Automated reporting of primaquine dose efficacy, tolerability and safety for Plasmodium vivax malaria using a systematic review and individual patient data meta-analysis
Peta Edler, Megha Rajasekhar, David J. Price, Ishag Adam, Ghulam Rahim Awab, Bridget E. Barber, Larissa W. Brasil, Nathália N. Chamma-Siqueira, Cindy S. Chu, Liwang Cui, André Daher, Margarete do Socorro M. Gomes, Lilia Gonzalez-Ceron, Matthew J. Grigg, Harin Karunajeewa

TL;DR
This paper presents automated reports on the effectiveness and safety of primaquine doses for treating P. vivax malaria, using data from 41 studies to help guide treatment policies.
Contribution
The study introduces an automated reporting system using a large database and R Shiny app to analyze primaquine dose effects in different regions.
Findings
9,270 patient records from 41 studies were pooled into a standardized database.
Automated reports provide region-specific insights into primaquine efficacy and safety.
The system supports policy decisions by analyzing dose effects on relapse, haemolysis, and tolerability.
Abstract
The antirelapse efficacy of primaquine is related to the total dose administered, whereas the risks of haemolysis and gastrointestinal intolerance are associated with the daily dose administered. National Malaria Control Programmes require local information on efficacy, tolerability and safety to optimize antimalarial treatment policies for Plasmodium vivax malaria control and elimination efforts. A living systematic review identified efficacy studies of uncomplicated P. vivax malaria including patients treated with daily primaquine regimens, published since January 1, 2000. Available data were pooled and an R Shiny app was developed to integrate statistical analyses performed using R and Stata that assessed the impact of primaquine mg/kg dose on efficacy, hematological safety and gastrointestinal tolerability. As of January 16, 2025, a total of 9,270 individual patient data records…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
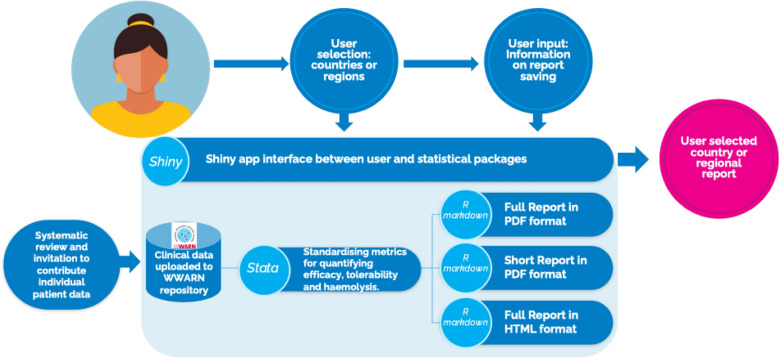 Figure 1
Figure 1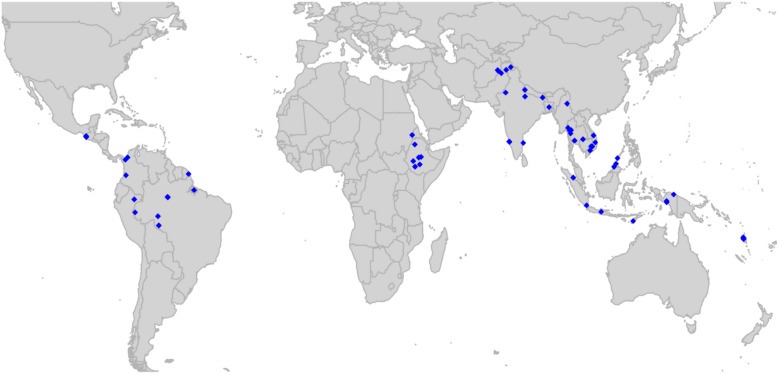 Figure 2
Figure 2- —https://doi.org/10.13039/501100000925National Health and Medical Research Council
- —https://doi.org/10.13039/100010269Wellcome Trust
- —https://doi.org/10.13039/501100003593Conselho Nacional de Desenvolvimento Científico e Tecnológico
- —https://doi.org/10.13039/100000865Bill and Melinda Gates Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Mosquito-borne diseases and control · vaccines and immunoinformatics approaches
Background
Efforts to reduce malaria transmission in countries co-endemic for Plasmodium falciparum and Plasmodium vivax have been much more successful for P. falciparum [1]. P. vivax forms dormant liver stages (hypnozoites) that cause relapsing infections, contributing to 66–90% of all recurrent episodes of vivax malaria, sustaining ongoing transmission and hampering P. vivax elimination [2, 3]. Killing hypnozoites requires treatment with an 8-aminoquinoline drug, of which primaquine is the most widely available. The antirelapse efficacy of primaquine is related to the total dose administered, however, in practice a major barrier to its use are concerns of haemolysis in individuals with glucose-6-phosphate dehydrogenase (G6PD) deficiency, which is related to the daily dose administered [4, 5]. Single-dose tafenoquine has been recently recommended by the World Health Organization (WHO) for use in South America [6], however, to date, concerns about its optimal dose [7] and its use in combination with artemisinin-based combination therapy [8] have slowed widespread implementation.
