Cryoglobulinemic Vasculitis Manifesting as Rapidly Progressive Glomerulonephritis: A Case Report
Sritharan Thivacaren, Mihiran Thanigasalan, Anura Hewageegana, Mohamed Nazar Abdul Latiff, Priyani Amarathunga

TL;DR
A 35-year-old man with rapidly worsening kidney disease was found to have a rare immune-related condition called cryoglobulinemic vasculitis, which was successfully treated with plasma exchange and immunosuppressive drugs.
Contribution
This case report highlights the rare association between monoclonal gammopathy of renal significance and mixed cryoglobulinemia presenting as rapidly progressive glomerulonephritis.
Findings
Renal biopsy confirmed cryoglobulin deposits and a membranoproliferative pattern in a patient with rapidly progressive glomerulonephritis.
Treatment with plasma exchange and immunosuppressive therapy led to significant improvement in renal function and proteinuria.
The case emphasizes the importance of early diagnosis and treatment to prevent irreversible kidney damage in cryoglobulinemic vasculitis.
Abstract
Cryoglobulinemic vasculitis is a small- to medium-vessel vasculitis involving the skin, joints, peripheral nerves, and kidneys, due to deposition of immune complexes containing cryoglobulins. Cryoglobulins are immunoglobulins that precipitate below 37°C and are classified into three types: type I (monoclonal) and types II and III (mixed). We report a rare case of mixed cryoglobulinemia associated with monoclonal gammopathy of renal significance (MGRS) presenting as rapidly progressive glomerulonephritis (RPGN). A 35-year-old man presented with generalized edema, frothy urine, microscopic hematuria, and lower limb numbness for three weeks. Laboratory evaluation revealed elevated serum creatinine (8.5 mg/dL), markedly reduced C4 complement (0.5 mg/dL), positive rheumatoid factor, and an IgM monoclonal band on immunofixation. Bone marrow biopsy showed no abnormal plasma cell proliferation.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
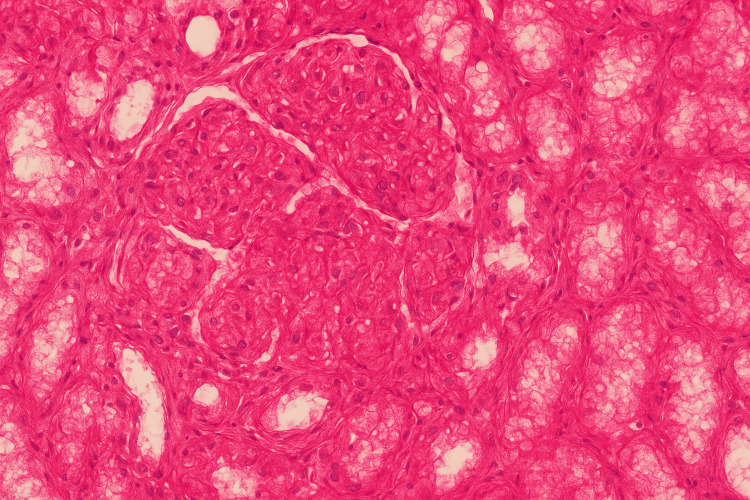 Figure 1
Figure 1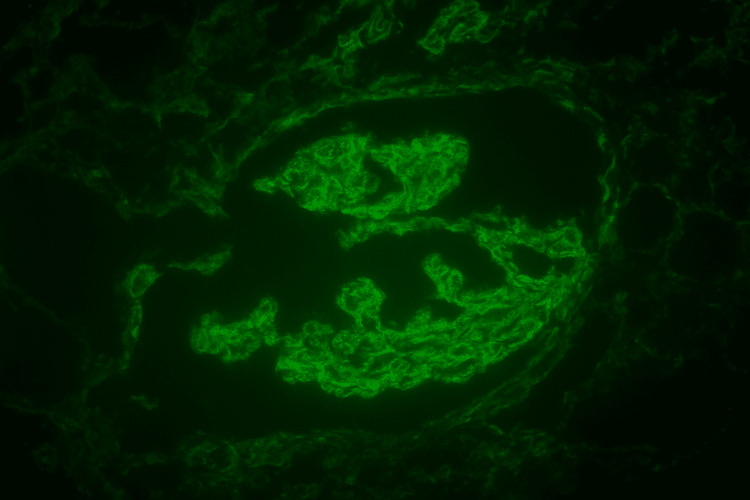 Figure 2
Figure 2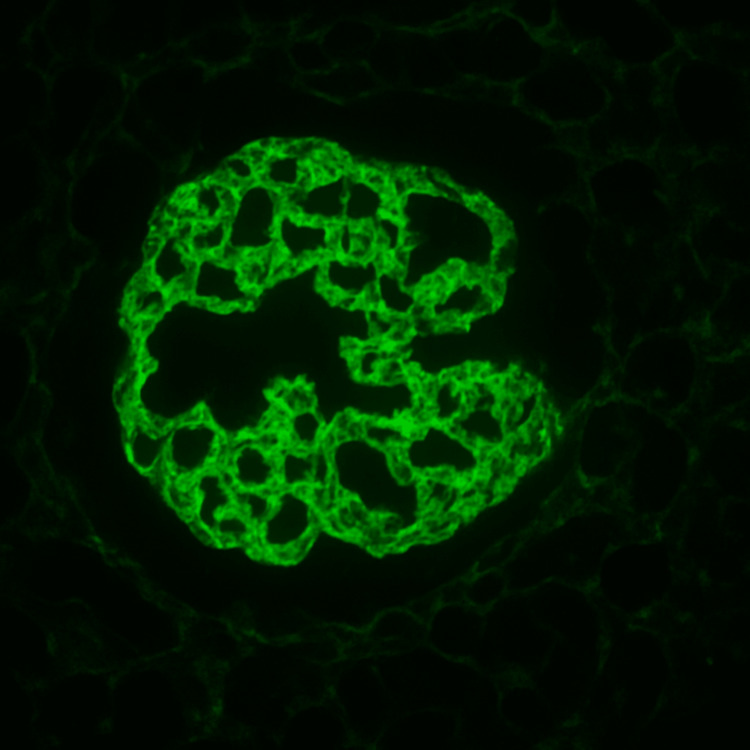 Figure 3
Figure 3| On admission | After treatment | Normal values | |
