utilized for the purpose of conducting these analyses (Figure S2-S7).
The absence of significant inconsistency was noteworthy on the basis of outcomes of global inconsistency test (P > 0.05) (Figure S8, Figure S9). As such, these analyses were performed using a consistency model.
NMA of PFS and OS in all cases
Relative to osimertinib (HR, 0.70, 95% CI, 0.58–0.86) and befotertinib (HR, 0.65, 95% CI, 0.42–1.00.42.00), amivantamab + lazertinib was associated with improved PFS. EGFR-mutated advanced NSCLC cases treated with osimertinib + CT exhibited PFS significantly better than that of cases treated with aumolertinib (HR, 0.61, 95% CI, 0.40–0.93), furmonertinib (HR, 0.64, 95% CI, 0.41–0.98), lazertinib (HR, 0.64, 95% CI, 0.41–0.98), osimertinib (HR, 0.62, 95% CI, 0.48–0.80), osimertinib + bevacizumab (HR, 0.72, 95% CI, 0.51–1.00.51.00), befotertinib (HR, 0.57, 95% CI, 0.36–0.90), and zorifertinib (HR, 0.61, 95% CI, 0.39–0.93). The absence of differences particularly in PFS was noteworthy when comparing osimertinib, aumolertinib, furmonertinib, befotertinib, lazertinib, zorifertinib, and osimertinib + bevacizumab (Fig. 4 A).Fig. 4. Pooled estimates of the network meta-analysis were based on the general population and different EGFR mutation subtypes A. Pooled hazard ratios (95% credible intervals(CI)) for PFS in all patients; B. Pooled hazard ratios (95% CI) for OS in all patients; C. Pooled hazard ratios (95% CI) for PFS in patients with EGFR 19del; D. Pooled hazard ratios (95% CI) for PFS in patients with EGFR 21 L858R. Afa, Afatinib; Afa + Bev, Afatinib + bevacizumab; Afa + Cet, Afatinib + cetuximab; Ami + Laz, Amivantamab + lazertinib; Aum, Aumolertinib; Bef, Befotertinib; CT, Chemotherapy; Dac, Dacomitinib; Erl + Bev, Erlotinib + bevacizumab; Erl + Lin, Erlotinib + linsitinib; Erl + Ram, Erlotinib + ramucirumab; Fum, Furmonertinib; Gef + Apa, Gefitinib + apatinib; Gef + CT, Gefitinib + chemotherapy; Gef + Ola Gefitinib + olaparib; Ico + CT, Icotinib + chemotherapy; Laz, Lazertinib; Osi, Osimertinib; Osi + Bev, Osimertinib + bevacizumab; Osi + CT, Osimertinib + chemotherapy; SoC, Standard of care (gefitinib, erlotinib, icotinib); Zor, Zorifertinib
Osimertinib (HR, 0.54, 95% CI, 0.32–0.90) and osimertinib + CT (HR, 0.48, 95% CI, 0.26–0.88) exhibited correlation with significant improvements in the OS of advanced EGFR-mutated NSCLC cases relative to befotertinib. Amivantamab + lazertinib was linked to significantly greater OS relative to furmonertinib (HR, 0.54, 95% CI, 0.30–0.95) and befotertinib (HR, 0.43, 95% CI, 0.24–0.77). The absence of differences particularly in OS was noteworthy when comparing the osimertinib, osimertinib + bevacizumab, osimertinib + CT, lazertinib, and amivantamab + lazertinib regmines (Fig. 4B).
