Nanotechnology-Enhanced Materials and Smart Implants in General Surgery: A Systematic Review of Human Clinical Outcomes
Abdulkreem Al-Juhani, Rodan Desoky, Norah Almutiri, Fayza Akil, Ghadeer M Almutawah, Faisal Alzahrani, Yahya M Alanazi, Hadeel A Al Mohammed, Mahmoud S Desoky

TL;DR
This systematic review evaluates how nanotechnology-enhanced materials and smart implants affect clinical outcomes in general surgery, finding them promising for infection prevention and cancer staging.
Contribution
The study systematically reviews human clinical outcomes of nanotechnology-enhanced materials and smart implants in general surgery, comparing them to conventional methods.
Findings
Silver-based topical creams improved wound healing and bacterial clearance.
Carbon nanoparticle suspensions enhanced lymph node detection in cancer staging.
Adverse effects of these technologies were minimal or absent.
Abstract
Nanotechnology-enhanced materials and smart implants are emerging technologies that have shown promise in addressing various challenges in general surgery, including infection management, oncologic staging, and complication monitoring. In this systematic review, we aimed to examine the safety and efficacy of these technologies compared with conventional methods in patients undergoing general surgical procedures. A comprehensive search was conducted in MEDLINE (via PubMed), Embase, Scopus, Web of Science, the Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, WHO ICTRP, IEEE Xplore/Inspec, and Google Scholar according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, using standardized keywords related to nanotechnology, surgery, and clinical outcomes. The included studies were categorized according to intervention class and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
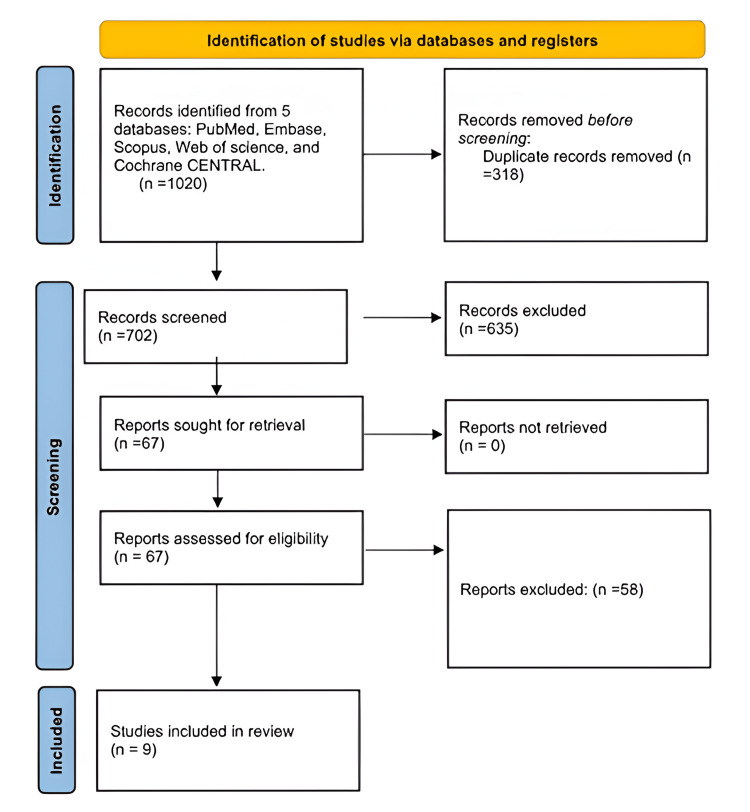 Figure 1
Figure 1| PICO element | Scope | Keywords/synonyms/MeSH terms |
| Population (P) | Patients undergoing general surgery (adults or children) - limited to general/abdominal surgery | Keywords: “general surgery” OR “abdominal surgery” OR “gastrointestinal surgery” OR “hernia repair” OR “soft tissue resection” OR “laparotomy” OR “laparoscopic surgery”. MeSH: “General Surgery”[Mesh] OR “Abdominal Surgery”[Mesh] OR “Digestive System Surgical Procedures”[Mesh] |
| Intervention (I) | Nanotechnology-enhanced surgical materials, devices, smart implants, nanoparticle therapies, or smart dressings | Keywords: nanotechnology OR nanomaterials OR nanoparticles OR “nano-enhanced” OR “nanostructured biomaterials” OR “antimicrobial coating” OR “nanoparticle-coated mesh” OR “smart implant” OR biosensor OR “smart device” OR “smart wound dressing” OR “nano-drug delivery”. MeSH: “Nanotechnology”[Mesh] OR “Nanostructures”[Mesh] OR “Nanoparticles”[Mesh] OR “Biomaterials”[Mesh] OR “Drug Delivery Systems”[Mesh] |
| Comparator (C) | Conventional surgical materials or standard surgical care | Keywords: “standard care” OR “conventional mesh” OR “standard surgical materials” OR “routine practice” OR “traditional implant”. MeSH: “Surgical Procedures, Operative”[Mesh] OR “Standard of Care”[Mesh] |
| Outcomes (O) | Clinical patient outcomes, including infection rates, wound healing, implant success or failure, complication detection, and morbidity or recovery | Keywords: “surgical site infection” OR “postoperative infection” OR “wound healing” OR “wound complication” OR “mesh failure” OR “implant failure” OR “hernia recurrence” OR “complication detection” OR “anastomotic leak” OR “patient outcome” OR morbidity OR recovery. MeSH: “Surgical Wound Infection”[Mesh] OR “Wound Healing”[Mesh] OR “Treatment Outcome”[Mesh] OR “Postoperative Complications”[Mesh] |