| Full blood count | |||
| White blood cells (109/L) | 7.97 | 8.7 | 4.0 – 10.0 (109/L) |
| Neutrophils (109/L) | 7.31 | 8.1 | 2.0 - 7.0 (109/L) |
| Lymphocytes (109/L) | 0.24 | 0.45 | 0.8 - 4.0 (109/L) |
| Hemoglobin (g/dL) | 12.2 | 9.0 | 11.0- 16.0 ( g/dL) |
| Platelets (109/L) | 191000 | 400000 | 150 – 450 (109/L) |
| Erythrocyte sedimentation rate mm/hour | 15 | N/A | 0-15mm/hour |
| Lactate dehydrogenase U/L | 240 | N/A | 140-280 U/L |
| Serum Sodium (millimole/L) | 128 | 146 | 136 – 145 (millimole/L) |
| Serum Potassium (millimole/L) | 4.4 | 4.5 | 3.5 – 5.1 (millimole/L) |
| Serum Creatinine (mg/dL) | 8.5 | 0.97 | 0.8-1.2 (mg/dL) |
| Urine full report | |||
| Pus cells | 10-15/hpf | 2-4/hpf | 0-5/hpf |
| Red cells | 25-30/hpf | Occ/hpf | 0-2/hpf |
| Protein | +200mg/dl | +50mg/dl | Nil |
| Urine Protein: creatinine | 3.3 | 0.56 | < 0.2 |
| Total Protein (g/dL) | 4.5 | N/A | 6.4- 8.3 (g/dL) |
| Albumin (g/dL) | 2.8 | 3.7 | 3.5- 5.2 (g/dL) |
| Globulin (g/dL) | 1.7 | N/A | 2.2 – 4.0 (g/dL) |
| Serum protein electrophoresis | An abnormal monoclonal band present in the gamma region 0.6g/L | ||
| Serum Immune fixation | Monoclonal band seen is IgM kappa | ||
| Serum free light chains | |||
| Kappa/k light chain (mg/L) | 18.4 | N/A | 6.7-22.4 (mg/L) |
| Lambda light chain (mg/L) | 37.7 | N/A | 8.3- 27 (mg/L) |
| k/lambda ratio | 2.05 | N/A | 0.26 - 1.65 |
| Qualitative assay for Cryoglobulins | Positive | ||
| Immunological markers | |||
| Antinuclear antibody | Positive | N/A | Negative |
| Anti- double stranded deoxyribonucleic acid | Negative | N/A | Negative |
| C-Antineutrophil cytoplasmic antibody | Negative | N/A | Negative |
| P -Antineutrophil cytoplasmic antibody | Negative | N/A | Negative |
| Anti-streptolysin O titrer | 37.7IU/ml | N/A | less than 200 IU/ml |
| RO -52 antibody | Positive | N/A | Negative |
| Anti-Sjogren's syndrome related to antigen A | Negative | N/A | Negative |
| Anti-Sjogren's syndrome type B | Negative | N/A | Negative |
| C3 (mg/dL) | 55.2 | N/A | 80- 178 (mg/dL) |
| C4 (mg/dL) | 0.5 | N/A | 15-45 (mg/dL) |
| Rheumatoid factor (U/mL) | 58.4 (Positive) | N/A | less than 20 (U/mL) |
| Virology markers | |||
| Hepatitis B surface Antigen (HBsAg) | Non-reactive | N/A | Non- reactive |