Primaquine doses are generally given as 3.5 mg/kg (low) or 7 mg/kg (high) total dose regimens over 7 or 14 days, equating to 0.25 mg/kg (low), 0.5 mg/kg (intermediate) or 1 mg/kg (high) per day. Previous guidelines recommend low total dose primaquine regimens (3.5 mg/kg over 7 or 14 days), which were considered to provide sufficient efficacy in most vivax-endemic settings since higher daily doses are associated with an increased risk of haemolysis and gastrointestinal intolerability [9]. However, comparative data informing these guidelines have been sparse. Recent individual patient data meta-analyses undertaken by the WorldWide Antimalarial Resistance Network (WWARN) have used data from 23 studies conducted in 16 vivax-endemic countries across the Americas, Africa, and the Asia–Pacific [10, 11], and demonstrated that increasing the total dose of primaquine from 3.5 to 7 mg/kg could potentially reduce the risk of vivax recurrence within 180 days by approximately 50% [10]. High total dose primaquine requires higher daily mg/kg dosing, but patients treated with primaquine doses of up to 0.5 mg/kg/day had a minimal increase in gastrointestinal intolerance with no increased risk of severe hemolysis in individuals with ≥ 30% G6PD activity [10, 11].
National Malaria Control Programmes (NMCPs) have highlighted the importance of regional and subregional data on primaquine efficacy and safety, since these may differ from the global pooled results. NMCPs have requested these data to inform decisions regarding national antimalarial policies [12]. To assist regional and national policy makers to access these data, we developed open access, automated local and regional reports using a single standardized data repository. This manuscript aims to describe the automated process of generating these reports and highlight their role for policy makers.
Methods
Studies were identified as part of an existing living systematic review of efficacy studies of uncomplicated P. vivax published since January 1, 2000 in any language. All studies included treatment with a daily primaquine regimen which was commenced within 7 days of schizontocidal treatment and had a minimum follow up duration of 28 days [10, 11, 13]. Investigators of eligible studies were approached to share individual patient data. Pseudo-anonymized data were shared to the WWARN repository, standardized and pooled into a single database according to an a priori statistical analysis plan. Patients were excluded from the analysis if they presented with severe malaria, received adjunctive antimalarials within 14 days of commencing treatment, received an alternative hypnozoiticidal agent to primaquine, received primaquine 7 or more days after commencing their schizontocidal treatment, had a protocol violation in the original study, or were missing age, sex or primaquine dose.
Efficacy analyses assessed the total dose of primaquine, and tolerability and safety analyses assessed the daily dose of primaquine. The total dose of primaquine regimens was categorized into two bands: low (2– < 5 mg/kg total dose) and high dose (≥ 5 mg/kg total dose), reflecting standard 3.5 mg/kg and 7 mg/kg total dose regimens. Patients with doses < 2 mg/kg were excluded from the efficacy analyses. Daily primaquine dose was categorized into three bands: low (< 0.375 mg/kg/day), intermediate (0.375– < 0.75 mg/kg/day) and high dose (≥ 0.75 mg/kg/day), reflecting standard 0.25 mg/kg, 0.5 mg/kg and 1 mg/kg daily dose regimens.
The statistical software packages R and Stata and the notebook interface R Markdown were used to generate reports on the effects of primaquine mg/kg dosing on efficacy, haematological safety and gastrointestinal tolerability. An R Shiny app was developed to integrate the statistical packages and provide a user interface to generate open-access, user-selected, country or regional automated reports in a variety of formats (Fig. 1).Fig. 1. Generation of region and country automated reports on primaquine efficacy and safety
The statistical analyses for the reports were based on a priori statistical analysis plans developed from the previous meta-analyses [10, 11], in which data could be filtered by country or region, based on the user selection in the R Shiny app. For each model, simple checks were undertaken, to ensure availability of reference data, that confidence intervals were logical, and that models converged (as detailed below).