| Study (year) | Setting/population | Design | N (analyzed) | Intervention (class) | Comparator | Primary outcome(s) | Follow up |
|
Pathi et al. (2024) [ | Infected wounds (mixed) | RCT, open-label, parallel | 86 (43 vs. 43) | Silver nanoparticle topical cream (antimicrobial nanotech) | Mupirocin | Bacterial clearance (day 5); complete wound healing (day 28) | 28 days |
|
Kosugi et al. (2024) [ | Elective GI surgery incisions | RCT | 865 (427 vs. 438) | Aquacel Ag Hydrofiber (ionic silver dressing) | Film dressing | Superficial SSI ≤30 days (UMIN 000043081) | 30 days |
|
Zhao et al. (2023) [ | Papillary thyroid cancer; thyroidectomy (UL and TT subgroups) | RCT, multicenter, blank-controlled | 569 randomized | CNS tracer | Control (no tracer) | PTH; total LNs; tiny LNs; parathyroid recognition/retention; RLN | Intra-op; POD1; 1 mo |
|
Tian et al. (2025) [ | Resectable gastric cancer (cT1-4a N0/+ M0) | RCT, phase 3, open-label | 96 randomized; 90 mITT (46 vs. 44) | CNSI tracer (pre-op endoscopic injection) | ICG fluorescence tracer | Retrieved LNs (primary); micro LNs; diagnostic value; 3 y DFS/OS planned | 30-day morbidity; long-term planned |
|
Olona et al. (2025) [ | Incisional hernia with clean-contaminated wounds (ostomy reversal/bowel resection) | Case series, retrospective vs. matched historical controls | 12 (silver mesh) vs. 11 (polypropylene) | Silver ion-impregnated polypropylene mesh | Conventional polypropylene mesh | SSI; morbidity; mesh explant | Discharge; 30 days; 12 mo |
|
Jessernig et al. (2024) [ | GI surgery patients - drain fluid samples | Diagnostic evaluation of clinical samples | 32 samples | Naked-eye macromolecular network sensors (smart biosensor) | Reference AL status | Diagnostic accuracy (ROC AUC) for early AL | Perioperative samples |
|
Vidya et al. (2023) [ | Early breast cancer - SLNB | Prospective multicenter comparative | 107 | SPIO magnetic tracer (Sienna+) | Tc 99m ± blue dye | SLN identification rate; non-inferiority | Perioperative |
|
Alvarado et al. (2019) [ | Early breast cancer - SLNB | Prospective multicenter non-inferiority | 146 | SPIO magnetic tracer (Magtrace™) | Tc 99m + blue dye | SLN identification; non-inferiority margin | Perioperative |
|
Zhang et al. (2018) [ | Early breast cancer - SLNB | Retrospective single-center cohort | 332 | CNS tracer | ALND verification subset | SLN identification; diagnostic accuracy metrics | Perioperative |
| Study (design; n) | Population/procedure | Primary effect (quantitative) | Secondary findings (concise) | Safety/AEs | Key limitations |
|
Pathi et al. (2024) [ | Infected wounds (mixed etiologies); topical silver nanoparticle cream vs. mupirocin | Bacterial clearance at day 5: 86% vs. 65.1% (p = 0.023). Complete healing by day 28: 81.4% vs. 37.2% (p ≤ 0.001) | Faster wound improvement across visits (Bates-Jensen tool) reported | No local/systemic AEs observed in either arm | Single-center; open-label; co-interventions (systemic antibiotics) allowed; short (28-day) follow-up |
|
Kosugi et al. (2024) [ | Elective GI surgery; Aquacel Ag Hydrofiber vs. film dressing | Superficial SSI ≤30 d: 6.8% vs. 11.4% (p = 0.019); adjusted OR 0.60 (95% CI 0.37-0.99; p = 0.044) | Benefit concentrated in the lower GI subgroup (p = 0.042); no difference in the upper GI subgroup | AEs not detailed in abstract; routine peri-op antibiotics standardized (protocol in full text). No safety signal noted | Single-hospital RCT; dressing vs. film only; outcome limited to superficial SSI; blinding not feasible |
|
Zhao et al. (2023) [ | Papillary thyroid cancer; thyroidectomy; CNPs (CNS) vs. control | UL subgroup: ↑ total LNs (p < 0.0001) and ↑ tiny LNs (p = 0.0268). TT subgroup: higher 1-month PTH with CNS (p = 0.0368) | No significant differences in serum Ca²⁺; parathyroid preservation and RLN injury rates similar; RLN protection assessed as secondary | No drug-related AEs or injection complications recorded | Endpoint heterogeneity across UL vs. TT; surgeon blinding impossible; clinical significance of “tiny LNs” yield requires context |