| Hepatitis C Antigen – Antibody (HCV Ag-Ab) | Non-reactive | N/A | Non- reactive |
| Ultrasound Abdomen | Lt Kidney -11.7 Bilateral Kidneys show increase echogenicity with blurred corticomedullary demarcation. No Hydronephrosis or hydroureter and no organomegaly. | ||
| High resolution computed tomography chest | No significant abnormality in bilateral lungs | ||
| Skin biopsy | Leukocytoclastic vasculitis | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · IgG4-Related and Inflammatory Diseases · Hepatitis C virus research
Introduction
Cryoglobulinemia is a rare condition that predominantly affects females compared to males, and the typical age of onset ranges from 40 to 50 years [1]. It involves small to medium vessels in the skin, joints, nerves, and kidneys due to cryoglobulin-containing immune complexes. Cryoglobulins are immunoglobulins in the serum that precipitate at temperatures below 37°C [1]. They were classified into three groups. Type Ⅰ are monoclonal (typically IgM, less commonly IgG or IgA), whereas type Ⅱ and Ⅲ cryoglobulins are mixed. Type Ⅱ is characterized by a monoclonal IgM combined with polyclonal IgG, whereas type Ⅲ is polyclonal (1). Types Ⅱ and Ⅲ are associated with chronic infections and autoimmune diseases.
Isolated proteinuria and hematuria are the common renal manifestations of cryoglobulinemic vasculitis. Here, we present a case of mixed cryoglobulinemia associated with monoclonal gammopathy of renal significance manifested as rapidly progressive glomerulonephritis. It is a very rare kind of presentation.
Case presentation
A 35-year-old man presented with a three-week history of generalized body swelling and frothy urine. He also reported microscopic hematuria. In addition, he described pain and numbness affecting both lower limbs and the chest wall, associated with reduced urine output. Neuropathy predominantly involves the lower limbs. There was no history of fever, cough, photosensitive rash, oral ulcers, arthritis, dry eyes, or dry mouth. He denied any respiratory or gastrointestinal symptoms and had no history of Raynaud phenomenon. There was no history of renal disease, autoimmune illness, or malignancy. He was not on long-term medications and had no known allergies.