NMA of PFS of EGFR mutation subtype
Amivantamab + lazertinib significantly outperformed both lazertinib (HR, 0.60, 95% CI, 0.36–0.99) and osimertinib (HR, 0.66, 95% CI, 0.51–0.89) with respect to its ability to prolong NSCLC cases’ PFS with EGFR 19del mutations. An extension of PFS was recorded in the osimertinib + CT group relative to the lazertinib (HR, 0.55, 95% CI, 0.33–0.95), osimertinib (HR, 0.61, 95% CI, 0.44–0.83), gefitinib + CT (HR, 0.50, 95% CI, 0.32–0.79), icotinib + CT(HR, 0.38, 95% CI, 0.21–0.71), and erlotinib + bevacizumab (HR, 0.43, 95% CI, 0.27–0.69) groups. However, the absence of differences particularly in PFS was noteworthy among EGFR 19del cases when comparing the aumolertinib, furmonertinib, befotertinib, lazertinib, osimertinib, and osimertinib + bevacizumab regimens (Fig. 4 C).
Osimertinib + CT provided EGFR L858R NSCLC cases with significantly extended PFS relative to osimertinib (HR, 0.63, 95% CI, 0.44–0.90), aumolertinib (HR, 0.54, 95% CI, 0.29–1.00.29.00), dacomitinib (HR, 0.51, 95% CI, 0.28–0.93), erlotinib + bevacizumab (HR, 0.54, 95% CI, 0.31–0.94), erlotinib + ramucirumab (HR, 0.52, 95% CI, 0.29–0.93), and gefitinib + apatinib (HR, 0.44, 95% CI, 0.23–0.83). The absence of differences particularly in PFS was noteworthy when comparing the aumolertinib, befotertinib, dacomitinib, furmonertinib, lazertinib, osimertinib, osimertinib + bevacizumab, amivantamab + lazertinib, erlotinib + bevacizumab, gefitinib + CT, and icotinib + CT regimens (Fig. 4D).
NMA of PFS in different gender subgroups
Among males, furmonertinib (HR, 0.54, 95% CI, 0.31–0.96) and osimertinib + CT (HR, 0.43, 95% CI, 0.23–0.80) exhibited correlation with significantly extended PFS relative to dacomitinib. The amivantamab + lazertinib (HR, 0.73, 95% CI, 0.55–0.98) and osimertinib + CT (HR, 0.53, 95% CI, 0.37–0.77) groups exhibited PFS significantly longer than that for the osimertinib group. Significantly better PFS was also observed in the osimertinib + CT group relative to the erlotinib + bevacizumab (HR, 0.56, 95% CI, 0.31–1.00.31.00), gefitinib + apatinib (HR, 0.44, 95% CI, 0.23–0.86), and gefitinib + CT (HR, 0.56, 95% CI, 0.32–0.99) groups. The absence of differences particularly in PFS extension yielded by the aumolertinib, befotertinib, furmonertinib, lazertinib, osimertinib, and osimertinib + bevacizumab regimens was noteworthy for male cases, but there was a trend toward superiority of furmonertinib over the other interventions (Fig. 5 A).Fig. 5. Pooled estimates for the network meta-analysis were based on gender, race, and age A. Pooled hazard ratios (95% CI) for PFS in man patients; B. Pooled hazard ratios (95% CI) for PFS in woman patients; C. Pooled odds ratios (95% CI) for Asian patients; D. Pooled odds ratios (95% CI) for elderly patients
Amivantamab + lazertinib significantly outperformed dacomitinib (HR, 0.56, 95% CI, 0.35–0.99), erlotinib + bevacizumab (HR, 0.43, 95% CI, 0.30–0.71), furmonertinib (HR, 0.56, 95% CI, 0.33–0.94), gefitinib + CT(HR, 0.55, 95% CI, 0.36–0.84), icotinib + CT (HR, 0.41, 95% CI, 0.23–0.71), and osimertinib (HR, 0.71, 95% CI, 0.55–0.91) with respect to the PFS outcomes for female cases. Significantly better PFS was observed in both the aumolertinib and osimertinib groups relative to the erlotinib + bevacizumab (aum: HR, 0.64, 95% CI, 0.42–0.96; osi: HR, 0.66, 95% CI, 0.46–0.93) and icotinib + CT (aum: HR, 0.56, 95% CI, 0.33–0.96; osi: HR, 0.58, 95% CI, 0.35–0.95) groups. Osimertinib + CT treatment yielded significantly better improvements in patient PFS relative to treatment with dacomitinib (HR, 0.53, 95% CI, 0.32–0.89), erlotinib + bevacizumab (HR, 0.44, 95% CI, 0.27–0.71), furmonertinib (HR, 0.53, 95% CI, 0.31–0.92), gefitinib + CT (HR, 0.52, 95% CI, 0.33–0.82), icotinib + CT (HR, 0.39, 95% CI, 0.22–0.70), lazertinib (HR, 0.59, 95% CI, 0.34–1.00.34.00), and osimertinib (HR, 0.67, 95% CI, 0.49–0.92)(Fig. 5B).