|
Tian et al. (2025) [ | Radical gastrectomy; CNSI vs. ICG tracer | Retrieved LNs (mean): 69.8 vs. 53.6 (p < 0.001). Micro LNs: 19.9 vs. 11.6 (p = 0.001) | Diagnostic metrics for metastasis: higher sensitivity for micro LNs with CNSI; workflow note - LN sorting faster with CNSI vs. NIR ICG | 30-day complications: 10.9% vs. 11.4% (p = 0.94); detailed breakdown shows no mortality; no tracer injection complications | Open-label; modest sample; short-term outcomes (DFS/OS planned but not yet available); device/platform differences (robotic NIR) may confound |
|
Olona et al. (2025) [ | Clean-contaminated incisional hernia repair; silver-impregnated polypropylene mesh | SSI: 0/12 vs. 3/11 (27.3%) in prior series; p = 0.052 (borderline). Explants: 0 | No significant differences in other follow-up variables; mixed repair techniques (mostly retromuscular) | No SSI and no explants in silver mesh cohort over ~12-month mean follow-up; specific AEs otherwise NR in abstract | Small, single-center, nonrandomized; historical comparator; short follow-up; potential selection/surgeon bias |
|
Jessernig et al. (2024) [ | Post-op GI surgery; visible, non-electronic macromolecular network sensors for enzyme leak detection | ROC AUC for AL detection: 1.0 on clinical samples (proof of concept) | Continuous bedside monitoring concept; naked-eye color shift for amylase/protease signature | Not applicable (no patient implantation/intervention in this study); COI: inventorship on patent declared | Early-phase diagnostic work; small sample; clinical impact (time to detection, outcomes) not yet tested in trials |
|
Vidya et al. (2023) [ | Early breast cancer; SLNB; SPIO vs. radioisotope ± blue dye | Per-patient SLN detection: 98.13% (SPIO) vs. 92.26% (standard). Per-node: 93.07% vs. 96.53%. All 31 node-positive cases detected by both | Demonstrated feasibility; concordance shown | AEs NR in abstract (focus on detection performance) | Not randomized head-to-head (both tracers used sequentially in the same patients); detection emphasis; limited safety reporting in the abstract |
|
Alvarado et al. (2019) [ | Early breast cancer; SLNB; Magtrace (SPIO) vs. technetium-99m + blue dye | Per-patient detection: 99.3% vs. 98.6%. Per-node: 94.3% vs. 93.5%. Δ 0.8%, 95% CI lower bound −2.1% → met non-inferiority | All malignant nodes found by standard were identified by SPIO; high concordance | AEs NR in abstract (performance trial) | Open-label procedural trial; safety outcomes not detailed in abstract; no long-term outcomes |
|
Zhang et al. (2018) [ | Early breast cancer; SLNB; CNS | SLN identification: 99.1% (329/332). Sensitivity: 95.9%. Specificity: 100%. FNR: 4.1% | Mean SLNs retrieved: 2.6; high diagnostic accuracy comparable to standards | Anaphylaxis, necrosis, local inflammation: 0; skin staining: 41.9% at median 13.2-month follow-up | Single-center retrospective; no RI/blue dye control arm; cosmetic staining common |
| Study | R | D | M | O | S | Overall |
|
Pathi et al. (2024) [ | Some concerns | Some concerns | Low | Some concerns | Some concerns | Some concerns |
|
Kosugi et al. (2024) [ | Low | Some concerns | Low | Low | Some concerns | Some concerns |
|
Zhao et al. (2023) [ | Low | Some concerns | Low | Some concerns | Some concerns | Some concerns |
|
Tian et al. (2025) [ | Low | Some concerns | Some concerns | Some concerns | Some concerns | Some concerns |
| Study | C | S | Cl | D | M | O | R | Overall |
|
Olona et al. (2025) [ | Serious | Serious | Low | Moderate | Moderate | Moderate | Moderate | Serious |