Kaplan–Meier survival analysis was used to calculate the risk of recurrence between day 7 and day 365 after starting primaquine treatment. Patients were left-censored on day 7 and right-censored on the day last reviewed, the last day before a > 60-day gap in blood smears, or the day of non-P. vivax parasitemia. The rate of vivax recurrence between day 7 and 180 in patients following low and high total dose primaquine compared with treatment without primaquine were estimated using Cox regression models adjusting for sex, age and baseline parasitemia, with shared frailty for study site. Each site within a study was considered to be a separate study site. Additional Cox models investigated the rate of vivax recurrence following 14-day primaquine treatment compared with 7-day treatment in patients with low or high total dose primaquine.
Patients were excluded from the tolerability analyses if they did not have symptom questionnaire data on tolerability, they received primaquine more than 7 days after commencing their schizontocidal treatment or they did not have data on daily primaquine dose. Gastrointestinal intolerance on days 5–7 was assessed according to the daily primaquine dose category using a logistic mixed-effects model, adjusting for age, sex and baseline parasite density, with a random effect for study site. Days 5–7 were chosen to avoid confounding from symptoms relating to schizontocidal treatment or acute malaria.
Patients were excluded from the hematological safety analyses if they did not have data on hemoglobin at day 0 and at least one follow up day, they received primaquine more than 7 days after commencing their schizontocidal treatment, they did not have data on daily primaquine dose and had unknown or < 30% G6PD activity. Linear mixed-effects regression was used to assess the absolute change in hemoglobin from day 0 to day 2–3 for each daily primaquine dose category, adjusting for hemoglobin on day 0, age, sex and baseline parasite density, with a random effect for study site. Day 2–3 was chosen as this is the time of expected hemoglobin nadir and when the majority of patients will be tested.
Results
Of 108 eligible studies, 40 have been shared to the standardized repository, in addition to two unpublished studies. As of January 16, 2025, a total of 9,270 patients from 41 studies [14–53] have undergone curation and are available for inclusion in the analyses (Additional file 1: Fig. S1, Tables S1-2). There are 6346 (68.5%) patients from the Asia–Pacific, 1236 (13.3%) from Africa and 1,688 (18.2%) from the Americas (Fig. 2). In total, 1582 (17.1%) patients were treated without primaquine, 66 (0.7%) with very low total dose primaquine (< 2 mg/kg; these participants were excluded from efficacy analyses), 4282 (46.2%) with low total dose primaquine (2– < 5 mg/kg) and 3340 (36.0%) with high total dose primaquine (≥ 5 m g/kg). Data are currently available for 7508 patients from 27 studies for efficacy analyses, 5772 patients from 17 studies for tolerability analyses and 5,710 patients from 19 studies for hematological safety analyses.Fig. 2. Map of study sites from which data were available for automated reports as of January 16, 2025
The R Shiny app can generate R Markdown reports for three global regions (Africa, the Americas and Asia–Pacific) or any combinations of countries. The current country reports are grouped into 8 subregional groupings based on geographic location and study size. Reports can be generated as either a detailed or summary version, both of which can be provided in an html and pdf format to aid with accessibility (Fig. 1). The reports were updated following feedback from NMCPs through the Asia–Pacific Malaria Elimination Network. To ensure ease of access for users, privacy of data and accuracy of results, reports generated through the R Shiny app have been reviewed by authors and made openly accessible through the WorldWide Antimalarial Resistance Network. Reports are available for review and download at https://www.iddo.org/wwarn/vivax-reports.
The living systematic review will be updated every 6 months for the next five years, with studies eligible for the primaquine database to be identified. If available, data will be pooled into the standardized database and updated reports will be generated. This ongoing process has subsequently identified investigators from the 13 eligible studies published since the original database collation on August 23, 2021, who have been approached to share data; 3 of whom have provided data, and 2 others who have agreed to share data.
Discussion
Automated reports for 17 countries and three global regions have been generated to define the effect of primaquine dose in patients with uncomplicated P. vivax malaria on efficacy, tolerability and safety; these are openly available using an existing global database of primaquine efficacy clinical trials. The WWARN global individual patient database will be updated twice yearly to provide countries and regions with up-to-date reports on efficacy and safety of primaquine as countries progress towards malaria elimination.