NMA of PFS is Asian and elderly patient subgroups
Treatment with erlotinib + bevacizumab (HR, 0.56, 95% CI, 0.32–0.99) and gefitinib + CT (HR, 0.50, 95% CI, 0.26–0.98) exhibited correlation with significantly better improvements in the PFS of Asian cases relative to SoC. The absence of differences particularly in PFS was noteworthy among the aumolertinib, afatinib, befotertinib, dacomitinib, lazertinib, furmonertinib, osimertinib, and zorifertinib regimens, although furmonertinib tended to outperform other treatments (Fig. 5 C).
Among elderly cases, icotinib + CT treatment was associated with significantly better improvements in patient PFS relative to afatinib (HR, 0.29, 95% CI, 0.15–0.58), afatinib + bevacizumab (HR, 0.15, 95% CI, 0.05–0.45), befotertinib (HR, 0.38, 95% CI, 0.16–0.88), dacomitinib (HR, 0.43, 95% CI, 0.21–0.86), furmonertinib (HR, 0.43, 95% CI, 0.20–0.93), and gefitinib + CT (HR, 0.50, 95% CI, 0.26–0.96). Relative to afatinib (HR, 0.33, 95% CI, 0.18–0.58), afatinib + bevacizumab (HR, 0.17, 95% CI, 0.06–0.47), befotertinib (HR, 0.42, 95% CI, 0.19–0.91), dacomitinib (HR, 0.47, 95% CI, 0.26–0.87), furmonertinib (HR, 0.48, 95% CI, 0.24–0.94), osimertinib (HR, 0.68, 95% CI, 0.47–0.98), and gefitinib + CT(HR, 0.56, 95% CI, 0.32–0.96), osimertinib + CT was associated with significantly better improvements in PFS among elderly cases. Significantly longer PFS was observed in the dacomitinib (HR, 0.35, 95% CI, 0.13–0.92), aumolertinib (HR, 0.28, 95% CI, 0.10–0.77), furmonertinib (HR, 0.35, 95% CI, 0.13–0.96), lazertinib (HR, 0.26, 95% CI, 0.10–0.69), and osimertinib (HR, 0.25, 95% CI, 0.09–0.64) groups relative to the afatinib + bevacizumab group (Fig. 5D).
NMA of OS of EGFR mutation subtype
The absence of differences particularly in OS extension was noteworthy among EGFR 19del cases with the exception of the significantly improved OS for cases in the afatinib group relative to those in the CT group (Figure S10A).
While there afatinib, afatinib + cetuximab, dacomitinib, erlotinib + bevacizumab, erlotinib + CT, osimertinib, and SoC did not differ significantly in their ability to improve the OS of EGFR L858R cases, dacomitinib tended to outperform other therapeutic modalities (Figure S10B).
NMA of OS in different gender subgroups
Among male cases, afatinib significantly outperformed CT (HR, 0.73, 95% CI, 0.55–0.97) with respect to its ability to improve OS. Relative to SoC (HR, 0.55, 95% CI, 0.36–0.83) and CT (HR, 0.53, 95% CI, 0.32–0.87), gefitinib + CT yielded significantly better OS (Figure S10C). Among female cases, dacomitinib was associated with significant improvements in OS relative to SoC, and it also tended to outperform other treatments (Figure S10D).