| Study | Risk of Bias - PS | IT | RS | FT | Overall RoB | Applicability - PS A | IT A | RS A |
|
Jessernig et al. (2024) [ | High | Unclear | Unclear | Unclear | High | High | High | Unclear |
|
Vidya et al. (2023) [ | Low | Low | Low | Low | Low | Low | Low | Low |
|
Alvarado et al. (2019) [ | Low | Low | Low | Low | Low | Low | Low | Low |
|
Zhang et al. (2018) [ | High | Low | Low | Unclear | High | Low | Low | Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Anxiety and Anesthesia Techniques · Medical and Biological Ozone Research
Introduction and background
Despite significant medical advances in general surgery, several clinical challenges persist. Three of the most important issues in the field today are accurate lymphatic staging, surgical site infections (SSIs), and delayed recognition of early postoperative complications [1,2]. SSIs remain among the most common health care-associated infections and are linked to increased length of hospital stay, higher health care costs, and greater morbidity. The growing threat of antimicrobial resistance (AMR) adds urgency to this issue, as bacterial resistance accounted for approximately 1.27 million deaths in 2019, compromising the safety of preoperative prophylaxis [3,4].
At the same time, postoperative complications such as anastomotic leakage are often detected late because of nonspecific clinical signs and delayed imaging. Similarly, accurate lymphatic staging still relies on radiotracers with or without blue dye mapping; however, these standards involve radiation exposure, logistical complexity, and limited accessibility [1,4]. Collectively, these gaps highlight the need for practical innovations, smarter materials, and advanced devices to prevent infections, identify complications earlier, and assist in surgical guidance.
Current standardized care protocols for pre- and postoperative infection prevention depend on timely antibiotic administration, antiseptic measures, and temperature and glucose control. However, the increasing reliance on antibiotics is undermined by AMR, and conventional wound dressings demonstrate variable efficacy in SSI prevention and wound healing. A recent multicenter clinical trial found that ionic-silver hydrofiber dressings reduced superficial SSIs compared with film dressings [5]. Another randomized trial reported improved healing and faster microbial clearance with silver nanoparticles [6].
Nodal mapping and detection play a crucial role in staging and treatment planning, particularly in breast cancer, where the current benchmark involves radioisotopes with or without blue dye. However, regulatory requirements, radiation exposure, and limited access can delay or complicate care. Nonradioactive tracers have recently emerged as viable alternatives: a multicenter noninferiority trial demonstrated that superparamagnetic iron oxide (SPIO) tracers are a practical substitute that avoids radiation exposure [7,8]. Carbon nanoparticles (CNPs) have also enhanced lymph node harvest and micrometastatic node detection, and in thyroid surgery, they have been shown to improve parathyroid preservation and nodal retrieval [9,10].
Early detection of postoperative complications such as anastomotic leaks remains a challenge because clinicians must often rely on nonspecific signs before ordering targeted imaging. This delay frequently leads to reinterventions and increases the risk of sepsis, morbidity, and prolonged hospitalization [4,11]. Novel bedside biosensors have shown promise as a complementary diagnostic pathway, and a non-electronic macromolecular network drain sensor has demonstrated excellent diagnostic performance for leak detection, although it has not yet been standardized [12].