On examination, he was pale with bilateral pitting edema extending to the knees. There was no peripheral cyanosis, no retinal or oral lesions, and no lymphadenopathy. Cardiovascular, respiratory, and abdominal examinations were unremarkable. Neurological examination revealed symmetrical sensory and motor impairment in both lower limbs.
Key laboratory results are summarized in Table 1. On admission, his serum creatinine was 8.85 mg/dL (baseline 1.3 mg/dL), serum sodium 128 mmol/L, and serum albumin 2.8 g/dL. Urinalysis showed 25-30 red cells/high-power field (hpf), 10-15 pus cells/hpf, and proteinuria >200 mg/dL. The urine protein-creatinine ratio was 3.3.
Serum protein electrophoresis demonstrated an abnormal monoclonal band in the gamma region (0.6 g/L), which was identified on immunofixation as IgM kappa. Complement levels were markedly reduced (C3: 55.2 mg/dL; C4: 0.5 mg/dL). Antinuclear antibody was positive (titer 1:320) with negative anti-double-stranded DNA. Tests for hepatitis B surface antigen and hepatitis C antibody were non-reactive.
His renal biopsy revealed eosinophilic, deeply PAS-positive globules in capillary loops resembling cryoglobulin deposits along with membranoproliferative patterns but no crescents. (Figure 1). Immunofluorescence revealed predominant IgM and kappa (Figures 2, 3). His qualitative assay for cryoglobulins became positive. His bone marrow biopsy and contrast CT of the chest, abdomen, and pelvis were normal.
H and E stain into 40 describes a membranoproliferative pattern with eosinophilic globules within the capillary lumen.
Immunofluorescence staining of mesangium IgM 3+ staining.
Immunofluorescence staining of mesangium Kappa 3+.
Type II cryoglobulinemic vasculitis (mixed) was made as a possible diagnosis after extensive investigations. He was treated with five plasma exchanges, intravenous methylprednisolone 500 mg in three doses followed by oral prednisolone 40 mg, intravenous immunoglobulin 10 g after each cycle of plasma exchange, and intravenous rituximab 700 mg (375 mg/body surface area) in two doses two weeks apart. He underwent four hemodialysis treatments until the acute kidney injury was settled. He was discharged with mycophenolate mofetil and prednisolone. The follow-up visit showed significant improvement in proteinuria and renal function.
Discussion
Type II cryoglobulinaemia consists of mixed cryoglobulins made up of monoclonal IgM with rheumatoid factor (RF) activity complexed with polyclonal IgG [1]. The monoclonal IgM is produced by a small, indolent B-cell or lymphoplasmacytic clone. When such a clone causes kidney injury without meeting criteria for overt lymphoma or myeloma, the condition is classified as monoclonal gammopathy of renal significance (MGRS) [1].
Pathogenetically, cryoglobulins precipitate at subphysiologic temperatures and dissolve on warming [1]. In vivo, these immune complexes deposit in small- and medium-sized vessels, activate the classical complement pathway, and cause vasculitis with consumption of complement, particularly C4. IgM monoclonal gammopathy has a high level of autoantibody activity, facilitating the formation of immune complexes, causing type II cryoglobulinemia [1].
Renal pathology most often reveals a membranoproliferative glomerulonephritis (MPGN) pattern [2] characterized by mesangial and endocapillary hypercellularity, double-contour GBM from mesangial interposition, and PAS-positive hyaline thrombi within glomerular capillaries representing precipitated cryoglobulin [2]. Immunofluorescence typically shows bright staining for monoclonal IgM (light-chain restricted, κ or λ) together with polyclonal IgG and strong C3 deposition in mesangial and capillary wall distributions. Electron microscopy often demonstrates large subendothelial electron-dense deposits with an organized microtubular or fingerprint substructure [2].