NMA of OS in Asian and elderly patient subgroups
In the Asian patient population, gefitinib + CT significantly outperformed afatinib (HR, 0.73, 95% CI, 0.53–0.97), befotertinib (HR, 0.58, 95% CI, 0.37–0.90), erlotinib + bevacizumab (HR, 0.74, 95% CI, 0.55–0.99), gefitinib + apatinib (HR, 0.62, 95% CI, 0.39–0.99), SoC (HR, 0.68, 95% CI, 0.55–0.84), and osimertinib (HR, 0.69, 95% CI, 0.49–0.97) as a menas of improving patient OS. The OS of cases in the dacomitinib treatment group was also significantly better than that of cases in the SoC group (HR, 0.76, 95% CI, 0.58–0.99) (Figure S10E).
Erlotinib + bevacizumab was associated with superior OS outcomes relative to CT in elderly cases and tended to outperform other therapeutic regimens (Figure S10F).
Efficacy rankings
With respect to PFS among the overall patient population, EGFR 19del cases, EGFR L858R cases, and women, osimertinib + CT yielded the best outcomes, followed by amivantamab + lazertinib. In the Asian population, amivantamab + lazertinib yielded the best outcomes, followed by osimertinib + CT. Among elderly cases, icotinib + CT yielded the best PFS outcomes, followed by osimertinib + CT (Figure S11).
With respect to OS among the overall patient cohort, amivantamab + lazertinib yielded the best outcomes, followed by osimertinib + CT treatment. Among EGFR 19del and male cases, the afatinib + cetuximab regimen yielded the best OS, while dacomitinib was associated with the best outcomes among EGFR L858R and female cases. Among Asian and elderly cases, gefitinib + CT and erlotinib + bevacizumab, respectively, exhibited correlation with the greatest OS outcomes (Figure S12).
Convergence and publication bias analyses
Good convergence was evident for all comparisons in the present NMA based on the established Brooks-Gelman-Rubin diagnostic plots (Figure S13, Figure S14) and trace plots (Figure S15-S20), and the symmetrical funnel plots were suggestive of no publication bias (Figure S21, Figure S22).
Discussion
Multiple EGFR-TKI therapeutic regimens have been designed to date and demonstrated to afford survival benefits to NSCLC cases whose tumors harbor EGFR mutations. Direct comparisons of these extant therapeutic modalities, however, are largely lacking, presenting clinicians with an immense challenge when seeking to select the best first-line regimen for use when treating a given patient. To address this issue, it was attempted to conduct the present investigation for comparable analysis of the efficacy of 24 different treatment strategies through an NMA approach, revealing that osimertinib + CT afforded the greatest benefits to the PFS of treated cases, although amivantamab + lazertinib may be associated with greater improvements in OS.
Within the encompassing cohort of EGFR-mutated NSCLC cases examined, the treatment regimens involving osimertinib + CT and amivantamab + lazertinib emerged as particularly beneficial, showcasing notable enhancements in both PFS and OS. Notably, the FLAURA study underscored the significant extension of OS and PFS in EGFR-mutated NSCLC cases with first-line osimertinib treatment [28]. This efficacy profile has led to the designation of osimertinib as the preferred therapeutic choice for cases with EGFR mutations according to the NCCN guidelines. Despite this, the persistent challenge of acquired resistance to EGFR-TKIs persists as a significant clinical concern. In response, there is ongoing exploration into combinatorial approaches involving these TKIs with other modalities to counteract this resistance phenomenon. Building on these findings, the FLAURA 2 study demonstrated that combining osimertinib and CT led to even greater improvements in patient outcomes relative to osimertinib alone, prolonging median patient PFS by approximately 9 months while lowering the risk of death or disease progression by 38% [12]. Amivantamab is a bispecific monoclonal antibody that binds to both EGFR and the c-MET receptor proteins on the cell surface, thereby blocking downstream signal transmission and inhibiting the proliferation of tumor cells expressing these proteins. The potent third-generation nervous system osmotic TKI lazertinib is capable of targeting EGFR-sensitive mutations and T790M mutations without impacting the activity of wild-type EGFR. In the phase III MARIPOSA trial, the amalgamation of amivantamab and lazertinib showcased a median PFS of 23.7 months, in stark contrast to the 16.6 months noted with osimertinib monotherapy [13]. Osimertinib and bevacizumab interact with a shared cascade of signaling pathways downstream from their targets. This synergy enables their combined application to effectively disrupt EGFR/VEGF signaling activity, potentially forestalling the onset of drug resistance and yielding superior antitumor efficacy [61, 62]. The latest results of a comprehensive NMA analysis have shown that osimertinib in combination with bevacizumab may be superior to other treatments regarding extension of PFS for cases with EGFR-mutated advanced NSCLC. In the present study, however, osimertinib + CT and amivantamab + lazertinib yielded greater improvements in the PFS an OS of cases relative to the combination of osimertinib + bevacizumab. These high-level findings, however, warrant more granular examination. If amivantamab + lazertinib is applied as a first-line treatment, for instance, the utilization of the MARIPOSA-2 protocols (amivantamab + CT ± lazertinib) would be inappropriate following patient relapse. As an alternative, the approved osimertinib + CT may be selected as the first-line approach, with combination amivantamab treatment being explored as a second-line option.