Nanotechnology-enhanced materials and smart implants have been developed to address these clinical challenges while offering improved safety profiles. Several human studies have demonstrated their potential to reduce SSIs (e.g., ionic-silver hydrofiber dressings), replace or supplement radioisotopes for nodal mapping (e.g., SPIO and CNPs), and enable real-time perioperative monitoring (e.g., biosensors). However, existing evidence remains heterogeneous across procedures, comparators, and follow-up durations. In this review, we aim to consolidate current clinical findings to evaluate the safety, effectiveness, and translational potential of these emerging technologies in surgical practice.
Review
Methodology
This review was designed according to a predefined methodology consistent with the Preferred Reporting Items for Systematic reviews and Meta-Analyses Protocols (PRISMA-P) and is reported in accordance with the PRISMA 2020 guidelines (Figure 1).
PRISMA flow diagramPRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses
The eligibility criteria (PICO) are summarized in Table 1. The population included human patients of any age undergoing general surgical procedures, such as gastrointestinal surgery, hernia repair, endocrine or thyroid surgery, and soft-tissue treatments. The interventions comprised nanotechnology-enhanced materials or “smart” implants and devices utilized intraoperatively or perioperatively. These included nano-coated meshes or implants, nano-structured biomaterials, sensor-enabled drains or dressings, nanoparticle-mediated therapeutic drugs, and nano-tracers for surgical navigation. The comparators were conventional materials or devices and standard care that lacked nano-enhancement or intelligent features. The outcomes evaluated included at least one patient-relevant endpoint, such as surgical-site or implant infection, wound healing duration or complications, implant or device failure, identification or time-to-detection of complications, need for reoperation, and length of hospitalization.
Study designs included randomized controlled trials, controlled clinical trials, and comparative observational studies. Conference abstracts were admissible if they provided adequate outcome data. Exclusion criteria comprised non-human studies; specialties unrelated to general surgery that did not provide extractable general surgery data; single-arm reports without a relevant comparator; and studies that solely presented surrogate or device performance indicators. No restrictions regarding publication date or language were applied.
Sources of information and search methodology: The search was conducted through MEDLINE (via PubMed), Embase, Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials, from database inception to the final search date. To capture transdisciplinary and grey literature, additional searches were performed in ClinicalTrials.gov, WHO ICTRP, IEEE Xplore/Inspec, Google Scholar, and major conference proceedings. Reference lists and forward citations of the included studies were also examined. Search strategies, developed in collaboration with a librarian, integrated controlled vocabulary and keywords across three domains: nanotechnology/smart materials, surgery, and clinical outcomes.
Selection of Studies and Management of Data
Duplicate studies were removed using a reference manager before importing records into a screening platform. Two reviewers independently screened titles and abstracts, followed by full-text assessments based on the eligibility criteria. Any discrepancies were resolved through consensus or adjudication by a third reviewer. The rationale for full-text exclusions was documented, and study progression was illustrated in a PRISMA flow diagram. A version-controlled repository maintained the methodology, screening forms, data extraction templates, and audit logs.
Data extraction and components: Two reviewers independently extracted data using a piloted, standardized form. Extracted data included study characteristics (authors, year, country, setting, funding, and conflicts of interest); study design (trial or observational, single-center, or multicenter), follow-up duration; population details (age, sex, indications, comorbidities, and procedure type); intervention details (nano feature, material or device type, coating composition, particle characteristics, sensor type, dose or exposure, timing, and implementation); comparator details; outcome definitions and measurement windows; and numerical results (events and denominators for dichotomous outcomes; means and standard deviations or medians and interquartile ranges for continuous outcomes; and HRs for time-to-event outcomes). Adverse events were also recorded. Authors were contacted for clarification or to obtain missing data when necessary.
Risk of Bias
Two reviewers independently assessed the risk of bias using RoB 2 for randomized trials and ROBINS-I for nonrandomized studies (or the Newcastle-Ottawa Scale when applicable). Domain-level and overall assessments informed interpretation and sensitivity analyses. The certainty of evidence for key outcomes was evaluated using GRADE, considering study limitations, inconsistency, indirectness, imprecision, and potential publication bias.