Clinical presentation can range from asymptomatic microscopic hematuria and mild proteinuria to nephrotic syndrome, chronic kidney disease, or rapidly progressive glomerulonephritis (RPGN) with crescent formation [3]. The differential diagnosis includes lupus nephritis, ANCA-associated vasculitis, and anti-GBM disease, making renal biopsy essential for definitive diagnosis.
Globally, chronic hepatitis C virus (HCV) infection is the most common cause [4]. It drives B-cell clonal expansion and monoclonal IgM production [5]. In HCV-negative cases, low-grade B-cell lymphomas, lymphoplasmacytic lymphoma, or monoclonal B-cell lymphocytosis are frequent underlying disorders.
Management aims to eliminate the pathogenic clone and control immune complex-mediated injury.
A) Clone-directed therapy: Rituximab is first-line for most B-cell clones, with or without alkylating agents (e.g., cyclophosphamide, bendamustine), depending on disease aggressiveness [6]. B) Immunosuppression: High-dose corticosteroids for rapid inflammation control, tapered as clone-directed therapy becomes effective. C) Plasmapheresis: Considered in severe, rapidly progressive, or multisystem involvement to promptly reduce circulating cryoglobulins. D) HCV-positive cases: Direct-acting antivirals in addition to immunomodulatory therapy when active vasculitis is present [7].
Conclusions
This case highlights the importance of considering cryoglobulinemic vasculitis in the differential diagnosis of rapidly progressive glomerulonephritis and emphasizes the need for early recognition, prompting immunosuppressive therapy to prevent irreversible renal damage and improve outcome. Prognosis is determined by baseline kidney function, chronicity of histological injury, and timeliness of effective clone control.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A case of renal damage induced by cryoglobulinemia associated with monoclonal gammopathy of renal significance BMC Nephrol Zhang Y Meng X Wang J 410262025 https://bmcnephrol.biomedcentral.com/articles/10.1186/s 12882-025-04330-w 4069156110.1186/s 12882-025-04330-w PMC 12281695 · doi ↗ · pubmed ↗
- 2Mixed cryoglobulinemia; a rare presentation of Waldenström macroglobulinemia J Nephropathol Ribeiro CI Santos C Almeida C 15957132020 https://nephropathol.com/Article/jnp-15957
- 3Renal-limited cryoglobulinemic vasculitis: two case reports Intern Med Toriu N Sawa N Oguro M 187918865720182996241710.2169/internalmedicine.0131-17PMC 6064702 · doi ↗ · pubmed ↗
- 4Non-hepatitis virus associated mixed essential cryoglobulinemia Kidney Int Annear NM Cook HT Atkins M 161164772010 https://pubmed.ncbi.nlm.nih.gov/19890273/1989027310.1038/ki.2009.416 · doi ↗ · pubmed ↗
- 5Clinicopathological spectrum of cryoglobulinemic glomerulonephritis without evidence of autoimmunity disorders: a retrospective study from a single institute of China Kidney Dis (Basel) Zhang X Yu XJ An CW 253263820223570270410.1159/000522537 PMC 9149548 · doi ↗ · pubmed ↗
- 6Cryoglobulinemic membranoproliferative glomerulonephritis associated with mucosaassociated lymphoid tissue lymphoma treated with rituximab Clin Nephrol Case Stud Ha AY Noronha N Gleason P 1442016 https://pmc.ncbi.nlm.nih.gov/articles/PMC 5437996/2904313410.5414/CNCS 108740 PMC 5437996 · doi ↗ · pubmed ↗
- 7Cryoglobulinemic vasculitis and membranoproliferative glomerulonephritis in a patient with cured virus C infection Nefrologia (Engl Ed) Sagrado EC Cordón CM González AS 295297442024 https://pubmed.ncbi.nlm.nih.gov/38631963/3863196310.1016/j.nefroe.2024.03.018 · doi ↗ · pubmed ↗