Several trials to date have shown that EGFR-TKI efficacy varies as a function of the subtype of EGFR mutation present in the target tumor, with cases harboring 19del mutations attaining greater benefits from TKI treatment relative to 21L858R cases [63–65]. While some past studies have compared the most effective first-line treatments for advanced NSCLC cases with these two types of EGFR driver mutations [66, 67], the emergence of more recent data from several major RCTs has largely rendered these earlier findings obsolete. The present NMA indicated that osimertinib + CT and amivantamab + lazertinib are still the best first-line option to improve the PFS of cases harboring either EGFR 19del or L858R mutations, in line with what was observed in the overall study population. Moreover, single-agent third-generation TKI treatment was associated with a promising PFS benefit among 19del cases, whereas combination therapy yielded better survival outcomes for L858R cases. This may be related to the more aggressive growth of 21L858R tumors, which also exhibit higher co-mutation rates and worse TKI affinity [68–70]. Notably, however, 19del cases were found to benefit to a greater extent from osimertinib + bevacizumab treatment relative to the 21 L858R cases. This raises the possibility that combination chemotherapy is superior to combined anti-angiogenic treatment as a TKI combination strategy for L858R cases. The mechanistic basis for this finding, however, remains uncertain, underscoring an important avenue for further research.
A growing wealth of evidence suggests that particular clinicopathological characteristics including sex, age, and ethnicity can all shape treatment outcomes and patient prognosis such that these factors should be considered when selecting the best therapeutic modalities for these individuals. The results of this NMA revealed that osimertinib + CT yielded the greatest improvements in PFS among both male and female cases. However, males attained greater benefits from furmonertinib relative to female cases. TKI combination therapies also tended to be the most highly ranked regimens for male cases, whereas single-agent TKI treatments tended to provide better outcomes for female cases. This may suggest that female cases exhibit greater TKI sensitivity relative to male cases, in line with past reports [71, 72]. Among Asian cases, the present analyses revealed that the two regimens associated with the greatest PFS benefits were the same as those for the overall patient population. However, Asian cases attained lower levels of benefit from osimertinib monotherapy relative to the overall study cohort. Furmonertinib and aumolertinib may therefore be better options for the single-agent TKI management of Asian cases. Icotinib + CT and osimertinib + CT yielded the greatest PFS benefits to elderly cases in this study, partially echoing past reports [67]. Osimertinib was also identified as the best alternative option for the treatment of elderly cases unable to tolerate combination therapy.