No quantitative aggregation was conducted. Instead, a systematic narrative synthesis was performed, categorizing studies by intervention class (e.g., antimicrobial nano-coatings, nano-tracers, sensor-enabled devices, and nanoparticle administration) and by procedural type. For each outcome, the direction and magnitude of effects were described using the estimates from each study (risk or ORs, mean differences, and HRs with 95% CIs when available), explicitly avoiding vote counting based on statistical significance. In cases of heterogeneous outcome measures, ranges and medians were reported, correlating findings with study design, risk of bias, and clinical context. Planned stratified summaries (e.g., adult versus pediatric populations; clean versus contaminated operations; open versus minimally invasive procedures; and study design or risk-of-bias strata) and sensitivity considerations (e.g., abstracts-only reports) were addressed narratively. Funnel plots and tests for small-study effects were not conducted.
Ethics and Transparency
This review synthesizes previously published data; therefore, ethics approval was not required. Comprehensive search methods, a PRISMA flow diagram, risk-of-bias assessments, and, where permissible, de-identified data extraction files and analytical materials were included to enhance reproducibility.
Results
Overview of the Evidence
Nine studies met the inclusion criteria, comprising four randomized controlled trials, two prospective multicenter comparative studies, one retrospective cohort study, one case series with historical controls, and one diagnostic validation study. These studies addressed three main indications: infection prevention (silver-based materials), lymphatic mapping and oncologic staging (CNPs and SPIO), and early complication detection (macromolecular network biosensor). In total, 2,250 participants or samples were included across studies (infection prevention: 974; mapping/staging: 1,244; sensing: 32 drain-fluid samples). Variability in interventions, comparators, and outcome assessment periods precluded meta-analysis; therefore, results were synthesized narratively and organized by indication (Table 2).
Infection Prevention
Two randomized studies and one case series evaluated silver-based interventions for infection prevention. In an RCT involving gastrointestinal incisions (n = 865), an ionic-silver hydrofiber dressing significantly reduced superficial SSIs within 30 days compared with a standard film dressing (6.8% vs. 11.4%; adjusted OR, 0.60; 95% CI, 0.37-0.99), representing an absolute risk reduction of 4.6% (46 per 1,000). In another trial of infected wounds (n = 86), a topical silver nanoparticle cream demonstrated superior bacterial clearance by day 5 (86% vs. 65.1%) and complete wound healing by day 28 (81.4% vs. 37.2%) compared with the control. A smaller clean-contaminated incisional hernia series (12 vs. 11) reported no SSIs (0/12) with silver-impregnated mesh, in contrast to 3/11 cases (27.3%) in the historical control group (p = 0.052); no mesh explants were required. None of the studies reported device- or drug-related adverse effects. The summarized findings are presented in Table 3.
Lymphatic Mapping and Oncologic Staging
The evidence base comprised two randomized controlled trials (thyroidectomy and radical gastrectomy), two prospective multicenter studies on breast cancer sentinel lymph node biopsy (SLNB) comparing SPIO with radioisotope mapping (with or without blue dye), and one retrospective cohort study evaluating CNS in breast cancer.
In the FUTURE 01 trial (mITT n = 90) for radical gastrectomy, injection of CNP suspension (CNS) increased total lymph node yield (mean 69.8 vs. 53.6) and micro lymph node count (19.9 vs. 11.6), while 30-day postoperative complication rates were comparable between groups (10.9% vs. 11.4%). In thyroidectomy (n = 569), CNS improved nodal retrieval in unilateral lobectomy subanalyses and was associated with higher one-month postoperative PTH levels after total thyroidectomy; serum calcium concentrations and RLN injury rates were unchanged in the reported abstract.
For breast cancer SLNB, two prospective multicenter RCTs, such as SMART (n = 107) and SentimagIC (n = 146), evaluated SPIO tracers. Both studies demonstrated non-inferiority to conventional radioisotope-based mapping, achieving per-patient SLN detection rates of 98.1% versus 92.3% (SMART) and 99.3% versus 98.6% (SentimagIC). All malignant nodes identified through standard techniques were also detected by SPIO.
A retrospective cohort of breast cancer patients (n = 332) using CNS for SLNB reported SLN identification in 99.1% of cases, sensitivity of 95.9%, specificity of 100%, and a false negative rate of 4.1%. Skin staining occurred in 41.9% of patients at a median of approximately 13 months post-procedure. No significant tracer-related adverse effects were reported in the mapping studies.