Plasmodium vivax strains differ between geographic regions with substantial heterogeneity in transmission, relapse phenotype, hypnozoite load and primaquine efficacy. For instance, regions such as Papua, Indonesia and Papua New Guinea have the rapidly relapsing variant (3–4 weeks between relapses), whereas relapses in South Asia generally occur 8–9 months after the initial infection [54]. In some areas, high antirelapse efficacy is achieved with relatively low total doses (3.5 mg/kg) of primaquine [21] whereas in other areas a higher total dose is required [10]. The availability of the automated reports using local data from countries and regions will guide policymakers to optimize primaquine dosing for vivax radical cure in their local context. As single-dose tafenoquine is implemented into national policies, there will be an opportunity to integrate efficacy, tolerability and safety data from tafenoquine efficacy studies into the automated reports and allow comparison with primaquine regimens.
Reports are limited by inclusion of only a subset of published data. Of the potentially eligible studies, 66 (61%) were unavailable for analysis, with most (48/66; 73%) published more than 10 years ago. Timely access to clinical data is critical for ensuring that reports are contemporary, and yet time lags between completion of trials and access and curation of data are an issue to overcome; only one of the 12 studies published since 2023 is available for the current reports. All investigators of these trials have been approached and two have agreed to share their data. One investigator has recently shared their data, which, along with data from an additional older study, will be added to the database in the coming months.
The methodology of trials assessing the antirelapse efficacy of 8-aminoquinolines is heterogeneous. Differences in the duration of follow up and inability to distinguish accurately between relapses, new infections and recrudescences, have hampered comparisons between trials, although new methods to distinguish recurrences have been developed [55, 56]. Similarly, there are a lack of standardized metrics to assess safety following 8-aminoquinoline treatment. The definition of hemolytic adverse events attributable to 8-aminoquinolines varies substantially between studies, and this can result in over- or under-estimation of the safety of 8-aminoquinolines. Defining severe drug-induced hemolysis attributable to 8-aminoquinolines is further complicated by associated parasite-induced hemolysis and the fall in hemoglobin being strongly correlated to the baseline hemoglobin concentration [57]. These automated reports provide standardized definitions for relapse efficacy and safety, ensuring results can be compared between trials and between geographic locations.
Automation of reports provide consistent safety and efficacy metrics across different study designs, and this will reduce the time to review and compare outputs from different studies. However, these reports are not formal analyses and therefore may lack detailed assessment of limitations that could potentially lead to misinterpretation. Users should be aware that there can be substantial variations in reporting of gastrointestinal symptoms [58] and that comparisons of non-randomized study arms may lead to unexpected findings. Administration of primaquine with food has been demonstrated to greatly reduce the risk of gastrointestinal symptoms [59]. The risk of bias assessments that are now routinely included in formal individual patient data meta-analyses have not been incorporated into the automated reports. Furthermore, users need to be aware of the potential for bias with efficacy studies with smaller sample sizes and consider these automated reports in the context of more formal published individual patient data meta-analyses [10, 11]. Although reports have been designed to automate analyses of data from published efficacy studies, they could also incorporate and analyse shared data from unpublished therapeutic efficacy studies conducted either by NMCPs or researchers, facilitating formal analysis and reporting. Queries about reports are available through a contact email at https://www.iddo.org/wwarn/vivax-reports.
Recent global evidence on primaquine mg/kg dosing suggests that higher total primaquine doses will lead to substantial reductions in P. vivax relapses across most endemic regions [6, 10]. The availability of national and regional reports describing the effect of primaquine mg/kg dose for uncomplicated P. vivax on efficacy and safety provides NMCPs with the opportunity to consider these global implications together with data from their local regions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maguire JD, Krisin, Marwoto H, Richie TL, Fryauff DJ, Baird JK. Mefloquine is highly efficacious against chloroquine-resistant Plasmodium vivax malaria and Plasmodium falciparum malaria in Papua, Indonesia. Clin Infect Dis. 2006;42:1067–72.10.1086/50135716575721 · doi ↗ · pubmed ↗
- 2Daher A, Pereira D, Lacerda MVG, Alexandre MAA, Nascimento CT, Alves de Lima ESJC, et al. Efficacy and safety of artemisinin-based combination therapy and chloroquine with concomitant primaquine to treat Plasmodium vivax malaria in Brazil: an open label randomized clinical trial. Malar J. 2018;17:45.10.1186/s 12936-018-2192-x PMC 578237429361939 · doi ↗ · pubmed ↗