The limitations of the current investigation should be pointed out. Notably, the categorization of gefitinib, erlotinib, and icotinib into a single treatment group may introduce a potential bias. Nonetheless, it is essential to highlight that multiple studies have consistently shown similar safety and efficacy profiles across these first-generation TKIs [46, 66, 73, 74]. Secondly, this NMA was based only on available clinical trial data, but it is nonetheless susceptible to the effects of confounding factors. Third, this analysis could not analyze adverse effects in subgroups of cases according to particular clinicopathological characteristics, as these events primarily occurred in the general population rather than in patient subgroups. Fourth, while OS is regarded as the gold standard metric by which to analyze antitumor therapies, the OS data for some of the included clinical trials remains relatively immature such that this may have introduced some degree of heterogeneity into the results. As such, PFS was the primary outcome indicator evaluated in this study, underscoring an important avenue for future research. Fifth, this network meta-analysis has inherent limitations. The trials we included were mainly conducted at different times, and their molecular diagnostic methods were mostly PCR rather than the more comprehensive NGS. Therefore, we are unable to obtain detailed patient-level data on specific EGFR mutation subtypes (for example, uncommon exon 19 deletion mutations [75] that may vary in response to treatment) or molecular co-mutations (such as MET, TP53, etc.). The heterogeneity of these biological factors may significantly affect the treatment outcome [76, 77]. For instance, for the Amivantamab + Lazertinib combination regimen, existing evidence suggests that the patient population with high MET protein expression (IHC positive) may benefit more significantly [78], but our analysis cannot be conducted at this subdivision level. Future network meta-analyses of individual patient data or aggregated data studies targeting specific biomarker subgroups are crucial for revealing the relative efficacy of different treatment regimens in subgroups with more precisely defined molecules.
Conclusions
This NMA demonstrates that the optimal first-line treatment for advanced EGFR-mutated NSCLC may vary based on specific clinicopathological characteristics. The key findings can be summarized as follows:
- Broadly superior regimens: Osimertinib plus CT and amivantamab plus lazertinib emerged as the most notable regimens, demonstrating superior PFS and OS benefits, respectively, in the overall population.
- PFS benefits: Osimertinib plus CT consistently showed the greatest PFS benefit across different genders and EGFR mutation subtypes.
- OS benefits based on subgroups: The greatest OS benefits were associated with:
- 19del mutations and male patients: Afatinib + cetuximab.
- L858R mutations and female patients: Dacomitinib.
- Asian patients: Gefitinib + CT.
- Elderly patients: Erlotinib + bevacizumab.
These findings underscore the potential for personalized first-line treatment strategies.
Supplementary Information
Supplementary Material 1: Table S1. PRISMA extension checklist for this network meta-analysis. Table S2. Search strategy. Figure S1. Network map comparing different treatment outcomes in different groups. Figure S2-S7. Heterogeneity analysis. Figure S8, S9. Inconsistency analysis. Figure S10. Pooled estimates of the network meta-analysis. Figure S11, S12. Ranking diagram for network meta-analysis. Figure S13, S14. Brooks-Gelman-Rubin diagnostic plots for evaluating model convergence. Figure S15-S20. Trace plot for evaluating model convergence. Figure S21, S22. Funnel plot for evaluating publication bias.
Supplementary Material 2.
Supplementary Material 3.
Supplementary Material 4.
Supplementary Material 5.
Supplementary Material 6.
Supplementary Material 7.
Supplementary Material 8.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pinto JA, Vallejos CS, Raez LE, et al. Gender and outcomes in non-small cell lung cancer: an old prognostic variable comes back for targeted therapy and immunotherapy? ESMO Open. 2018/01/01/ 2018;3(3):e 000344. 10.1136/esmoopen-2018-000344.10.1136/esmoopen-2018-000344 PMC 590584029682332 · doi ↗ · pubmed ↗
- 2Yang F, Zhang W, Shang X, et al. Comparison of the efficacy and safety of first-line treatments based on clinicopathological characteristics for patients with advanced epidermal growth factor receptor mutated non-small-cell lung cancer: A systematic review and network meta-analysis. Critical Reviews in Oncology/Hematology. 2022/09/01/2022;177:103760. 10.1016/j.critrevonc.2022.103760.10.1016/j.critrevonc.2022.10376035870763 · doi ↗ · pubmed ↗