Early Complication Sensing
A diagnostic validation study (n = 32 clinical drain samples) employing a visual, non-electronic macromolecular network sensor achieved an AUC of 1.00 for detecting biochemical signatures of anastomotic leaks. Patient-level clinical outcomes such as time-to-detection, reoperation, and infection rates were not evaluated. No device-related adverse events were reported in this preliminary investigation (Table 3).
Safety
Across studies, no significant adverse effects were associated with silver dressings or creams, CNS/CNSI injections, or SPIO tracers. The only recurring safety issue was cosmetic skin discoloration related to CNS use in breast SLNB, observed in approximately 42% of cases. Postoperative morbidity within 30 days did not differ significantly between CNSI and ICG in gastrectomy procedures (Table 3).
Risk of Bias
All four randomized trials were judged as having “some concerns” overall according to the RoB 2 tool. The non-randomized silver-mesh series was rated “serious” overall risk using ROBINS-I. Diagnostic accuracy evaluations using QUADAS-2 classified the SPIO studies (SMART, SentimagIC) as “low risk,” whereas the CNS breast cohort and the macromolecular sensor study were both rated “high risk.” These risk-of-bias assessments warrant cautious interpretation, particularly for non-randomized and early-phase diagnostic studies. The detailed assessments are presented in Table 4, Table 5, and Table 6.
Synthesis Statement
The collective evidence supports the use of silver-based approaches for reducing superficial SSIs and accelerating wound healing in selected settings. It also confirms that SPIO is a non-inferior alternative to radioisotopes for sentinel lymph node mapping and highlights the benefits of CNPs in improving nodal yield and preserving parathyroid function, without introducing new safety concerns. Biosensor technology shows excellent diagnostic accuracy; however, further clinical studies are required to establish its impact on patient-relevant outcomes.
Discussion
Our systematic review aimed to evaluate the safety, effectiveness, and therapeutic potential of nanotechnology-enhanced materials and smart implants in general surgery based on human clinical outcomes. The nine included clinical studies demonstrated the significance of nanotechnology across diverse surgical applications. The evidence showed that silver-based materials markedly reduced superficial SSIs and promoted wound healing [5,6,13-16]. SPIO demonstrated comparable effectiveness to conventional mapping techniques [17-20]. CNSs in SLNB showed high identification rates with no significant adverse effects [9,15,16]. One preliminary study using a non-electronic macromolecular network sensor showed the potential to identify anastomotic leakage. Collectively, these findings highlight the promising benefits of these technologies for improving human clinical outcomes in the future [21].
Regarding the effectiveness of silver-based technology, the literature has shown encouraging results. Metal-based nanoparticles possess strong antibacterial properties, providing high potential for treating bacterial infections [22]. A recent randomized clinical trial comparing mupirocin with Kadermin, a silver nanoparticle-based cream, reported significant differences in wound healing and bacterial clearance of culture-positive infected wounds [23]. Similarly, when compared with standard film dressings, Aquacel Ag Hydrofiber dressings reduced the incidence of superficial SSIs by approximately 40% [24]. Metal-based nanoparticles thus show considerable promise as antibacterial agents for infection management [25].
Previous single-center and sample-based studies have demonstrated that CNPs can enhance lymph node detection in colorectal cancer [25,26] and papillary thyroid cancer [27,28]. In contrast, another study found no significant benefit in lymph node dissection when using CNPs [29]. However, our findings suggest that CNS may aid in detecting a higher number of lymph nodes, particularly micrometastatic or small lymph nodes, in papillary thyroid cancer, potentially enabling more radical dissections. Aside from minor skin staining noted in one study, CNS demonstrated comparable efficacy to traditional methods for lymph node retrieval and improved parathyroid preservation.
Two studies reported that SPIO-guided SLNB is a viable alternative for early breast cancer, achieving identification rates comparable to the standard dual technique using radioisotopes and blue dye. This suggests SPIO could safely replace the gold standard for sentinel lymph node mapping [30]. The use of SPIO during mastectomy for uncomplicated conditions also spared most patients unnecessary axillary surgery and its associated morbidities [31]. Multiple studies utilizing various tools for early detection of anastomotic leaks underscore the importance of timely diagnosis and support the potential value of innovative biosensor approaches [32].
Despite the small sample sizes, short follow-up durations, and heterogeneous outcomes among included studies, our systematic review represents a preliminary but important step in assessing the clinical outcomes of nanotechnology-enhanced materials and smart implants in general surgical practice. Strengths of this review include adherence to PRISMA 2020 guidelines, the use of multiple reviewers, standardized data collection, and a structured evaluation of bias. Additionally, our exclusive focus on human clinical studies enhances the practical relevance of the findings.
One of the greatest challenges in modern medicine is the rapid emergence of AMR among common pathogens [32]. In this context, silver-based topical therapies and dressings offer a promising alternative, providing broad-spectrum antibacterial activity and the potential to reduce infection rates and healthcare utilization. Both CNS and SPIO also serve as effective alternatives to traditional radioisotopes and dyes. CNS demonstrated clear benefits, including improved micrometastatic lymph node retrieval, while SPIO yielded outcomes comparable to conventional radioisotopes, with the added advantage of eliminating radiation exposure.
Although still in preliminary stages, biosensor technologies represent a major shift toward real-time, early detection of postoperative complications, including anastomotic leakage. Such advancements may enable earlier intervention and potentially reduce morbidity. However, further large-scale, multicenter randomized controlled trials with extended follow-up periods are required to evaluate delayed complications. Specifically, for biosensors, future prospective trials should emphasize patient-centered outcomes such as leak detection timing, reoperation rates, and postoperative morbidity.
Conclusions
The findings underscore that nanotechnology-enhanced materials and intelligent implants hold substantial potential to transform general surgical practice. These innovations demonstrate promise in three key areas: reducing the risk of SSIs, improving the precision of lymphatic mapping in thyroid, gastric, and breast procedures, and enabling early detection of postoperative complications. The reviewed studies indicate that these approaches can produce outcomes comparable to or exceeding current standards, with few adverse effects reported. However, existing trials remain limited by small sample sizes, short follow-up durations, and heterogeneity in comparators and outcome measures. Therefore, large-scale, multicenter studies with extended follow-up are essential to confirm their safety, assess long-term clinical benefits, and establish standardized protocols for widespread clinical implementation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Guidelines for the Prevention of Surgical Site Infection Geneva World Health Organization 2018 https://www.ncbi.nlm.nih.gov/books/NBK 536404/30689333 · pubmed ↗
- 2Enhanced recovery after surgery guidelines and hospital length of stay, readmission, complications, and mortality: a meta-analysis of randomized clinical trials JAMA Netw Open Sauro KM Smith C Ibadin S 07202410.1001/jamanetworkopen.2024.17310 PMC 1119562138888922 · doi ↗ · pubmed ↗
- 3Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis Lancet 62965539920223506570210.1016/S 0140-6736(21)02724-0PMC 8841637 · doi ↗ · pubmed ↗
- 4Management of anastomotic leakage after rectal surgery: a review article J Gastrointest Oncol Tsai YY Chen WT 122912371020193194994410.21037/jgo.2019.07.07PMC 6955017 · doi ↗ · pubmed ↗
- 5The Nordic Senti Mag trial: a comparison of super paramagnetic iron oxide (SPIO) nanoparticles versus Tc 99 and patent blue in the detection of sentinel node (SN) in patients with breast cancer and a meta-analysis of earlier studies Breast Cancer Res Treat Karakatsanis A Christiansen PM Fischer L 28129415720162711715810.1007/s 10549-016-3809-9PMC 4875068 · doi ↗ · pubmed ↗
- 6The role of carbon nanoparticles in lymph node dissection and parathyroid gland preservation during surgery for thyroid cancer: a systematic review and meta-analysis Cancers (Basel) Koimtzis G Stefanopoulos L Alexandrou V 40161420223601100910.3390/cancers 14164016 PMC 9407010 · doi ↗ · pubmed ↗
- 7Drainage fluid amylase as a biomarker for the detection of anastomotic leakage after low anterior resection of rectal cancer: a two-center study Cancer Diagn Progn Ishiyama Y Hirano Y Yamato M 80280742024 https://www.cancerdiagnosisprognosis.org/article/449/drainage-fluid-amylase-as-a-biomarker-for-the-detection-of-anastomotic-leakage-after-low-anterior-resection-of-rectal-cancer-a-two-center-study 3950260510.21873/cdp.10399 PMC 11534043 · doi ↗ · pubmed ↗
- 8Emergent crisis of antibiotic resistance: a silent pandemic threat to 21st century Microb Pathog Akram F Imtiaz M Haq IU 10592317420233652603510.1016/j.micpath.2022.105923 · doi ↗ · pubmed ↗